Daudt Polido W, Aghaloo T, Emmett TW Number of implants placed for complete-arch fixed prostheses: a systematic review and meta-analysis. Clin Oral Impl Res. 2018; 29:154-183
Weintraub JA, Orleans B, Fontana M Factors associated with becoming edentulous in the US Health and Retirement Study. J Am Geriatr Soc. 2019; 67:2318-2324
Kailembo A, Preet R, Stewart Williams J. Common risk factors and edentulism in adults, aged 50 years and over, in China, Ghana, India and South Africa: results from the WHO Study on global AGEing and adult health (SAGE). BMC Oral Health. 2016; 17 https://doi.org/10.1186/s12903-016-0256-2
Kassebaum NJ, Smith AGC, Bernabé E Global, regional, and national prevalence, incidence, and disability-adjusted life years for oral conditions for 195 countries, 1990–2015: a systematic analysis for the global burden of diseases, injuries, and risk factors. J Dent Res. 2017; 96:380-387
Bhering CLB, Mesquita MF, Kemmoku DT Comparison between all-on-four and all-on-six treatment concepts and framework material on stress distribution in atrophic maxilla: a prototyping guided 3D-FEA study. Mater Sci Eng C Mater Biol Appl. 2016; 69:715-725
Horita S, Sugiura T, Yamamoto K Biomechanical analysis of immediately loaded implants according to the ‘All-on-Four’ concept. J Prosthodont Res. 2017; 61:123-132
Sailer I, Strasding M, Valente NA A systematic review of the survival and complication rates of zirconia-ceramic and metal–ceramic multiple-unit fixed dental prostheses. Clinical Oral Implants Research. 2018; 29:184-198
Sailer I, Balmer M, Hüsler J Comparison of fixed dental prostheses with zirconia and metal frameworks: five-year results of a randomized controlled clinical trial. Int J Prosthodont. 2017; 30:426-428
Mangano C, Iaculli F, Piattelli A Fixed restorations supported by Morse-taper connection implants: a retrospective clinical study with 10–20 years of follow-up. Clin Oral Implant Res. 2015; 26:1229-1236
Papaspyridakos P, Barizan Bordin T, Kim Y-J Implant survival rates and biologic complications with implant-supported fixed complete dental prostheses: a retrospective study with up to 12-year follow-up. Clin Oral Implants Res. 2018; 29:881-893
Ali K, Kay EJ. What are the long-term survival and complication rates of complete-arch fixed implant rehabilitation in edentulous patients?. Evid Based Dent. 2019; 20:97-98
Tribst JPM, Dal Piva AM de O, Borges ALS Does the prosthesis weight matter? 3D finite element analysis of a fixed implant-supported prosthesis at different weights and implant numbers. J Adv Prosthodont. 2020; 12:67-74
Joda T, Zarone F, Ferrari M. The complete digital workflow in fixed prosthodontics: a systematic review. BMC Oral Health. 2017; 17
Pjetursson BE, Valente NA, Strasding M A systematic review of the survival and complication rates of zirconia-ceramic and metal-ceramic single crowns. Clin Oral Impl Res. 2018; 29:199-214
Sailer I, Strasding M, Valente NA A systematic review of the survival and complication rates of zirconia-ceramic and metal-ceramic multiple-unit fixed dental prostheses. Clin Oral Impl Res. 2018; 29:184-198
Fehmer V, Mühlemann S, Hämmerle CH, Sailer I. Criteria for the selection of restoration materials. Quintessence Int. 2014; 45:723-730 https://doi.org/10.3290/j.qi.a32509
Ali Z, Eliyas S, Vere JW. Choosing the right dental material and making sense of the options: evidence and clinical recommendations. Eur J Prosthodont Restor Dent. 2015; 23:150-162
Schnabl D. Prosthetic rehabilitation of partially edentulous patients: fixed – removable – combined? Metal–ceramics – all-ceramics? Implants? Anything goes! Part 2: two case studies represent the fixed, respectively the combined fixed-removable prosthetic restoration by utilization of implants. Swiss Dent J. 2015; 125:155-161
Pihlaja J, Näpänkangas R, Raustia A. Early complications and short-term failures of zirconia single crowns and partial fixed dental prostheses. J Prosthet Dent. 2014; 112:778-783
Larsson C, von Steyern PV. Ten-year follow-up of implant-supported all-ceramic fixed dental prostheses: a randomized, prospective clinical trial. Int J Prosthodont. 2016; 29:31-34
Metal–Ceramic implant-supported fixed dental prostheses: the gold standard for the completely edentulous patient. A case report Adel Martínez Martínez María del Pilar Lujan-Pardo Stephanye Ariza-Martínez Dental Update 2024 49:7, 707-709.
Authors
Adel MartínezMartínez
Professor, Gitouc Investigation Group, Faculty of Dentistry, University of Cartagena, Cartagena, Colombia
The development of implantology has allowed implant-supported fixed prosthetic treatments in edentulous patients to become the main alternative to conventional rehabilitation. The dental experience of edentate patients comprises an extensive history of successes and failures with traditional rehabilitation. The following report describes a case of a completely edentulous patient who recovered oral function and aesthetics by placing six implants in each jaw and, subsequently, restoration with metal–ceramic implant-supported fixed dental prostheses (FDPs). The authors explore the criteria that must be considered for the selection of the material to be used in implant-supported fixed prostheses.
CPD/Clinical Relevance: To ensure enhanced survival rates for implant-supported fixed prosthetic restorations in edentulous patients, patient factors, their expectations, the number of implants to be placed and the materials to be used must be carefully considered.
Article
Adel Martínez-Martínez
Edentulousness can be partial or complete.1 For dentists, this is one of the most complex situations to address owing to its multifactorial aetiology and the impact it has on systemic and emotional health, as well as the functional and aesthetic compromise it represents. Different factors have been linked to the premature tooth loss that has lead to the partial or complete edentulism. Among them are low educational level, smoking, diabetes, poor general health of the individual, physical limitations or disabilities, and few or no visits to the dentist.2 Since oral health is essential for general health, function and wellbeing, and considering that, worldwide, oral health has not shown improvements in the last 25 years3,4 it is necessary to provide alternatives for edentulous patients that allow them to restore function, aesthetics and self-esteem.
The evolution of osseo-integration has allowed implant-supported prosthetic treatments in edentulous patients to become the main alternative to conventional rehabilitation with a complete denture. Implant-supported prosthetic options range from removable overdentures supported on two or four implants, to hybrid metal–ceramic, zirconia–ceramic, and hybrid acrylic prostheses with all-on-four or all-on-six techniques, with immediate or delayed loading.5–7 Survival rates differ according to the prosthetic material employed, being 98.7% at 5 years for metal–ceramic implant-supported prostheses and 93.0% for zirconia–ceramics. According to some reports, the risk of fracture and chipping is 11.6% for the metal–ceramic prosthesis compared with a significant 50% for the zirconia–ceramic.8,9 Several studies report high survival rates in implants managed with fixed restorations. In Mangano et al,10 survival was 97.2% at 20 years. On the other hand, Papaspyridakos et al reported 5- and 10-year survival rates of 98.7%,11 and Ali et al12 published survival rates of 99.4% for implants and 98.2% for full-arch fixed metal–ceramic prostheses.
The number of implants and the weight of the full-arch prosthesis influence the strain generated on the bone. In their 3D finite element analysis, Tribst et al demonstrated that prostheses with masses between 10 g and 60 g and supported by four or more implants do not generate bone strain.13
In this article, the authors report a case of a completely edentulous patient, managed with metal–ceramic FDPs supported by six implants in each jaw.
Case report
A 62-year-old female patient, with complete edentulism, who had worn dentures for more than 20 years, requested a fixed prosthetic solution (Figure 1). Clinical examination showed edentulous alveolar ridges, covered by healthy gingiva, without signs of infection, inflammation, or presence of residual dental roots. Imaging studies revealed moderate bone resorption in height and width in both jaws from the anterior to the premolar region. The molar area showed severe resorption, with maxillary sinus floor pneumatization and close proximity of the inferior dental canal to the edentulous ridge. According to the clinical and imaging findings, the ridges were classified following the guidelines proposed by Cawood and Howell, as class IV ridges and bimaxillary complete edentulism.
Figure 1. Initial condition, prominent labial, and nasolabial folds are observed.
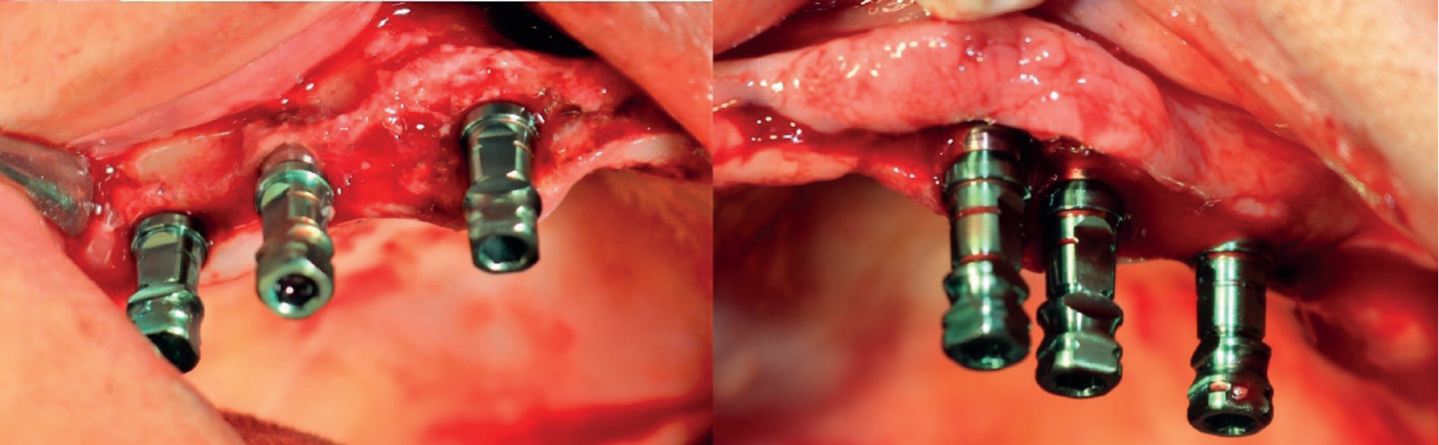
The proposed treatment plan included six Zimmer-Biomet Inc (USA) dental implants for each jaw with left maxillary sinus floor augmentation and immediate implant placement. This would be followed by rehabilitation with metal–ceramic implant-supported hybrid prostheses, with gingival tissue characterization to obtain proper labial support. In the upper jaw, under local anaesthesia, a bone expansion technique with osteotomes was performed for placement of a Tapered Screw-Vent Implant System (Zimmer Biomet Dental Inc) in UR3-UR5-UR6, and maxillary sinus floor augmentation was conducted in UL6 to place implants in UL3-UL5-UL6 (Figure 2). In a second session, implants were placed in the lower jaw from LR5 to LL5.
Figure 2. TSV implants: Zimmer in position, right and left sides.
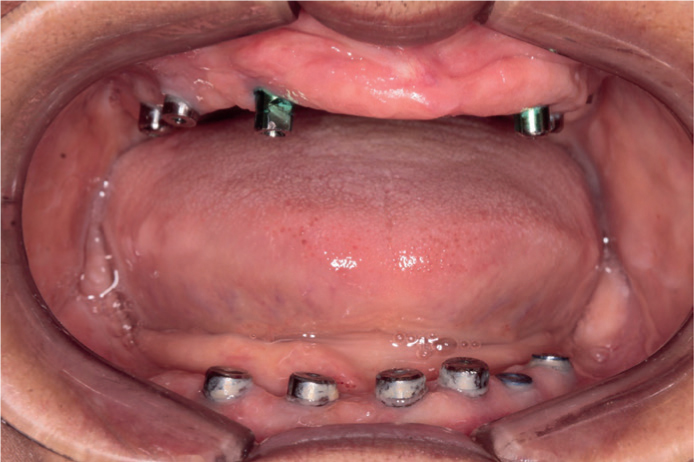
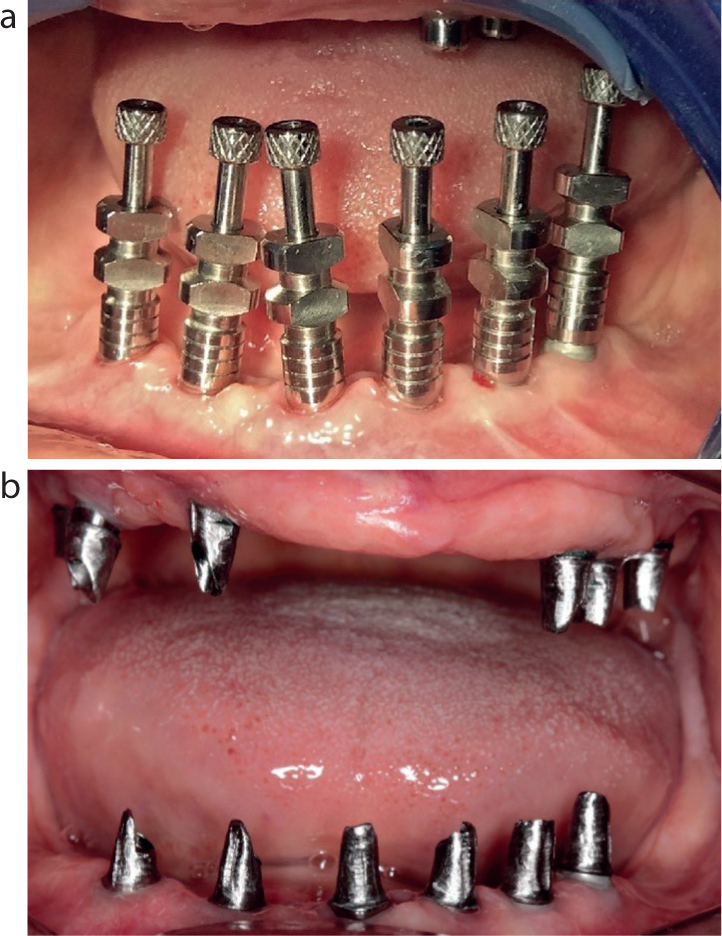
Six months after clinical and radiographic checks, and after confirming adequate osseo-integration, the restorative phase began (Figure 3). An open-tray technique with impression copings was used. Copings were splinted with pattern resin and the impression was cast in type IV plaster. On the working cast, record bases with wax rims were made for a jaw registration to determine vertical dimension, position, size of the teeth, smile line, profile, and facial fullness of the patient (Figure 4a). Once these aspects were determined, the cast was sent to the laboratory to prepare the abutments and design the structures. A first test for the verification jig of the working casts, the abutments, and the structures in polymethylmethacrylate (PMMA) was tried in the patient to check the precision of the position of the implants in the plaster model and parallelism of the definitive abutments (Figure 4b). The super structures were cast in Cr-Co, and a second try-in was carried out to verify accuracy (Figure 5). In the laboratory, ceramic layering was performed for the dental area with pink ceramic for the characterization of the gingiva. The final try-in of the prostheses was completed to check occlusion, the result was approved by the patient and she gave her consent for placing the screwed cement bridge. The objective of restoring function and self-esteem to the patient was achieved (Figure 6). Additionally, instructions were given about the special care of the prostheses, and review was indicated every 6 months.
Figure 3. Intra-oral condition 6 months after surgery. Notice the healing caps and temporary abutments.Figure 4.
(a) Open-tray impression technique. Note the impression copings in position. (b) Abutments prepared in the laboratory: first test in the patient.Figure 5.
(a) CAD/CAM metal structures. (b) Final restoration, metal–ceramic fixed dental prostheses.Figure 6. Extra-oral view before and after treatment. Notice the aesthetic when the patient smiles.
Discussion
The presence of a metal superstructure, in this case, the Cr-Co alloy, reduces prosthetic complications associated with fractures and it creates ideal support for the ceramic material. The presence of a metal occlusal surface can improve wear resistance and help maintain the vertical dimension; however, the appearance can be compromised. The inclusion of CAD/CAM technology has allowed the use of aesthetic restorative materials, such as zirconia, for fixed implant-supported prostheses, with some success.14
Although the aesthetic result is one of the main factors to be considered in these cases, the survival of the dental prosthesis and implants with few complications, whether a fixed metal–ceramic or all-ceramic prosthesis is used, remains important for clinicians. A 2018 systematic review by Pjetursson et al15 reported on the survival rate and complications for zirconia-based and metal–ceramic implant-supported single crowns (SCs). The meta-analysis revealed a 98.3% 5-year survival rate for metal–ceramic implant-supported SCs compared to 97.6% for zirconia implant-supported SCs. For the metal restorations, 86.7% experienced no technical or biological complications, while 83.8% of the zirconia restorations met this objective. The incidence of chipping was similar between the two materials; however, a greater number of failures due to fracture were reported in the zirconia restorations (2.1% versus 0.2% for the metal–ceramic implant-supported SCs). The clinical case presented by the authors was a metal–ceramic implant-supported fixed dental prostheses. There were no complications in a 2-year follow-up and no fractures.
A systematic review by Sailer et al16 evaluated the survival rate and complications of zirconia–ceramic and/or monolithic zirconia implant-supported FDPs versus metal–ceramic FDPs. The study reported a higher number of cases treated with metal–ceramic FDPs (n = 932) compared to zirconia-ceramic FDPs (n = 175), which suggests that clinicians had a preference for metal–ceramic implant-supported restorations to rehabilitate completely edentulous patients. The survival rates of metal–ceramic implant-supported FDPs was 98.7% versus 93% for zirconia implant-supported FDPs) and there was a low incidence of fractures and chipping was reported (11.6% versus 50% for zirconia implant-supported FDPs).16 All of which make metal–ceramic restorations the gold standard for implant-supported fixed prostheses, especially in cases of multiple implants in bimaxillary edentulous patients. 17–19
Ceramic chipping in zirconia prostheses is the most frequently described complication.20 Larsson et al21 reported rates of more than 50% for this complication in implant-supported prostheses, despite advances in the quality of zirconia and prosthetic fabrication techniques.
Currently, there is insufficient evidence in the literature to support the use of metal-free materials for implant-supported fixed prostheses over traditional materials. Poggio et al22 recommended selecting the restorative material based on clinical experience and the individual needs and preferences of each patient. The authors of this report support this view and advocate the use of a metal–ceramic superstructure for full arch fixed-implant bridges.
Conclusions
The success of the rehabilitation in edentulous patients in whom the placement of dental implants is considered will depend on many factors, such as the experience of the team, the quantity and quality of the maxillary bone, and the material to be used in the prosthetic restoration. Since Brånemark's original design of the removable fixed prosthesis over implants, there have been many changes. The Brånemark prosthesis consisted of a gold alloy framework attached to implant copings. The teeth of the acrylic resin prosthesis were placed on the framework and secured with acrylic resin. The main drawbacks to this type of restoration were the distal extension fractures due to the extensive cantilever. In the case reported here, the authors designed the ceramic bridge implant with the hybrid technique, in which the ceramic prosthesis is cemented onto the titanium superstructure with resinous cement, and subsequently screwed onto the implants, thus allowing occlusal access to remove the prosthesis. Additionally, the cement settles passively and does not invade the peri-implant mucosa. The authors suggest that the gold standard construction for a full arch implant-supported fixed prostheses would use metal–ceramic.