
Article
Dentists' risk in COVID-19 times
Coronavirus Disease 2019 (COVID-19) originates from a virus currently identified as SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2).1 The coronavirus is most abundant in the nasopharyngeal region and the salivary secretions in infected individuals.2,3 The virus may be transmitted via droplets or direct contact, including or even from asymptomatic patients.4
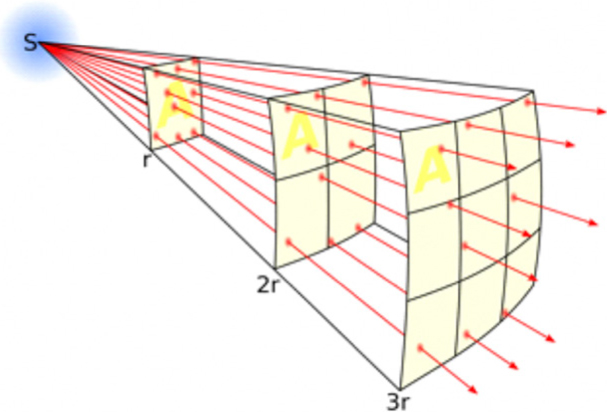
Dental professionals are particularly susceptible due to the nature of the occupation, working within intimate distances of patients.4,5 The Inverse-Square Law dictates that a dentist at 50 cm from a patient's mouth would be exposed to nine times more aerosol droplets (Figure 1) compared to a social distance of 150 cm6 (the calculation is based upon the intensity ratio calculated by the inverse-square law: (1/0.502) ÷ (1/1.502). This has not yet accounted for any increase in aerosol emission as a result of dental treatment.
0.2% pre-treatment chlorhexidine mouthwash has been used to reduce the dental team's risk of contracting infectious diseases.7 Chlorhexidine has been shown to reduce intra-oral bacterial load, reducing the bacterial load of aerosol produced.7,8 However, its efficacy in preventing the spread of the SARS-CoV-2 virus may be questioned considering that it is an antibacterial with weak virucidal properties.4,9,10
Povidone-iodine can reduce the viral load in the oral cavity and oropharynx significantly, it was found to be potent against Middle-East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS) coronaviruses.11,12 1% Povidone-iodine mouthwash was shown to reduce the viral titre of MERS and SARS coronavirus by 99.99%.11 However, its use should be excluded in those with iodine hypersensitivity, thyroid disease, impaired renal function, pregnant and breastfeeding women.13,14
The coronavirus envelope contains a lipid bilayer, which makes the virus highly susceptible to oxidizing agent disinfectants.15 0.5% Hydrogen peroxide at 0.5-1% and 0.21% sodium hypochlorite have been shown to be effective against coronaviruses.4,9 0.25% sodium hypochlorite mouthwash has been used in periodontal treatment.12,16,17 The use of these agents under dentist supervision, as pre-treatment mouthwash as an alternative to chlorhexidine, may be prudent in the current circumstances surrounding COVID-19.