Glendor U. Epidemiology of traumatic dental injuries – a 12 year review of the literature.: official publication of International Association for Dental Traumatology; 2008
DiAngelis AJ, Andreasen JO, Ebeleseder KA International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012; 28:2-12
Andersson L, Andreasen JO, Day P International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2012; 28:88-96
Cardaropoli G, Araujo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J Clin Periodontol. 2003; 30:809-818
Tan WL, Wong TL, Wong MC, Lang NP. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012; 23:1-21
Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodont Rest. 2003; 23:313-323
Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005; 32:212-218
Araújo MG, Sukekava F, Wennstrom JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol. 2005; 32:645-652
Botticelli D, Berglundh T, Lindhe J. Hard-tissue alterations following immediate implant placement in extraction sites. J Clin Periodontol. 2004; 31:820-828
Chen ST, Darby IB, Reynolds EC. A prospective clinical study of non-submerged immediate implants: clinical outcomes and esthetic results. Clin Oral Implants Res. 2007; 18:552-562
Sanz M, Cecchinato D, Ferrus J A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. Clin Oral Implants Res. 2010; 21:13-21
Hammerle CH, Chen ST, Wilson TG Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004; 19:26-28
Braut V, Bornstein MM, Belser U, Buser D. Thickness of the anterior maxillary facial bone wall – a retrospective radiographic study using cone beam computed tomography. Int J Periodont Rest. 2011; 31:125-131
Horvath A, Mardas N, Mezzomo LA, Needleman IG, Donos N. Alveolar ridge preservation. A systematic review. Clin Oral Investig. 2013; 17:341-363
Morjaria KR, Wilson R, Palmer RM. Bone healing after tooth extraction with or without an intervention: a systematic review of randomized controlled trials. Clin Implant Dent Relat Res. 2014; 16:(1)1-20 https://doi.org/10.1111/j.1708-8208.2012.00450.x
Maestre-Ferrin L, Boronat-Lopez A, Penarrocha-Diago M, Penarrocha-Diago M. Augmentation procedures for deficient edentulous ridges, using onlay autologous grafts: an update. Med Oral Patol Oral. 2009; 14:e402-407
von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients. Clin Oral Implants Res. 2006; 17:359-366
Ilizarov GA, Ledyaev VI. The replacement of long tubular bone defects by lengthening distraction osteotomy of one of the fragments. 1969. Clin Orthop Relat Res. 1992; (280)7-10
McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg. 1992; 89:1-8
Patients who suffer dento-alveolar trauma present a unique challenge for the dentist. There are numerous options to consider when attempting to restore the dentition. This article reviews the role of dental implants in replacing lost or damaged teeth. It also describes some of the options available to maintain the alveolar bone between tooth removal and implant placement, as well as techniques used to recreate the deficient hard and soft tissue after a tooth has been avulsed or extracted.
Clinical Relevance: Knowledge of the role of dental implants and techniques for the preservation of the hard and soft tissues will assist the clinician to reduce patient morbidity and achieve an optimal restorative result.
Article
Traumatic dental injuries occur frequently in both children and adults. A 12-year review of the literature1 indicates that 25% of school children have experienced at least one episode of dental trauma. This figure rises to 33% for permanent teeth in adults, with most injuries occurring before the age of nineteen.
Management of trauma
In most cases, maintaining the natural dentition is the ideal option and so every attempt should be made to preserve the tooth or teeth after an accident. Following the most up-to-date dental trauma protocols,2,3 including re-implantation, splinting and use of antibiotics, will provide the best opportunity for achieving this.
The authors would also recommend an excellent online resource The Dental Trauma Guide (www.dentaltraumaguide.org) which is an interactive tool and suggests an evidence-based treatment for every traumatic dental injury (Figure 1).
Figure 1. The Dental Trauma Guide website (www.dentaltraumaguide.org).
Reasons for tooth loss
Even if the above-mentioned protocols are adhered to, however, the involved tooth or teeth may still require eventual replacement. Tooth loss may occur immediately or at a later date due to one of the various complications after trauma, including:
Root fracture;
Root resorption;
Ankylosis and subsequent replacement resorption; and
Long-term endodontic failure.
The tooth may even have been completely avulsed and lost at the outcome. The dentist is subsequently faced with the task of planning the next most appropriate course of action. In doing so, all treatment options should be considered, such as resin-bonded or conventional bridges, removable partial dentures, dental implants and orthodontic treatment involving space closure.
This two-part article will focus solely on the role of dental implants in the management of dento-alveolar trauma, including the theory and techniques used to preserve the hard and soft tissues where implant placement needs to be delayed owing to the young age of the patient.
Fate of the alveolar process after tooth loss
The alveolar process is dependent on the continued presence of the teeth. If a tooth is extracted or lost, a number of alterations will occur. Cardaropoli et al4 described the events that take place within the socket after a tooth is removed. Blood clot formation occurs in the first 24 hours. This is replaced by granulation tissue in the following 2–3 days while the epithelium starts to cover the entrance of the socket. After approximately 7 days, the granulation tissue is replaced with connective tissue and osteoid, which is a precursor to bone. Within 3 weeks, there are signs of osteoid mineralization as immature woven bone is laid down. The entire socket entrance should be epithelialized at this point. After 6 weeks, bone formation within the socket is more pronounced and further mature bone with trabeculae can be seen.
During this period, whilst the extraction socket is filling with new bone, the remaining alveolus undergoes remodelling. Reduction in ridge width (Figure 2) of 29–63% and height loss of 11–22% has been reported in a recent systematic review.5 Fifty percent of ridge reduction will occur within the first year after extraction, of which 30% occurs within the first 3 months.6
Figure 2. Reduced ridge width of lateral incisor space after tooth loss.
Bundle bone theory
Although the above describes what happens within the extraction socket, it does not illustrate all the processes that occur.
Bundle bone is a thin cortical plate lining the alveolar socket, which on a radiograph is referred to as lamina dura. It is approximately 0.8 mm thick and does not receive the same type of blood supply as trabecular (spongy) bone. Within the jaws, the bundle bone is very much dependent on the periodontium for its blood supply in assisting bone maintenance and turnover. When a tooth is lost, the periodontium is severed and eventually eliminated with collateral loss of the dependent bundle bone. This seems to have a significant impact on the bone availability when placing implants, particularly in the anterior maxilla. Araújo and Lindhe7 studied the alterations in the edentulous ridge profile that occurs following tooth extraction in dogs. They found that, although the lingual wall remained relatively unchanged, the buccal wall margin moved more apically by 1.8 mm ± 0.2 mm after 8 weeks.
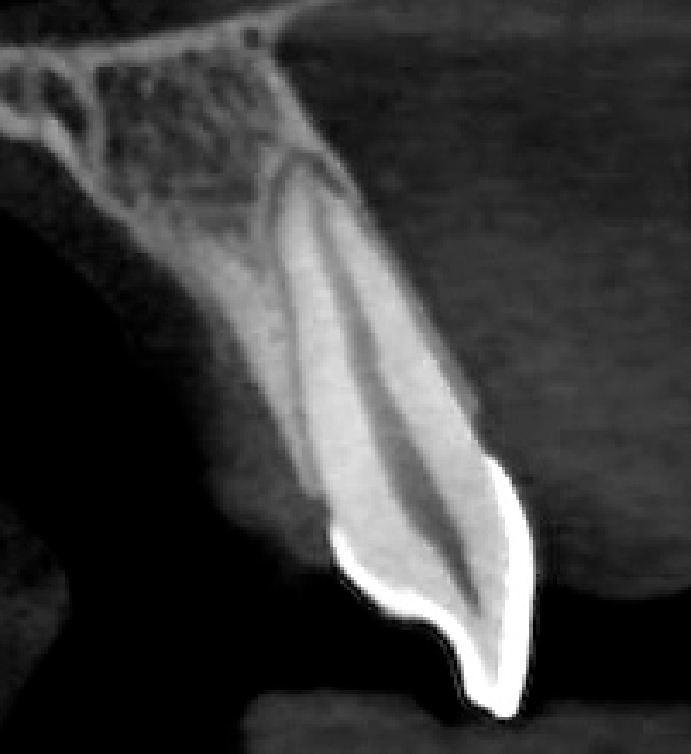
This may be due to the fact that the lingual wall is considerably thicker than the buccal wall. Indeed, the buccal/labial wall in the anterior maxilla may be composed entirely of bundle bone (Figure 3), which would have significant consequences when planning to replace the tooth with a dental implant.
Figure 3. Cross-section of a central incisor showing thin labial bone plate which is most likely composed of bundle bone only.
Previously, it was believed that the placement of an implant immediately after extraction maintained the bone and soft tissue volume. Araújo and colleagues compared extraction sites against extraction with immediate implant sites.8 The resulting buccal and lingual walls were found to be similar at the edentulous and implant sites, with more pronounced bone loss at the buccal aspect. Human studies9,10,11 have demonstrated significant buccal ridge resorption when implants are placed immediately after extraction, with figures ranging from 30–56%. Immediate implant placement is a more technique-sensitive procedure,12 with potentially compromised long-term aesthetic outcomes.
A recent study,13 measuring labial bone thickness in 125 subjects, reported that, in 90% of cases, the labial bone was either thin or missing, while only 10% of anterior teeth had labial bone thickness greater than 1 mm. This finding is significant, as Ferrus et al14 demonstrated that sockets with labial wall thickness < 1 mm resulted in 43% width reduction in comparison to only 21% reduction if the labial wall thickness was > 1 mm.
As mentioned, the post extraction remodelling processes that occur will result in an overall reduction in alveolar ridge width and height. There will also be a lingual or palatal shift in the centre of the ridge (Figure 4), or it may result in complete loss of the alveolar process following tooth loss. This is true for both single and multiple tooth loss and is particularly severe if part or all of the labial alveolar bone is missing at the time of tooth loss.
Figure 4. Palatal shift of the centre of the ridge.
Alveolar ridge preservation
If, after trauma, the patient is too young or there are other factors (eg pathology, financial constraints) that preclude early implant placement, there are a number of strategies that a clinician should consider to minimize alveolar ridge resorption and thus facilitate dental implant placement at a later stage. Without such intervention, resorption of the alveolar ridge is inevitable and it may be severe enough to preclude implant placement, unless invasive block bone grafting is carried out to reconstruct the ridge morphology.
Therefore, as far as the site-specific management strategies are concerned, one should consider the following options:
Decoronate and bury the root;
Extraction and alveolar ridge preservation.
Decoronate and bury the root
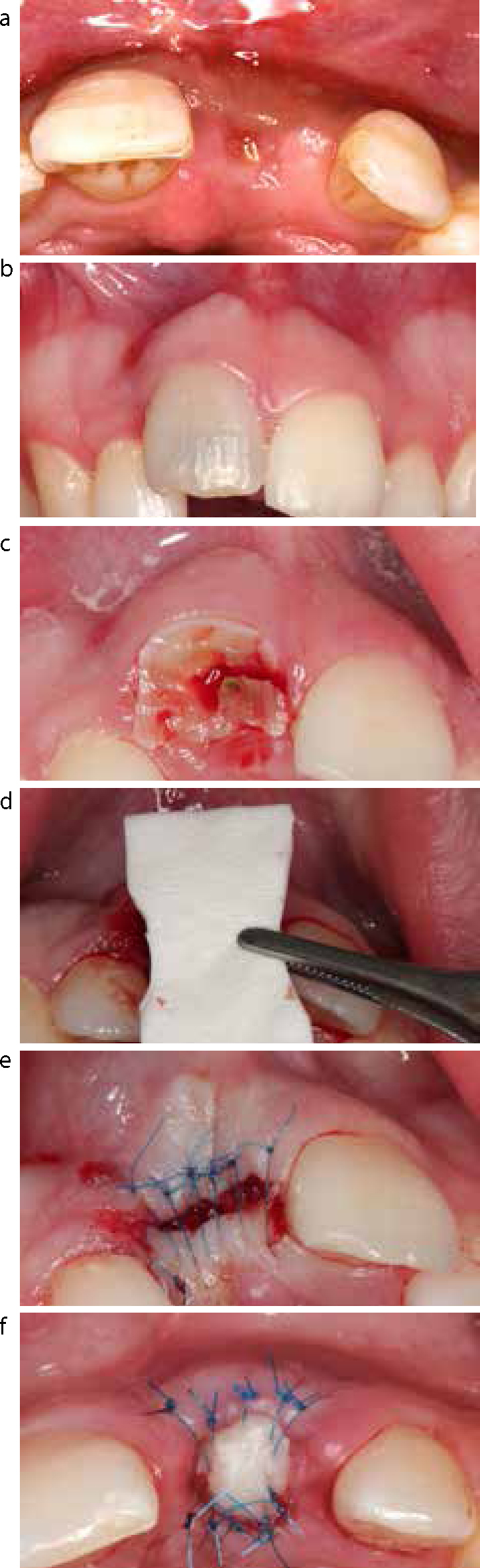
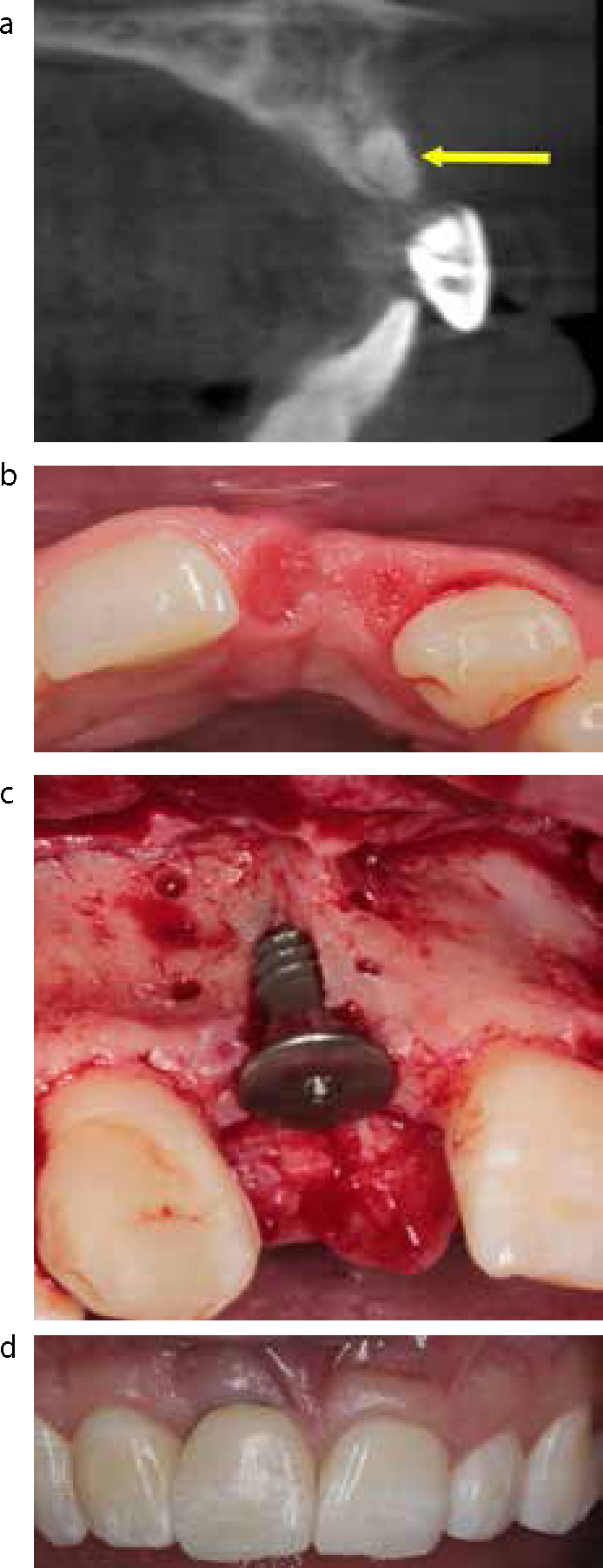
The preserved root will maintain the periodontium and thus sustain an intact blood supply for the bundle bone. This will prevent the alveolar ridge remodelling as described above and maintain the alveolar ridge width and height. This option may not be appropriate if certain types of tooth-associated pathology are present. Root canal disinfection and obturation may be considered prior to burying teeth with pulpal pathology, whereas roots with vital pulp do not necessarily require endodontic treatment. The socket opening should be surgically covered with a free gingival graft or a recently introduced soft tissue matrix graft (eg Geistlich Mucograft) as the epithelium is unlikely to cover the retained root completely (Figure 5 a–f).
Figure 5.
(a) Buried root with incomplete spontaneous soft tissue closure. (b) Traumatized UR1 (c) UR1 is decoronated. (d) Soft tissue matrix (Geistlich Mucograft) placement. (e) Final closure. No attempt is made to achieve primary closure. (f) Alternative closure with free gingival graft harvested from palate.
When the patient is old enough or contra-indications to implant placement have been addressed, the root can be extracted and a dental implant placed in the preserved site. This option also has the added benefit of allowing appropriate time for adequate treatment planning.
Extraction and alveolar ridge preservation
If the tooth has been avulsed and lost or it is felt that the remaining root is not viable for burying (Figure 6), the clinician may perform one of a range of ridge preservation techniques.
Figure 6. Unviable root for burying.
Essentially, this involves packing the extraction socket with a bone graft material. These bone graft substitutes can be animal derived (xenografts); human-derived (allografts); or synthetic (alloplastic) graft materials and are designed to encourage host bone formation through Guided Bone Regeneration (GBR).
Guided Bone Regeneration has its basis in the principles of Guided Tissue Regeneration (GTR). GTR was initially developed to treat lost periodontal tissues as a result of periodontitis. It was believed that by preventing the gingival epithelial and connective tissues from entering a treated defect through the use of cell occlusive membranes, the non-excluded cells with potential for periodontal regeneration would be allowed to proliferate in the defect and regenerate the lost tissues.
GBR follows a similar process, with the use of membranes which prevent the rapid migration of soft tissues that can hinder and prevent osteogenesis, but differs in that there is no associated tooth at the treated site.
Graft materials are used in conjunction with membranes and range in their reported abilities to maintain and encourage bone formation. The ideal grafting material should include some, if not all, of the following properties:
Osteogenesis – new bone is formed by cells contained within the graft material;
Osteoconductivity – the graft may not contribute to new bone formation but acts as a scaffold for bone formation by host tissue;
Osteoinductivity – the graft helps to induce the host tissues in the surrounding area to form new bone.
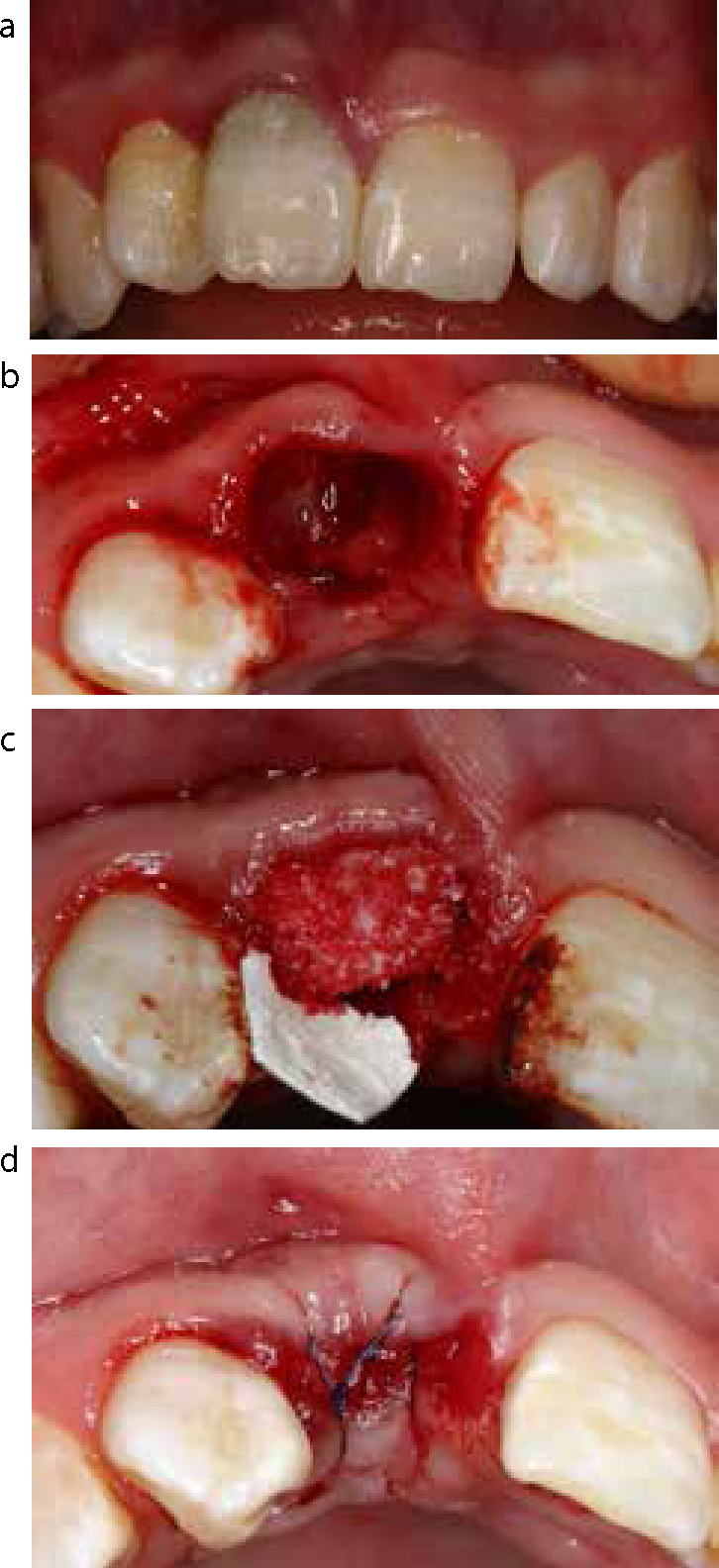
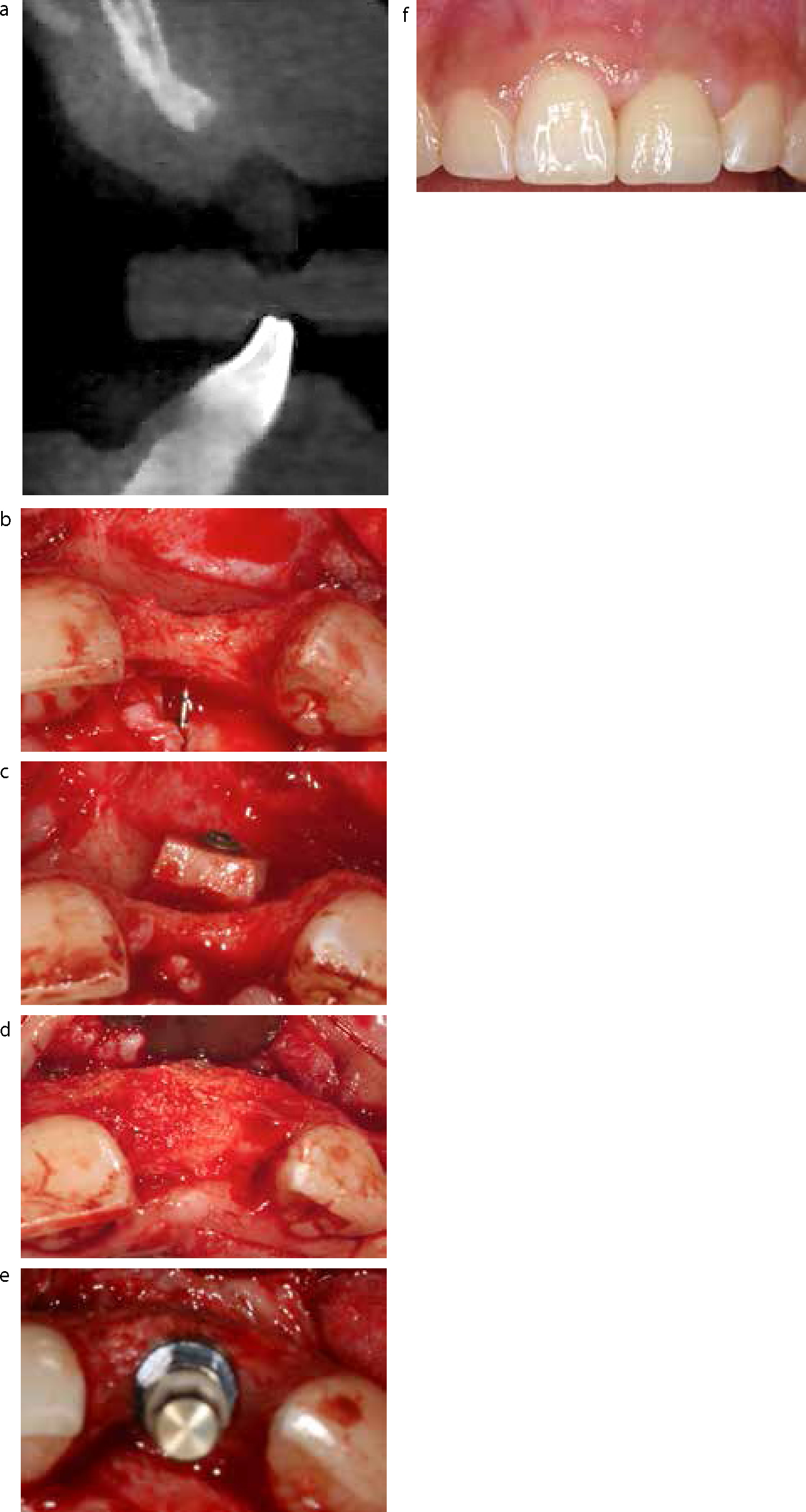
Apart from autografts (patient's own bone), most of the bone substitutes are primarily osteoconductive. The bone substitutes are generally used in combination with barrier membranes to exclude soft tissue infiltration from the periosteum into the bone graft, with resultant resorption and fibrous encapsulation. The most commonly used membranes are collagen-derived from animals, eg Bio-Gide (Figure 7 a-d), synthetic membranes, eg Cytoplast or MembraGel (Figure 8 a–e) or allograft, eg Alloderm, that cover the graft material and stabilize the site while minimizing the resorption of the bone substitute.
Figure 7.
(a) Pre-op of UR1 due for extraction. (b) Extraction socket with buccal bone of the socket found to be completely missing. (c) Extraction socket grafted with deproteinized bovine bone mineral which is covered by porcine collagen membrane. (d) Final closure, with only partial coverage of the membrane.Figure 8.
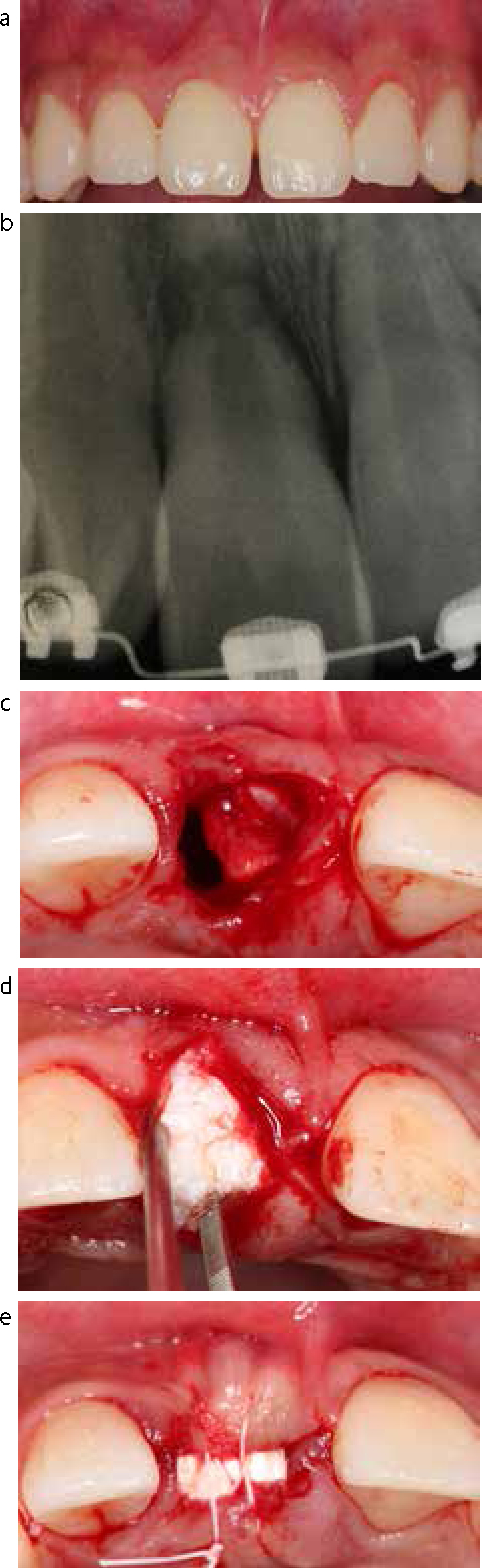
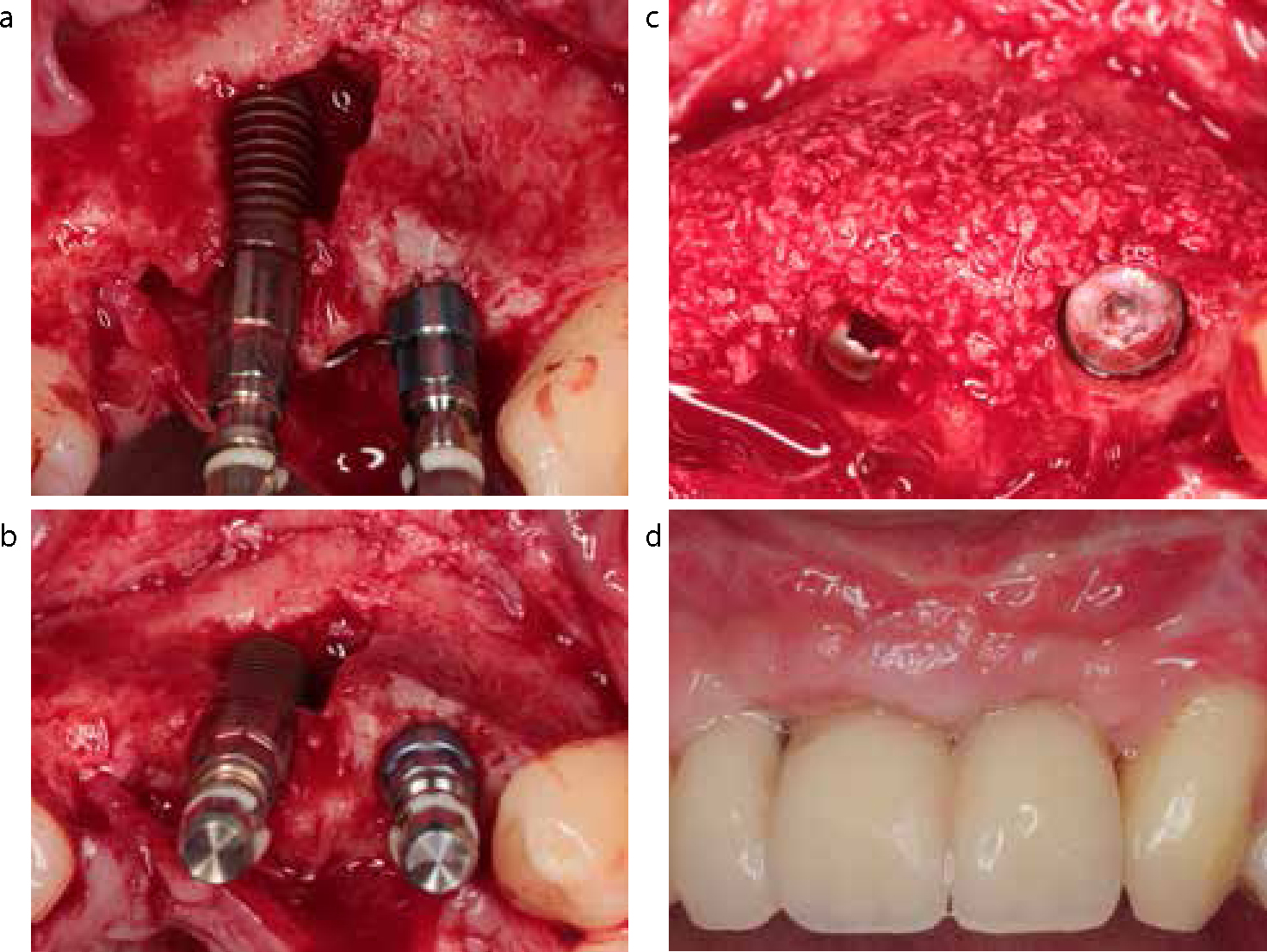
(a) Pre-op of UR1 to be extracted. (b) UR1 with external root resorption. (c) Extraction socket with resorption of buccal plate. (d) Socket grafted with deproteinized bovine bone mineral and covered by dense-PTFE membrane. (e) Dense-PTFE membrane can be left exposed and primary closure is not necessary.
Although these methods are used to encourage favourable bone growth and minimize alveolar ridge resorption15 (Figures 9 and 10), that occurs following tooth removal, there is inconclusive evidence supporting the efficacy of such techniques, and the quality of regenerated bone is particularly debated.16
Figure 9.
(a) Cone-beam CT scan after 37 months showing radio-opaque outline of the grafted bone material (arrowed), which has resulted in maintenance of ridge width of patient in Figure 7. (b) Ridge width at implant surgery. (c) Even though a dehiscence is encountered, implant placement was possible with simultaneous GBR, thereby preventing invasive block bone graft. (d) Final aesthetic result.Figure 10.
(a) Cone-beam CT scan after 14 months showing maintenance of ridge width of patient in Figure 8 (arrowed). The outline of the radio-opaque bone graft can be seen. As buccal bone at the time of extraction was missing, complete collapse of the ridge could be expected. (b) Ridge width at implant surgery. (c) Ridge on raising flap showing complete integration of the graft material. (d) Fenestration encountered during implant placement was managed with simultaneous GBR, thereby preventing invasive block bone graft. (e) Final aesthetic result.
Severe trauma
Cases of severe trauma may result in extensive loss of hard and soft tissues in both the vertical and horizontal planes, thereby necessitating more invasive augmentation procedures to reconstruct the lost alveolar ridge architecture to facilitate implant placement. Such patients should be informed of the difficulties involved under such circumstances prior to any treatment so that unrealistic expectations are avoided.
The most commonly used technique involves block bone grafts. Other techniques involving distraction osteogenesis, titanium-mesh grafting, etc can also be used in certain selected cases.
Autogenous block bone grafts
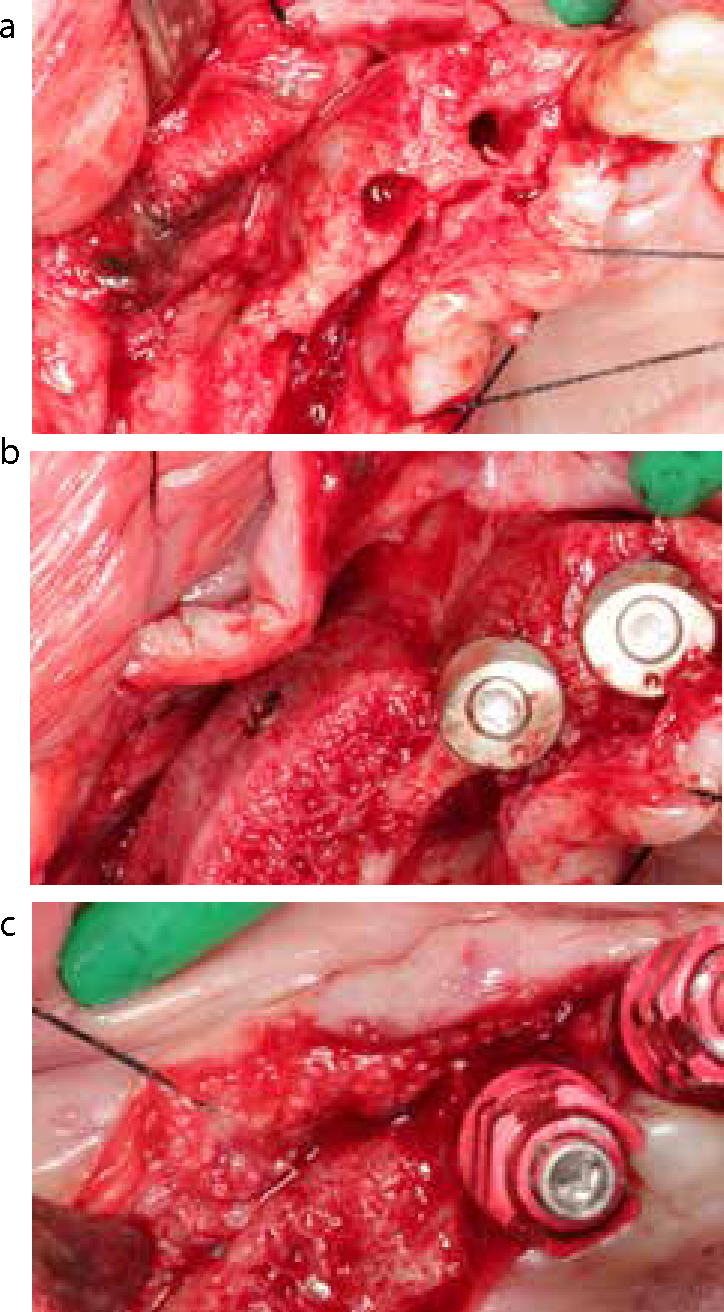
Autogenous block grafts are generally used in these situations and can be harvested from intra- or extra-oral locations, depending on the size of the defect being treated.
Intra-oral locations are used for smaller ridge deficiencies (Figure 11a) and are generally harvested from the retromolar area or the anterior mandible. Extra-oral locations are used for more extensive grafting and are harvested from the iliac crest of the hip bones. The grafts are removed as blocks which are held in position with fixation screws (Figure 11b). The block graft can be supplemented with other graft material or cancellous bone particles to fill voids (Figure 11c).
Figure 11.
(a) Cone Beam CT scan demonstrating significant alveolar ridge atrophy. (b) Severe hard tissue deficiency evident on reflection of flap. (c) Block bone graft held in position with fixture screw. (d) Graft, supplemented with deproteinized bovine bone mineral, after 6 months' healing. (e) Implant placed in grafted site. (f) Final restorative outcome.
The use of bone substitutes with membranes has been advocated to minimize the resorption of the block graft that may occur in unprotected grafts.17,18 Careful case selection should be a priority given the substantially increased morbidity involved with block graft use. Implants are then generally placed between 4–6 months after bone placement to allow ample time for graft integration before excessive resorption has occurred (Figure 11d–f).
Cadaveric block bone grafts
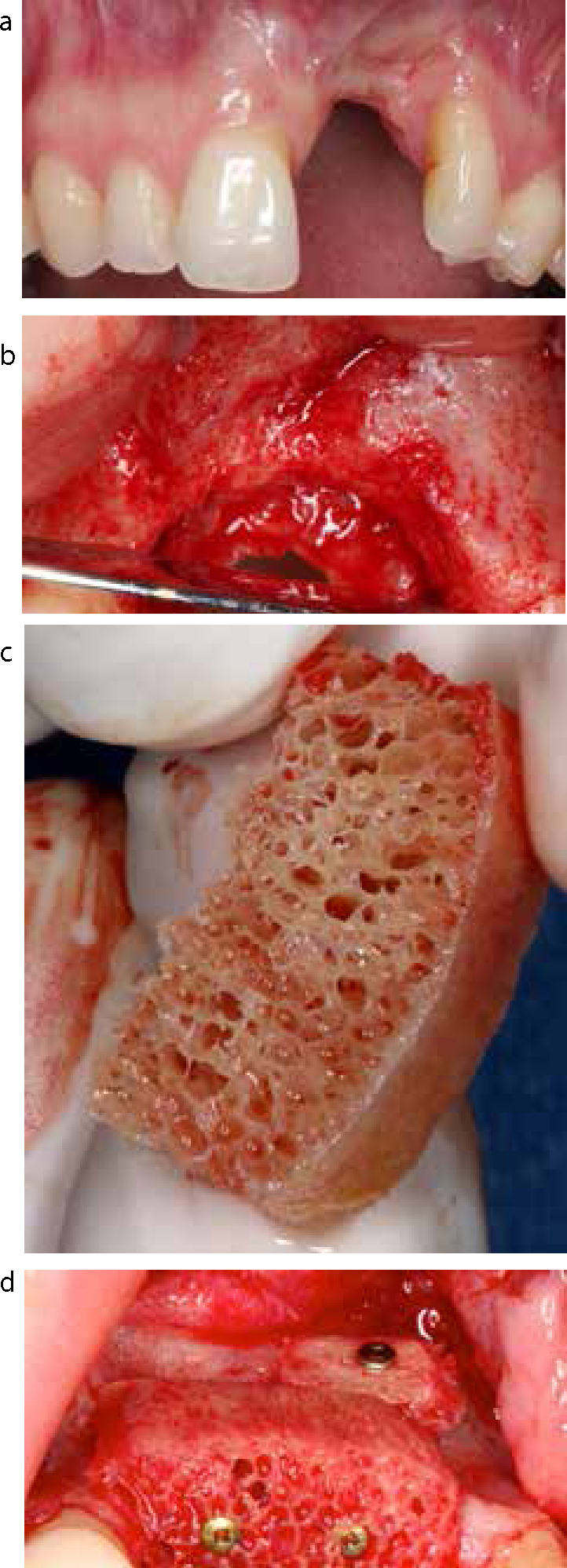
The use of processed cadaveric cortico-cancellous bone blocks can also be successfully used (Figures 12a–c, 13a–d) and has the advantage of precluding donor site morbidity, but there will always be concerns about the source of the tissue, especially given relatively recent funeral home scandals in the United States. Tissue banks should have appropriate accreditation and registration before clinicians consider using their products. There is also the perceived risk of contracting a disease with the use of such graft material, though to date there has not been a reported case of disease transmission in the literature. Nonetheless, the clinician should ensure that the patient is counselled and an informed, written consent is obtained. In the United Kingdom, the UK Blood Transfusion and Tissue Transplantation Services constantly review and update their guidance on human derived products (http://www.transfusionguidelines.org.uk) and should be contacted prior to use of such bio-materials.
Figure 12.
(a) Extensive alveolar ridge width deficiency requiring a large bone block graft. (b) A cortico-cancellous allograft was used which required adaptation to follow the shape of the maxillary ridge. (c) A well-integrated bone block at 4 months, ready for implant placement.Figure 13.
(a) Severe ridge deficiency after traumatic loss of teeth. (b) Horizontal and vertical bone loss seen after flap elevation. (c) Cortico-cancellous allograft block. (d) 3-dimensional augmentation with cortico-cancellous allograft block in place. Such volume of bone could have otherwise only been available from an extra-oral site.
In particular, large size grafts or multiple implant sites can be easily managed with allografts rather than having to rely on harvesting from the iliac crest of the patient. Iliac crest surgery increases patient morbidity, such as gait problems, nerve damage and increased recovery time, risks from general anaesthesia and costs to the NHS or the patient.
Distraction osteogenesis
Distraction osteogenesis has also been successfully used in the recreation of alveolar ridge deficiencies following severe trauma. Originally a chance finding by Ilizarov and Ledyaev19 in long bones, the technique has been used in the oral environment.20 Distraction osteogenesis involves the creation of a break within the treated bone followed by the use of distractors that maintain a gap between the two component parts and elongate the fractured callus. The stress and tension causes an increase in metabolic activity and increased cellular proliferation similar to endochondral ossification.
Distraction osteogenesis decreases the need for large bone grafts, the associated morbidity and the potential for infection that may occur. The patient must comply with the distraction schedule, while older patients may have a decrease in the number of mesenchymal stem cells which might impair bone healing at the treated site. The technique has an added benefit of stretching the soft tissue and therefore avoiding the need for soft tissue grafting. Distraction is mainly employed in augmenting the ridge in a vertical direction and a secondary bone grafting procedure for horizontal augmentation is often necessary. Figure 14 (a–e) illustrates a case of severe vertical anterior maxillary loss after a road traffic accident which was successfully managed with a multidisciplinary approach and utilizing distraction osteogenesis.
Figure 14.
(a) Pre-operative photo showing loss of three maxillary incisors along with part of the anterior maxilla and intrusion of UR3 and UL2 due to severe road-traffic accident. (b) Placement of distractor after osteotomy cuts to allow movement of ‘coronal’ fragment. (c) Pre-distraction radiograph. (d) Post-distraction radiograph. (e) Post-distraction healing.
It should be remembered that, despite the use of these techniques, further grafting may be necessary at the time of implant placement with a combination of particulate autogenous and xenografts, as can be seen in Figure 15 (a–d).
Figure 15.
(a) Implant placement with dehiscence. (b) Correct 3-D implant position despite alveolar width deficiency. (c) Additional sGBR. (d) Provisional 3-unit bridge. A significant reconstruction of the hard and soft tissue has been achieved.
Occasionally, soft tissue deficiency may be encountered and connective tissue grafts or free gingival grafts may be necessary to improve the soft tissue profile of the site. These grafts are harvested from the palate and therefore require a second surgical site. Geistlich Mucograft, a porcine-derived collagen matrix, has become available as a substitute and therefore would aid in reducing patient morbidity, as a donor site surgery is not needed. This will be covered in Part 2 of this short series.
In certain clinical situations, it may not be possible to regain the hard and soft tissues that have been lost after a traumatic event completely. In such instances, a compromised aesthetic outcome should be expected. The final aesthetic results may possibly be enhanced with the use of pink-coloured porcelains or composites, which are used to mimic the lost tissues (Figure 16a–c).
Figure 16.
(a) Patient suffered a dento-alveolar fracture resulting in loss of four incisors and part of the anterior maxilla. (b) Two implants with sGBR were placed in lateral incisor sites to retain a four-unit bridge with gingiva-coloured porcelain. (c) Acceptable aesthetic outcome in a patient with a low smile line.
Conclusion
This article describes the events following loss of a tooth and has covered some of the preparatory phases involved prior to the placement of dental implants. Various strategies that should be considered after traumatic loss of teeth have been described. These stages should not be overlooked in an effort to expedite definitive treatment as they may impact significantly on the final outcome. The second part of this series will cover the implant treatment in detail.