Herd MK, Woods M, Anand R Lymphoma presenting in the neck: current concepts in diagnosis. Br J Oral Maxillofac Surg. 2012; 50:309-313 https://doi.org/10.1016/j.bjoms.2011.03.263
Ammar MI, Oeppen RS, Bowles C, Brennan PA. Hard neck lumps: a review of uncommon and sometimes overlooked causes of these worrying presentations. Br J Oral Maxillofac Surg. 2017; 55:899-903 https://doi.org/10.1016/j.bjoms.2017.06.008
Aldridge T, Kusanale A, Colbert S, Brennan PA. Supraclavicular metastases from distant primaries: what is the role of the head and neck surgeon?. Br J Oral Maxillofac Surg. 2013; 51:288-293 https://doi.org/10.1016/j.bjoms.2012.03.016
Yalin Y, Pingzhang T, Smith GI, Ilankovan V. Management and outcome of cervical lymph node metastases of unknown primary sites: a retrospective study. Br J Oral Maxillofac Surg. 2002; 40:484-487 https://doi.org/10.1016/s0266435602002449
Oeppen RS, Gibson D, Brennan PA. An update on the use of ultrasound imaging in oral and maxillofacial surgery. Br J Oral Maxillofac Surg. 2010; 48:412-418 https://doi.org/10.1016/j.bjoms.2009.10.022
Shah KS, Ethunandan M. Tumour seeding after fine-needle aspiration and core biopsy of the head and neck – a systematic review. Br J Oral Maxillofac Surg. 2016; 54:260-265 https://doi.org/10.1016/j.bjoms.2016.01.004
Compérat E, Zhang F, Perrotin C Variable sensitivity and specificity of TTF-1 antibodies in lung metastatic adenocarcinoma of colorectal origin. Mod Pathol. 2005; 18:1371-1376 https://doi.org/10.1038/modpathol.3800422
Cervical lymphadenopathy can serve as a silent progressive indicator of systemic pathology and metastatic disease. Incidental or asymptomatic cervical lymphadenopathy can present a clinical dilemma when deciding on appropriate referral pathways and in specialist investigations. Metastasis to the head and neck may be more easily identified than locating the primary tumour site, which often requires a multitude of investigations to achieve an accurate diagnosis. As highlighted in this case report, primary care dentists play a central role in identification of patients with cervical lymphadenopathy who may require urgent specialist input in the context of subclavicular disease.
CPD/Clinical Relevance: This article highlights the clinical assessment of cervical lymphadenopathy and the investigatory tools used in secondary care to facilitate diagnosis.
Article
The COVID-19 pandemic continues to draw uncertainty with regard to identifying patients with undiagnosed cancer. The health crisis has been followed by significant reductions in urgent referrals from primary care, likely to be attributable to increased remote consulting, reduced face-to-face assessment and public fear resulting in patient reluctance to attend clinical settings. Approximately 12,000 new head and neck cancer diagnoses are made yearly in the UK, accounting for 3% of all new cancer cases.1 Data from England in April 2020 compared to April 2019, showed a 60% decrease in the number of urgent cancer referrals and an 18% decline in the number of people commencing treatment following an urgent GP referral.2,3 Emergency department presentations in England also decreased by 57% in April 2020 compared to the same period in the previous year.2 Thus, as the pandemic evolves, there is an emerging clinical iceberg of undiagnosed cancers yet to present.
Neck lumps can be the primary or associated alerting sign to suspicious systemic pathology. A case report of a patient who presented with cervical lymphadenopathy to her dentist during the first COVID-19 lockdown in England and was subsequently diagnosed with metastatic malignancy from an asymptomatic primary lung site is presented.
Case report
A 65-year-old Afro-Caribbean female patient was referred urgently to the Oral and Maxillofacial Surgery (OMFS) unit by her GDP during the the first national COVID-19 lockdown in England, for assessment of a right parotid gland swelling and enlarged right supraclavicular lymph node. The patient consulted her GDP with a 4-week history of right-sided facial pain, a loose tooth and a neck lump. Medically, she was fit and well with no regular medications and was an ex-smoker, having smoked for 30 years before stopping at the age of 50. Alcohol consumption was less than 14 units weekly. She had no significant family history apart from her step-brother who reportedly had cancer. She was retired, having worked previously as a receptionist and telephonist. The lower right second premolar was cavitated and mobile with tenderness to percussion, alongside a palpable, firm swelling within the right parotid gland and a solitary, firm, enlarged right supraclavicular lymph node. A 2-week wait referral was made to OMFS to investigate the right parotid swelling, which was provisionally diagnosed as cervical reactive lymphadenopathy.
Assessment by OMFS revealed a right pre-auricular swelling extending below the earlobe. An enlarged, firm, fixed lymph node was noted in the right level III region of the neck. A second firm lymph node was identified in the right level IV region. Examination of the intra-oral soft tissues was normal. There was no history of weight loss, cough, haemoptysis or shortness of breath. Cavities were confirmed to the LR5 and LR4, with peri-apical radiolucency associated with the LR5 demonstrated by an orthopantogram (OPG) (Figure 1). Treatment of these teeth was referred back to the GDP while the patient underwent further investigations.
Figure 1. OPG obtained on initial assessment by the OMFS unit demonstrating caries on the LR5 and LR4 with a peri-apical radiolucency associated with the clinically mobile LR5 tooth
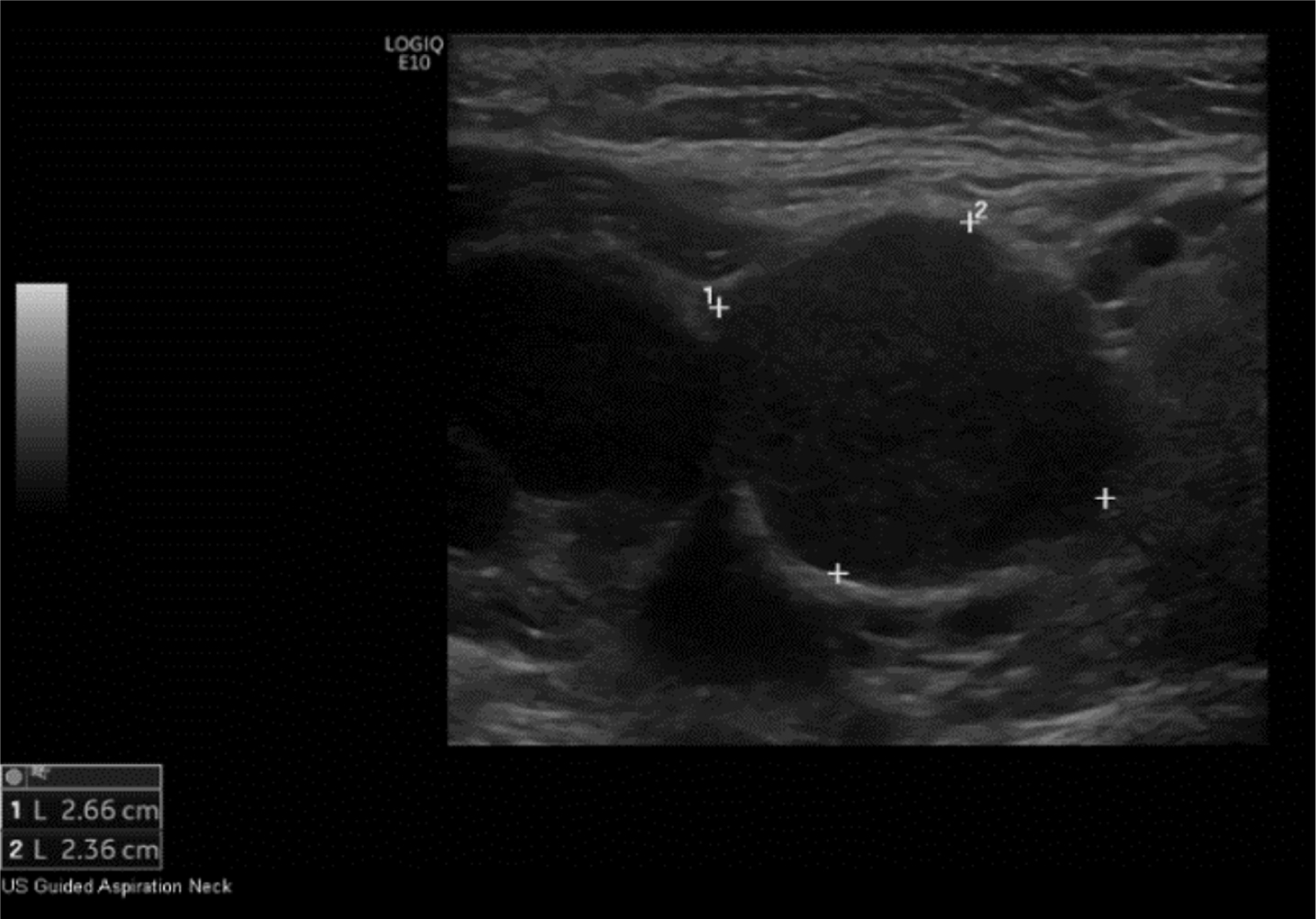
Ultrasound revealed multiple abnormal lymph nodes in the right neck levels II–V and left neck levels IV and V, with rounded, hypo-echoic appearances (Figure 2). Similar abnormal lymph nodes were identified in the right parotid gland. The thyroid and submandibular glands were unremarkable, as was the left parotid gland.
Figure 2. Ultrasound image of the left neck demonstrating abnormal lymph nodes
A right level V lymph node core biopsy was carried out under local anaesthetic. Microscopic histological examination revealed a metastatic, poorly differentiated malignant tumour of epithelial origin. Immunohistochemistry stains were performed and the tumour cells were noted positive for thyroid-transcription factor-1 (TTF-1). The immunohistochemistry profile was consistent with metastatic, poorly differentiated carcinoma from a lung primary site.
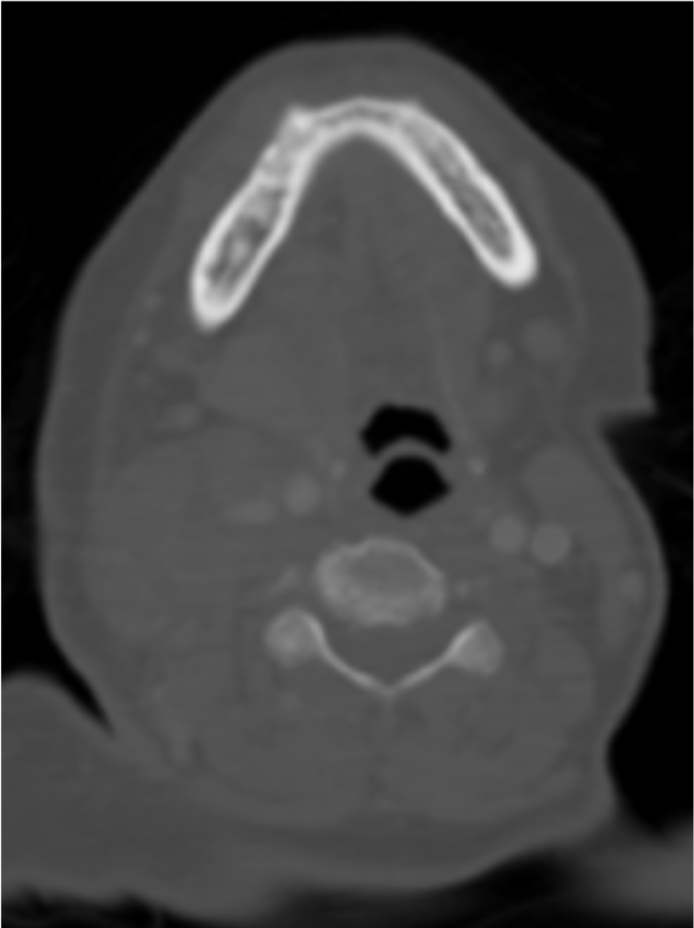
Neck computed tomography (CT) confirmed bilateral pathological lymph nodes, the largest measuring 3 x 2.5 cm in the right level II, III, IV and V regions. The airway was patent, although deviated to the left with parotid lymphadenopathy (Figure 3).
Figure 3. CT demonstrating deviation of the airway to the left with bilateral abnormal lymph nodes in the neck and right parotid lymphadenopathy
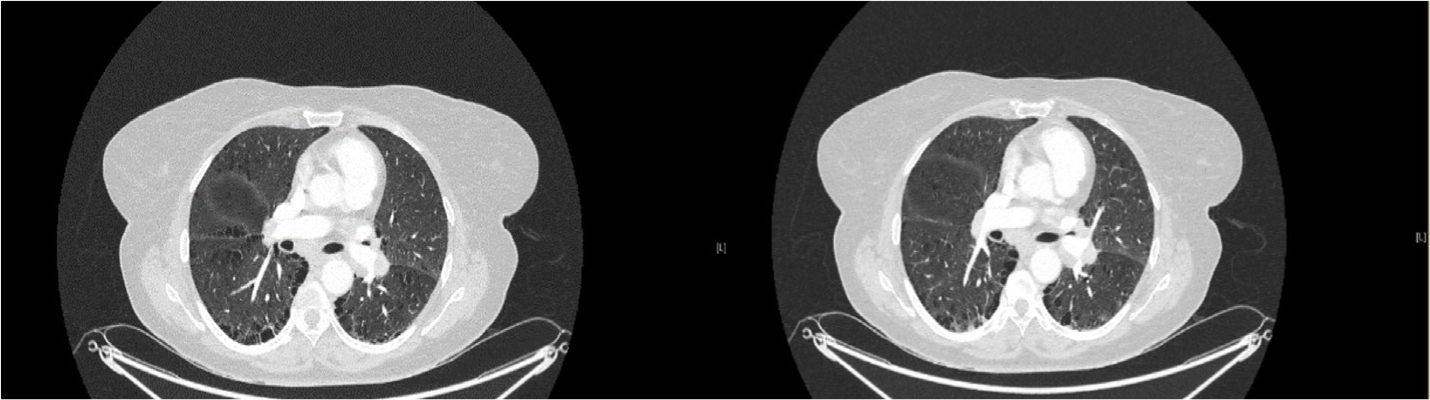
Chest CT revealed a 14.4 x 12 mm mass with spiculated contours in the right upper lung apex. Multiple mediastinal and hilar pathological metastatic lymph nodes were identified (Figure 4). A metastatic, peripheric, pleural-based nodule was present in the left upper lobe, inferior lingular segment. Abdominal CT excluded pathological lymph nodes or aggressive bone lesions.
Figure 4. Chest CT demonstrating multiple metastatic hilar lymph nodes, with a mass in the right lung
Given the findings, the right neck level V lymph node biopsy was indicative of metastatic non-small-cell carcinoma from a lung primary site, with further lung lymph node sampling using endobronchial ultrasound, confirming adenocarcinoma. Thus, the final diagnosis was adenocarcinoma of the right lung with cervical, parotid, mediastinal and hilar lymphadenopathy. The staging was T3N3M0.
Oncologist specialist opinion deemed immunotherapy with anti-neoplastic agent pembrolizumab an appropriate management strategy. Given that the tumour was positive for programmed death ligand-1 (PDL-1), the aim of this treatment was to inhibit activity of this protein and allow the patient's own immune system an opportunity to recognize and destroy the cancer cells. This would provide a more specific and targeted treated compared to radiation or chemotherapy, while also avoiding common chemotherapy-associated side-effects, including nausea, vomiting and hair loss. Surgical intervention was not deemed suitable at this stage, given the size and location of the primary tumour and dissemination to distant lymph nodes. Treatment was led by the oncology team with a plan for ongoing OMFS review.
Discussion
There are approximately 300 lymph nodes in the head and neck region, a significant proportion of the estimated 800 lymph nodes in the entire lymphoreticular system.4 History-taking, particularly a patient's reason for seeking a professional opinion, is critical in the information-gathering process. A neck lump causing symptoms, such as pain, or an asymptomatic neck lump causing concern, may be the primary reason for a patient seeking consultation. A neck lump identified as an incidental finding during a clinical encounter requires equal investigation to confirm its nature and exclude suspicious or systemic pathology. For example, a hard, left-sided neck lump might be the sole presentation of an asymptomatic malignancy of the aerodigestive tract.5
In the context of metastasis, cervical lymphadenopathy is a common presentation of head and neck malignancy before the primary tumour becomes symptomatic. Metastatic pathways are dictated by anatomical relationships, so may be predictable.6 Although cervical lymph nodes drain the head and neck, they can become involved with distant primary tumours. The downward flow of the head and neck lymphatic system can aid identification of a primary malignancy.6 However, in systemic disease processes, inferior lymphatic communications allow entry into the neck.6 Solitary supraclavicular lymphadenopathy raises concerns of distant primary malignancy below the clavicle. Cutaneous, salivary, oral, pharyngeal and laryngeal lesions require exclusion and investigation.6 Enquiries should also be made into risk factors and concurrent symptoms beyond the oral cavity, for example a cough, haemoptysis, haematuria, prostatic symptoms, changes in bowel habits or gynaecological bleeding.6 In addition to cervical lymphadenopathy, lymphadenopathy at other node sites, namely the axilla, groin and abdomen, are relevant in the consideration of lymphoma, which accounts for approximately 5% of head and neck malignancy.4 Lymph node firmness on palpation may indicate calcification, which can result from malignancy, cancer therapy, such as radiotherapy, caseous necrosis in tuberculous lymphadenitis, sarcoidosis or amyloidosis.7
The likely primary site for a poorly differentiated carcinoma metastasized to the cervical lymph node is a site in the head and neck region. The primary site for most cervical nodal metastatic squamous cell carcinomas is the oral cavity, larynx or cervical oesophagus.8
Approximately 11% of cervical lymph nodes containing metastases originate from lesions outside the head and neck.8 Thus overall, lung cancer spread to the neck is a rare cause of cervical lymphadenopathy. Supraclavicular lymph nodes are most commonly involved and thus, isolated lymphadenopathy in this region raises suspicion of subclavicular disease.6 Most lung tumours are classified as non-small-cell carcinomas or small-cell carcinomas. Non-small-cell carcinoma are differentiated into subtypes of varied prevalence: squamous carcinoma (40%); large-cell carcinoma (25%); adenocarcinoma (10%); and alveolar cell carcinoma (10%).6 Dissemination risk is up to 82% in adenocarcinoma, which alongside large-cell carcinomas, have an increased tendency to metastasize beyond the thorax.6
Examinations including panendoscopy, fine-needle aspiration cytology (FNAC) and imaging are required to locate the primary cancer. If the primary remains occult and node biopsies inconclusive, investigations should extend beyond the head and neck.6 Ultrasound is a well-tolerated, widely accessible study that can rapidly provide diagnostic information to support clinical examination of superficial structures, as part of active investigations or monitoring of cervical lymphadenopathy.9 Abnormal lymph nodes are usually hypo-echoic with cortical thickening and loss of the central echogenic hilus.9 Primary lesions not located by examination, CT, MRI or positron emission tomography require lymph node tissue sampling.6
FNAC and core-needle biopsies are readily performed by manual palpation or image guidance, avoiding the invasiveness and adverse outcomes associated with open biopsy.10 Accuracy rates are reportedly up to 98% for FNAC and 100% for core needle biopsy.10 FNAC has high diagnostic accuracy, sensitivity and specificity in the diagnosis of malignant lymph nodes, including metastatic squamous cell carcinoma in the head and neck. Despite this, FNAC is based solely upon cytology rather than lymph-node architecture. Thus, histological subtyping is not possible and tissue sampling, frequently via core biopsy, facilitates a conclusive diagnosis.4
Immunohistochemistry further supports identification of primary lesions. TTF-1, a tissue-specific transcription factor expressed in thyroid and lung epithelial cells, is frequently expressed by thyroid and lung carcinomas, aiding distinction between primary lung carcinoma and lung metastasis.11
Conclusion
Cervical lymphadenopathy, particularly supraclavicular nodes, may be the only alerting sign to advanced systemic disease. GDPs should be vigilant to the possibility of asymptomatic subclavicular malignancy by ensuring thorough history-taking and clinical recognition of abnormalities. Diagnostic challenges can present in metastatic neck lumps, particularly if there is difficulty in locating the primary tumour. Given the challenges to patient access and provision of clinical care presented by the pandemic, GDPs play an increasingly pivotal role in identifying potential sinister pathology and initiating the patient journey to receiving a definitive diagnosis.