Crossland G, Bath A. Bismuth iodoform paraffin paste: a review. J Laryngol Otol. 2011; 125:891-895
Balasubramanian T, Bleacher L. BIPP Pack a revisit. J Otolaryngol. 2011; 1:1-2
Gurd FB, McKim LH. BIPP and liquid paraffin treatment of war and civilian wounds. Ann Surg. 1941; 113:987-1000
Agrawal R, Sangle A, Vyawahare A. Bismuth Iodoform and paraffin paste a boon in treatment of keratocystic odontogenic tumor: a case report. J Dent Med Res. 2014; 1:32-35
O'Connor AF, Freeland AP, Heal DJ, Rossouw DS. Iodoform toxicity following the use of BIPP: a potential hazard. J Laryngol Otol. 1977; 91:903-907
Charlu AP Kumar S, Chacko R. Qualitative evaluation of ‘BIPP dressing’ for intraoral mucosal defect. J Clin Diagn Res. 2018; 12:11-14
Coulson CJ, Pothier DD, Lai P, Rutka JA. Bismuth iodoform paraffin paste hypersensitivity reactions in mastoid cavities following isolation of mucosal lining: a series of 587 patients. J Laryngol Otol. 2012; 126:240-243
Atwal A, Cousin GC. Bismuth toxicity in patients treated with bismuth iodoform paraffin packs. Br J Oral Maxillofac Surg. 2016; 54:111-112
Hartley C, Ng KL, Jackson A. CT and MR appearance of otolaryngologic packing materials. AJNR Am J Neuroradiol. 1995; 16:1697-1702
Nigam A, Allwood MC. BIPP – how does it work?. Clin Otolaryngol Allied Sci. 1990; 15:173-175
Freedman M, Stassen LF. Commonly used topical oral wound dressing materials in dental and surgical practice – a literature review. J Ir Dent Assoc. 2013; 59:190-195
Rastogi S, Modi M, Sathian B. The efficacy of collagen membrane as a biodegradable wound dressing material for surgical defects of oral mucosa: a prospective study. J Oral Maxillofac Surg. 2009; 67:1600-1606
Kumar EV, Chembolu N, Patiola BR A collagen membrane – a biologic mucosal substitute for intraoral denuded areas. Int J Sci Res. 2017; 6:316-320
Bigliardi PL. Povidone iodine in wound healing: a review of current concepts and practices. Int J Surg. 2017; 44:260-268
Haq J, Siddiqui S, McGurk M. The use of Carnoy's solution following enucleation of ameloblastoma: ten year's experience. Br J Oral Maxillofac Surg. 2015; 53
Bismuth Iodoform Paraffin Paste: History, Uses and Alternatives in Oral and Maxillofacial Surgery Gurpreet Kaur Randhawa Richard M Graham Karanveer Singh Matharu Dental Update 2024 48:3, 707-709.
Authors
Gurpreet KaurRandhawa
BDS(Hons) MFDS, RCS(Ed)
Dental Core Trainee, North Manchester General Hospital
Bismuth iodoform paraffin paste (BIPP) continues to be widely used in dental/oral and maxillofacial/ENT surgery for surgical cavity packing and wound dressing where pressure, antisepsis and haemostasis is required. We present information on its history and uses, including historical use, constituents, uses in surgery, risks and considerations for deciding on its use. Although side effects and adverse reactions have been reported, these are rare.
CPD/Clinical Relevance: BIPP is commonly used in surgical procedures and an appreciation of its background, history, uses and side effects are important as well as an understanding of its alternatives.
Article
Bismuth iodoform paraffin paste (BIPP) is commonly used in dental and surgical applications as a wound dressing, for cavity packing, as well as in ear, nose and throat procedures, when pressure, antisepsis and/or haemostasis is required. It commonly comes in the form of a paste or impregnated sterile gauze (Figure 1).1 Clinicians also use BIPP paste dressing in a range of oral and maxillofacial surgical procedures.
Figure 1. BIPP-impregnated gauze.
History
BIPP was first used by Rutherford Morison in 1916 to dress soldiers' wounds.2 He found that when bismuth and iodoform were mixed with paraffin, it permitted a healing response and reduced infection rates. His recommendations were as follows:
Adequate exploration of the wound to remove foreign bodies and necrotic tissue;
Debridement with alcohol to dry tissues;
Application of BIPP.
Excess BIPP was then removed as incomplete removal of excess paste commonly resulted in failure.
This was described for use in World War I to treat gunshot wounds, and since then, BIPP has continued to be used as a wound packing material.3
Constituents and properties
BIPP is composed of two active ingredients: one-part bismuth subnitrate and two parts iodoform, plus one inactive ingredient: one part sterile liquid paraffin.
Bismuth is antiseptic and is responsible for shrinkage of bodily tissues. It also releases dilute nitric acid on hydrolysis, which stimulates an immune response. Bismuth has a half-life of 5 days in the body, but can remain in the kidney for longer.4
Tri-iodomethane (iodoform) has a distinctive colour and smell. It decomposes to release iodine, which is also an antiseptic.4 O'Connor et al found raised plasma iodine levels following its use in a maxillectomy cavity.5
Paraffin is added to BIPP as a lubricant to aid atraumatic placement and removal of the pack.4 Being non-active it has no other function. When added to gauze, BIPP makes the gauze impervious to blood and body fluids, therefore reducing the chance of surgical site infection.
In addition, BIPP exerts a drying effect on sites of application. It has been recommended that BIPP should be refrigerated and stored between 2° and 8°C and that its average shelf life is approximately 36 months.
Uses in surgery
Although BIPP does not initiate or promote wound healing, it does provide an environment for healing to occur4,6 and is used in dental, oral and maxillofacial surgery for a variety of uses, for example:
Nasal packing;
Topical dressing until closed wounds have healed, or a graft has taken;
To fill intra-oral mucosal defects such as cystic cavities;
Dento-alveolar surgery, eg dressing following exposure of unerupted teeth.
Agrawal et al4 used BIPP as a cavity packing agent following enucleation of a mandibular odontogenic keratocyst plus peripheral osteotomy and Carnoy's solution. This was a more conservative alternative to mandibular resection and flap reconstruction. The use of BIPP in the treatment of benign lesions (to minimize morbidity) has been encouraged; however, not often in established frank malignancies where resection and often reconstruction would be the most common treatment of choice.
Charlu et al6 studied the use of BIPP for intra-oral defects post excision of pre-cancerous lesions that were too large for primary closure. Healing took place under the BIPP by granulation tissue formation and muscosalization. In all cases, BIPP was an adequate intra-oral dressing. None of the patients suffered allergic reactions, patient compliance was acceptable and oral hygiene and feeding were unaffected. Compared to other grafting and reconstruction techniques, the use of BIPP can avoid donor-site morbidity and is easily placed and secured.
Risks and other considerations
Although BIPP continues to be regularly used in dental/oral and maxillofacial surgery, side effects have been reported.
Iodoform
The commonest side effect to BIPP is a type IV hypersensitivity reaction to iodoform7 in which an erythematous rash appears. Prolonged use of BIPP can also result in iodoform poisoning, which manifests as irritation of the eye, skin, gastric and respiratory surfaces.
Bismuth
The rarest reaction is encephalopathy due to bismuth toxicity. Neurotoxicity can occur because bismuth interferes with oxidative metabolism in the brain. Symptoms of toxicity include: headache, nausea, sore mouth and a blue-black bismuth line in the gingivae.4
Toxicity can also occur if large amounts of BIPP are used in contact with exposed bone, which leads to systemic absorption.
Paraffin
Liquid paraffin can be absorbed from wounds, causing granulomatous reactions. Prolonged use on wounds should be avoided. Although rare, sensitivity reactions and acne have been reported with topical use of white soft paraffin.8
Other considerations
Atwal and Cousin9 reported two cases of toxicity following the use of BIPP. One case was following marsupialization and decompression of an odontogenic keratocyst. In this case, the patient became fatigued, confused and reported memory loss. The second case occurred following use of BIPP in a hemimaxillectomy defect, following resection of a squamous cell carcinoma, in which the patient became increasingly confused. They suggest that absorption of BIPP could have been reduced by minimizing exposure and duration of contact with BIPP, and the use of an alternative dressing material.
BIPP can also result in renal failure as a result of bismuth absorption, therefore, its use is not recommended in patients with moderate to severe renal failure.
BIPP is radio-opaque due to its bismuth content and a radio-opaque marker strip within the gauze enables its radiographic detection if it becomes displaced.1 A case has been reported of BIPP-induced artefacts on computed tomography scans and, if possible, an alternative material should be used if these scans are required.10 On magnetic resonance imaging (MRI) scans, BIPP has imaging characteristics similar to muscle.10
In another study, Nigam and Allwood11 found that BIPP had negligible antibacterial properties against Staphylococcus aureus, Escherichia coli and Pseudomonas aeruginosa in vitro and no release of iodine was detected over a 4-week period. It is suggested that the antibacterial nature of BIPP may be due to the surgical debridement that is carried out before its application, but this is only in relation to these specific organisms.11
Alternatives to BIPP
Wound dressing
Whitehead's varnish has been used as an alternative to BIPP, although it is no longer available in the UK. Examples of its uses include: a dressing for skin-graft donor sites and a pack for cyst cavities. It contains iodoform, which acts as an antiseptic, and benzoic acid, which is a preservative and disinfectant. Whitehead's varnish can prevent post-operative infection and achieve haemostasis.12
There has been some research into the use of biodegradable collagen/skin membranes as a wound dressing for defects of the oral mucosa, for example Integra (Integra LifeSciences, USA). They have been shown to promote haemostasis, prevent infection, induce granulation tissue formation and allow rapid epithelialization of wound sites.13 This leads to reduced scarring and avoids a second surgical site.14
Antiseptic gauze, such as povidoneiodine (Betadine) soaked gauze can be used as an alternative to BIPP for wound dressing. Povidone-iodine gauze has a broad antimicrobial spectrum and is well tolerated.15
Alveogyl is often used to treat alveolar osteitis, commonly known as ‘dry socket’. It is comes in the form of a brown fibrous paste and, like BIPP, contains iodoform, which can reduce the bacterial load. Its other main ingredients are butamben, a local anaesthetic, and eugenol, an essential oil, which relieves post-operative pain.12 Alveogyl is not known to cause any side effects.
Zinc oxide-based materials
Zinc oxide is an alternative wound dressing material. It is combined with other materials to form a paste or cement. These materials are used to cover gingival tissues or extraction sockets.12
Coe-pack (GC, USA) is an example of a non-eugenol zinc oxide dressing material and is used after periodontal/oral surgery.
Oxidized regenerated cellulose
Oxidized regenerated cellulose is commonly used in extraction sockets to achieve haemostasis. It can also be used after harvesting bone from a donor site for grafting for haemostasis. The cellulose fibres act as a platform for platelet aggregation and haemostasis. An example of this material is Surgicel (Johnson and Johnson, USA). It is easy to use, can be cut to size and has antimicrobial activity against a number of pathogenic bacteria.
Carnoy's solution consists of chloroform, glacial acetic acid and ferric acid in an ethanol solvent. It is primarily used in conjunction with cyst enucleation of the jaws, for example odontogenic keratocysts, glandular odontogenic cysts and occasionally for ameloblastomas. It can either permit easier removal of the lining of these cysts if placed within the cyst, or is said to reduce the chances of daughter cyst growth/cyst recurrence in the cavity wall if used in the enucleated cavity.12 A 10-year retrospective study on the effect of Carnoy's solution with unicystic, solid and multicystic ameloblastomas, following enucleation, showed a low recurrence rate.16
Nasal packs
There are several alternatives to BIPP for nasal packing. Non-resorbable packs such as antiseptic povidone-iodine gauze or Merocel (Medtronic Inc, USA) can be used. Merocel is a compressed, dehydrated sponge composed of hydroxylated polyvinyl acetate that increases in size within the nasal cavity by absorbing saline or other fluid, in compressing blood vessels, resulting in haemostasis.
NasoPore (Stryker, USA) is a bioresorbable material containing foam that absorbs water. This supports the surrounding tissue, and provides pressure and haemostasis.
Precautions
Theoretically, iodine released from the iodoform in BIPP could pose a risk to patients with pre-existing thyroid disease. The release of iodine could exacerbate pre-existing hyperthyroidism and cause thyrotoxicosis; however, there have been no reports of this following use of BIPP.1 Excess iodine absorption in pregnant women could affect fetal thyroid development and function. BIPP should, therefore, be used with caution in these patients. However, further studies are required to assess the safety of BIPP in pregnant women. Iodine and bismuth are both excreted in breastmilk. It is not known whether bismuth causes harm to the newborn, but it is recommended that topical preparations of iodine are avoided in women who are breastfeeding. There is no evidence currently that BIPP interacts with other drugs.8
Case reports
The following cases demonstrate the use of BIPP in oral and maxillofacial surgical procedures.
Case 1: Le Fort II maxillary osteotomy and genioplasty
This patient had a post-operative chin wound dehiscence and infection, which was packed with BIPP (Figure 2). The pack was changed every 1–2 weeks for 6 weeks, until the mucosa/wound healed, the plate and screws were subsequently removed (Figure 3).
Figure 2. PA mandible showing wound dehiscence packed with BIPP, 6 weeks post-operatively.Figure 3. PA mandible 4 months post-operatively.
Case 2: amelobastoma (mandible)
This patient presented with a large cystic lesion of the mandible (Figure 4). The cyst was marsupialized and packed with BIPP (Figure 5), while pathology investigations were in process. The patient chose to continue with regular packing for 12 weeks until healing had occurred, and ultimately decided not to undergo ameloblastoma resection.
Figure 4. Pre-operative orthopantomogram of an ameloblastoma, right mandible.Figure 5. Post-operative orthopantomogram showing a cystic lesion the right mandible with BIPP packing in place after marsupialization of cystic lesion right mandible.
Case 3: dentigerous cyst associated with LL8
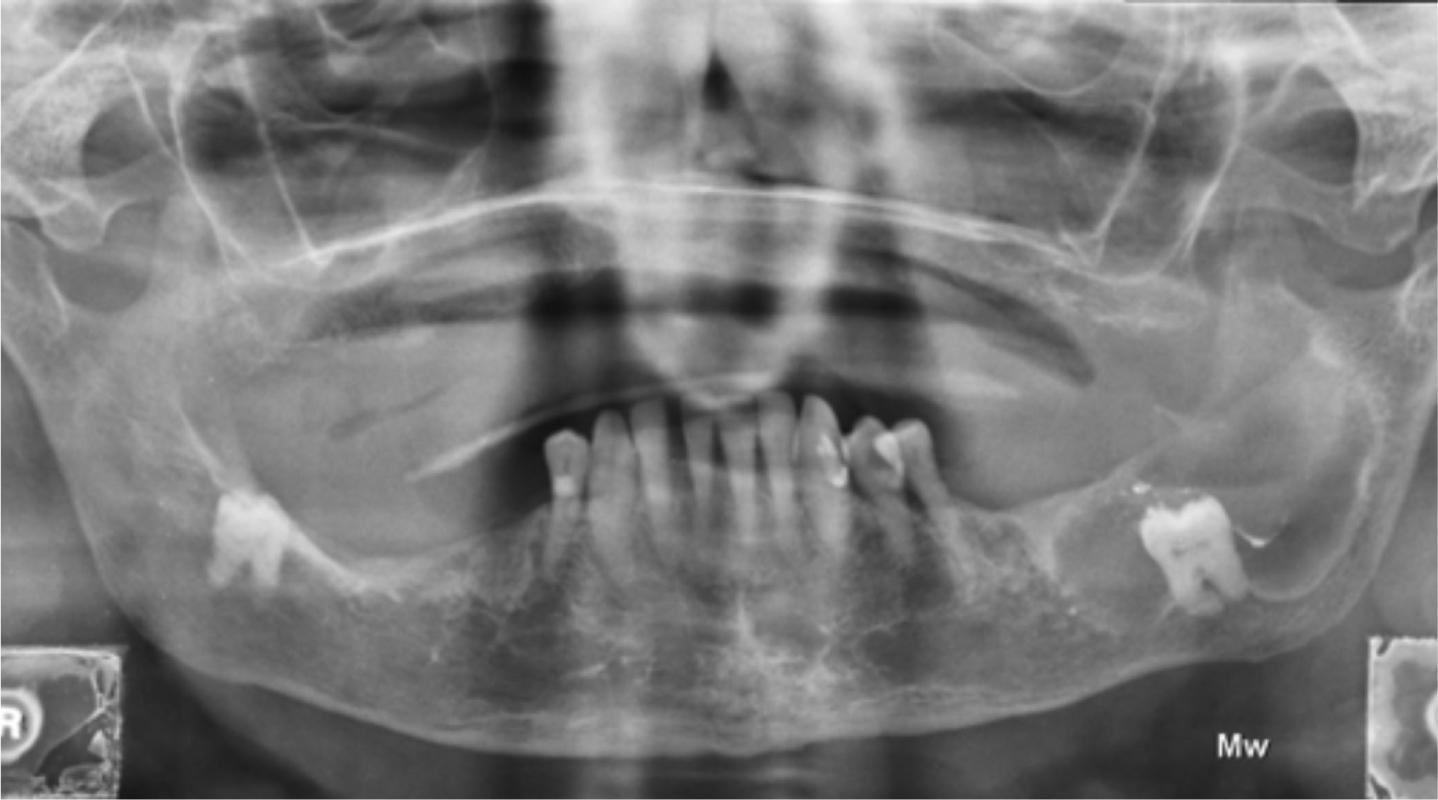
This patient had multiple comorbidities therefore opted for cyst marsupialization with BIPP packing as opposed to cyst enucleation with wisdom tooth extraction (Figure 6).
Figure 6. Orthopantomogram taken 4 weeks post-operatively showing early infill of dentigerous cyst defect associated with LL8 and remnant of BIPP following pack removal.
Conclusion
BIPP use started at the turn of the 20th century and it still continues to be widely used in dental/oral and maxillofacial/ENT surgery for surgical cavity packing and wound dressing. Some of the benefits include: application of pressure; haemostasis; and antisepsis. Although side effects and adverse reactions have been reported, these are uncommon events. There is no evidence that BIPP interacts with any other drugs; however, it should be used with caution in patients with hyperthyroidism and in pregnant/breastfeeding women. Further studies are required to establish the extent of the risks in these groups.
There are a number of alternatives to BIPP for surgical cavity packing and wound dressing, but despite this, BIPP still remains a preferred choice in many clinical scenarios. Overall, we therefore believe that BIPP is a relatively safe and inexpensive material that still has a place in current surgical management and should be recommended as a stock item in theatre, on the ward and in dental/oral and maxillofacial/ENT departments.