Jordan R, Adab P, Cheng K. Covid-19: risk factors for severe disease and death. BMJ. 2020; 368
Sohrabi C, Alsafi Z, O'Neill N World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020; 76:71-76
Horby P, Lim W, Emberson R Dexamethasone in hospitalized patients with Covid-19 — preliminary report. N Engl J Med. 2020; https://doi.org/10.1056/NEJMoa2021436
Wise J. Covid-19: arthritis drugs improve survival in intensive care patients, shows study. BMJ. 2021; 372
Willan J, King A, Jeffery K, Bienz N. Challenges for NHS hospitals during covid-19 epidemic. BMJ. 2020; 368
Fraher E, Pittman P, Frogner B Ensuring and sustaining a pandemic workforce. N Engl J Med. 2020; 382:2181-2183
Grossman S, Sandhu P, Sproat C, Patel V. Provision of dental services at a single institution in the UK's epicentre during the COVID-19 pandemic. Br Dent J. 2020; 228:964-970
Hall L, Johnson J, Watt I Healthcare staff wellbeing, burnout, and patient safety: a systematic review. PLoS One. 2016; 11
Johnson EL, Smith J, Arwel CF, Pancholi R. The tooth about Nightingale: a reflection on redeployment to Nightingale Hospital London. Dent Update. 2020; 47:565-568 https://doi.org/10.12968/denu.2020.47.7.565
Redeployment of dental teams during the covid-19 pandemic: A review of experiences and lessons learned Christopher Platais Francesca Siodlak Ishpinder Toor Louise Ormondroyd Dental Update 2024 48:2, 707-709.
Authors
ChristopherPlatais
BDS(Hons), BMedSci, MFDS RCS Ed
DCT2 in Dental and Maxillofacial Radiology, Guy's Hospital, London
The COVID-19 pandemic has spread across the globe, causing millions of cases and disrupting the lives of people worldwide. The increase in the number of critically unwell patients has put healthcare systems under immense strain, requiring them to adapt their service provision to cope with increased demand. At Guy's and St Thomas' NHS Foundation Trust (GSTFT) in London, redeployment of healthcare staff has been used to relieve pressure on the most overburdened hospital sectors, and this saw clinical dental teams involved in auxiliary medical roles throughout much of 2020. On the cusp of the New Year, COVID-19 cases continued to soar and GSTFT opted to cancel routine care and re-implement a second round of clinical redeployment. Here, we discuss our experiences and present positive feedback of early-career dentists being redeployed to medical wards during the UK's greatest health crisis of recent years.
CPD/Clinical Relevance: Clinical dental teams can positively contribute to the national COVID-19 response through the provision of urgent dental care, inpatient mouthcare services and auxiliary medical roles.
Article
Since early 2020, the world has watched with trepidation as the COVID-19 pandemic has caused more than 90 million cases and almost 2 million deaths worldwide. The UK confirmed its first case on 31 January 2020 and, as of January 2021, the country has the fifth-largest national death toll; exceeded only by Mexico, India, Brazil and the USA.1
At Guy's and St Thomas' NHS Foundation Trust (GSTFT) in Central London, part of the initial COVID-19 response involved redeployment of clinical dental teams to a variety of secondary care roles. This provided an opportunity for dental staff to learn from a range of specialties while also contributing to essential health services. After a brief summer hiatus, cases of COVID-19 have continued to escalate with a new, more-transmissible coronavirus variant being widely implicated. This has led to the implementation of a further national lockdown, and at GSTFT, further restructuring of healthcare services and associated redeployment of dental teams. Here, we reflect on our experiences and the lessons learned from our involvement in the first COVID-19 response.
COVID-19
COVID-19 is an infectious respiratory illness caused by the coronavirus SARS-CoV-2, which is primarily transmitted via droplets.2 The clinical presentation of COVID-19 varies between individuals, with many infections leading only to mild or moderate symptoms. Approximately 15% of those infected develop severe symptoms that require management with supplemental oxygen and a further 5% become critically unwell.3 The most severe complications of COVID-19 include pneumonia, acute respiratory distress syndrome (ARDS), septic shock, thrombo-embolism and multi-organ failure. Comorbid illness, obesity and old age increase the risk of severe symptoms.4
At the time of writing, there is no targeted treatment available for COVID-19 and the mainstay of management is supportive care.5 Despite this, there have been reports of improved survival with dexamethasone, tocilizumab and sarilumab.6,7 Additionally, three vaccines have been approved for use in the UK to date, and the NHS is currently underway with the rollout of a vaccination programme designed to prioritize those who are most vulnerable to COVID-19. Until these pharmaceutical approaches are developed and widely implemented, the priority continues to be prevention of viral transmission and simultaneous improvement of the healthcare system's ability to respond.
Mobilizing NHS healthcare provision
The initial surge in critically unwell COVID-19 patients presented many challenges to the NHS' infrastructure and workforce.8 Intensive care units (ICUs) underwent rapid expansion to maximize capacity by repurposing wards and theatres, recommissioning private facilities and even constructing temporary critical care Nightingale hospitals. Across the UK, elective treatment was postponed to facilitate this expansion and to allow clinical staff to be redeployed to the most overburdened hospital sectors.9
During this first wave of COVID-19, all non-urgent dental care was postponed and urgent dental care (UDC) was delivered through designated regional centres, including the adaptation of GSTFT's existing UDC pathway into an enhanced multi-discipline point of access.10,11 At the time, dental teams had wide-ranging remits that included UDC provision and redeployment to renal dialysis units and ICU.
In many respects, the current situation in 2021 is similar to that of early 2020. At the time of writing, the number of COVID-19 positive patients receiving mechanical ventilation within UK hospitals is greater than at any point in 2020,12 and the population has been recently placed under a national lockdown mandating that people stay at home to protect the NHS and save lives.13 In response, GSTFT has cancelled routine care and instigated a second round of clinical redeployment; many dental staff have been relocated in much the same way as in 2020, albeit with a significant proportion now allocated to assist with the newly implemented vaccination programme.
Intensive care
During the COVID-19 surges, GSTFT ICUs were drastically restructured to improve capacity and this involved repurposing a number of clinical areas to give a total of nine ICU wards over the two hospital sites.14 Strict protocols for zoning were also implemented to reduce the risk of transmission to patients and staff, including the introduction of designated areas for the donning and doffing of enhanced personal protective equipment (PPE). A key component of this PPE was the filtering facepiece level 3 (FFP3) mask, which provides a greater level of protection against aerosols compared to standard medical masks. These FFP3 masks required specific fit-testing to ensure that the masks formed an adequate peripheral seal, and drop-in testing sessions were arranged for all critical care staff.
Proning
Proning is a method of repositioning ventilated patients so that they lie prone, or face-down. This position leads to recruitment of alternative lung regions and enhanced drainage of airway secretions, which can be used to maximize ventilation and reduce mortality for patients with severe ARDS.15
Safely proning a patient can require up to seven clinicians, including an airway-trained doctor, and is therefore associated with a significant staff burden. The implementation of a designated team enabled proning to take place without disrupting the nursing care of patients in adjacent bed spaces. During the height of the pandemic, this service operated 24 hours a day, seven days a week and covered the nine ICU wards on an on-call basis.
Mouthcare
Oral health deteriorates rapidly following the onset of critical illness because of limited access for oral care, compromised immunity and reduced saliva flow; these factors predispose patients to oral and respiratory infections.16,17 Ventilator-assisted pneumonia (VAP) and hospital-acquired pneumonia (HAP) are two serious complications that can lead to prolonged treatment duration and an increased risk of mortality in patients that have compromised respiratory function due to COVID-19.
In late April 2020, Public Health England released guidance outlining the standards for provision of mouthcare for critically unwell COVID-19 patients.18 A mouthcare service aimed at delivering these standards was approved by GSTFT and, in under a week, the dental directorate had trained staff and rolled out a dentist-led service for COVID-19 patients across all ICU wards. This service aimed to provide oral assessments and deliver twice-daily mouthcare for each ICU patient, but dentists were also well placed to liaise with the medical team regarding possible dental causes of infective endocarditis, candida infection, xerostomia and identification of mobile teeth or retained dentures that could pose a potential inhalation risk.
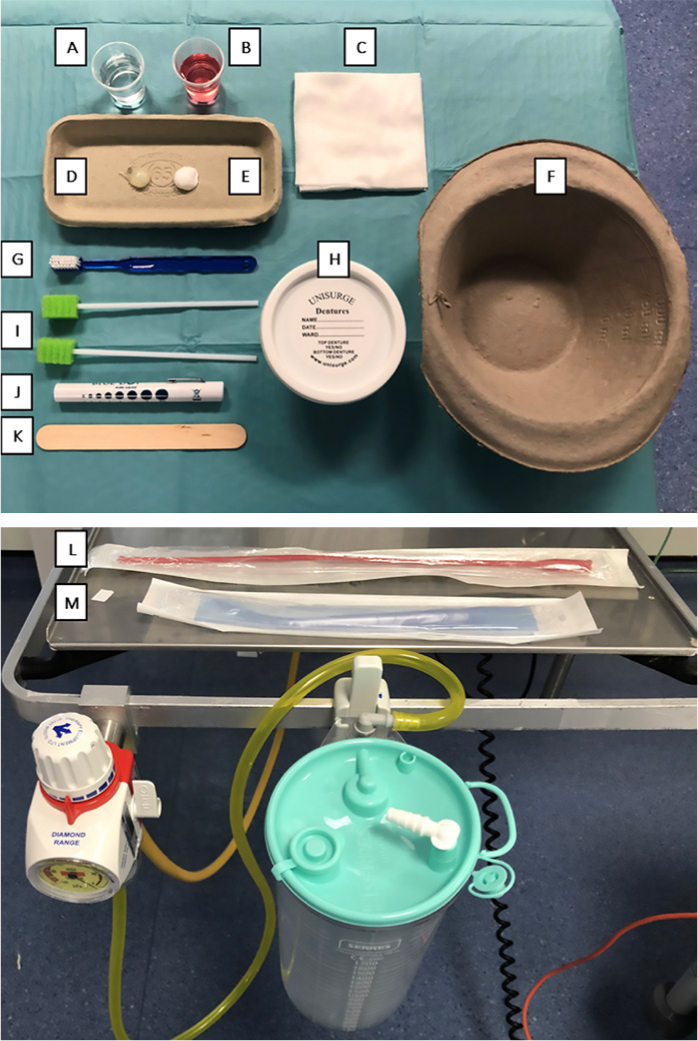
Self-performed or assisted mouthcare was encouraged as an important step towards rehabilitation for those non-ventilated patients who were able. For the remainder, clinician-performed mouthcare typically involved cleaning of the oral mucosa with 0.2% chlorhexidine gluconate solution applied via a mouth swab, and toothbrushing with fluoridated toothpaste and a small-headed, soft bristle brush. Excess material was then removed with the appropriate suction, and the lips cleaned with damp sterile gauze prior to application of paraffin wax to provide lubrication and reduce mucosal trauma from the endotracheal tube holder. An image of the available materials can be seen in Figure 1.
Figure 1. Photographic representation of the available materials for mouthcare provision in a critical care setting. A: sterile water; B: chlorhexidine gluconate (0.2%); C: sterile gauze; D: paraffin wax; E: fluoridated toothpaste (1350ppm); F: disposable spittoon bowl; G: toothbrush; I: mouth swabs; J: pen torch; K: wooden tongue depressor; L: Ruche suction; M: Yankauer suction.
Renal
The kidney is often affected in severe COVID-19 cases, with up to 36% of hospitalized patients developing acute kidney injury.19 Additionally, patients with pre-existing kidney disease continued to rely on regular haemodialysis, a method of removing waste products and excess water from the blood. Dental teams were redeployed to the dialysis units to mitigate the effects of potential increased patient admission during a time of predicted staff sickness and self-isolation.
An effective triage system to screen for potential COVID-19 cases prior to admission is important because these patients are generally immunocompromised, which increases the risks associated with contracting COVID-19. Dental teams carried out COVID-19 screening assessments, including tympanic temperature readings, before allocating an appropriate bed space. From here, they recorded basic observations, such as weight, blood pressure and pulse rate, and were trained to prepare the clinical environment, including lining the dialysis machines.
Staff wellbeing
The COVID-19 pandemic has caused great uncertainty for much of the general population, and concerns over safety and changes to everyday routine have brought with it a period of stress and anxiety, which in turn has negative implications for psychosocial wellbeing. Redeployed clinical staff often found themselves in unfamiliar, high-pressure environments. To help clarify the considerations for mental health, the World Health Organization (WHO) released a position statement in March 2020.20 Staff wellbeing is of paramount importance for ensuring ICUs are well managed, and this has direct implications for patient outcomes.21
At GSTFT, there was an increased emphasis on providing staff wellbeing services, including regular staff emails to outline available support, free subscription to self-care smartphone apps, free and discounted meals during work shifts and even access to wellbeing zones that included options for massage and aromatherapy. An integral component of the wellbeing service was access to psychology teams in the form of one-to-one counselling and group therapy sessions. Support groups were also available to staff who returned to their home departments, with protected time to attend these sessions within the working day.
Staff feedback
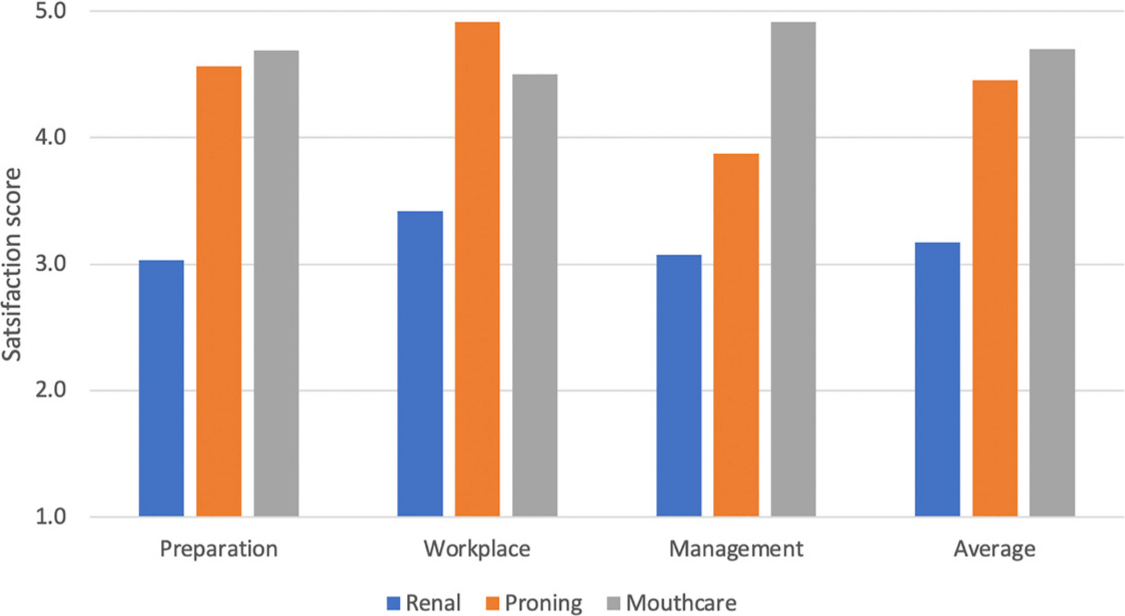
To gain insight into the preparedness of dental staff undergoing redeployment in secondary care, we collected feedback from the dental cohort at GSTFT using anonymous questionnaires to assess their views of training, clinical duties and management of their redeployment. The questions used to assess these domains can be seen in Table 1, with respondents asked to provide a numerical satisfaction score. The resultant data is shown in Figure 2 and reveals that dental staff generally viewed redeployment across each of the three services positively. Some of the differences seen between the services could be due to staff's perception of how their clinical skillset was used, and indeed a number of respondents noted that they felt unclear of their role within the renal department, while the mouthcare service was likely to feel more familiar.
Domain
Question
Preparation
Were you satisfied with the quality of training prior to starting?
Were you satisfied with the guidance and training provided during your shifts?
Did you feel adequately prepared to work in the department?
Did you feel you received all the necessary non-clinical information, eg location of changing rooms, scrubs, lockers?
Workplace
Did you feel comfortable working on the department?
If you had any questions or concerns while in the department, were you adequately supported?
Would you feel comfortable working within the department in the future?
Management
Did you feel you were kept informed of all relevant developments?
Did you receive the rota with enough notice?
Did you have the flexibility to attend work-related or personal commitments?
Did you feel happy raising any concerns?
Were the concerns you raised addressed sufficiently?
Figure 2. Bar chart to summarize the satisfaction scores, per feedback domain, for each department. All three departments were considered positively, with ICU considered more positive than renal. Respondents felt that the mouthcare service required the most preparation and was the best managed, but the proning service scored highest in the workplace.
In the authors' view, working alongside critical care teams during the COVID-19 pandemic was a valuable experience that gave a wider perspective of general patient care. The work within the proning service provided insight into the extent of the healthcare response that was required to navigate through this health crisis. Some of our patient encounters were positive, and we often witnessed steady weekly improvements in condition that led to patients being stepped down from critical care. Conversely, the proning service was reserved for treating the most unstable of patients, and we, unfortunately, also encountered loss of life while working with this cohort. These situations brought home the importance of a combined healthcare response and working alongside such a diverse mix of redeployed healthcare professionals was a humbling experience. Our time on the dialysis units allowed us to gain further insight into renal medicine, which will no doubt be beneficial in understanding the medical histories of our dental patients, such as an enhanced awareness of bleeding risk due to anticoagulation and immunosuppression due to transplant medications. Working within the mouthcare service felt closer to home, and it was good to use our dental skillset after weeks spent in general medical settings.
Redeployment across these three services during the COVID-19 response has provided a rich learning opportunity. We have furthered our clinical knowledge, improved teamworking skills and gained insight into the challenging and varied roles of our medical colleagues; these experiences will no doubt stay with us throughout our future careers.
Future steps
Much has been learned from the initial period of redeployment. Dental staff worked alongside a varied cohort of clinicians and our hope is that these working relationships will benefit our patients through the comprehensive provision of multidisciplinary care. There have since been talks with critical care and the allied health professions aimed at improving the provision of mouthcare for medical inpatients, and dental staff have been instrumental in formulating mouthcare training modules for ICU teams. Additionally, the dental directorate is holding initial stakeholder meetings to further evaluate the pathways available to GSTFT patients who require dental intervention after admission to medical wards.
The UK's COVID-19 pandemic is escalating and GSTFT has responded by rapidly restructuring its clinical services for a second time. Once more, dental staff find themselves on proning and mouthcare teams, and we encourage ongoing evaluation of these services to ensure that they continue to be effective and well received. For the first time, dental staff are being redeployed to the NHS COVID-19 vaccination programme, which to many signals the beginning of an important step towards controlling the pandemic and restoring an element of normality. Further evaluation and feedback from staff involved in these programmes is required to assess their efficacy and determine whether similar approaches to staff management should be implemented if required in the future. The success of clinical redeployment within secondary care additionally raises the question of whether primary care dentists could be similarly used; indeed, there are some who already have first-hand experience of redeployment to the Nightingale hospitals.22
Conclusion
Despite an initial hiatus, COVID-19 transmission and mortality have resurged in the UK and a government-enforced national lockdown has been introduced to protect an overburdened NHS. Clinical redeployment was well used during the first wave of the pandemic; the lessons learned from evaluation of our services have helped to ensure prompt mobilization in an attempt to counteract the increased strain on the NHS from this subsequent COVID-19 wave.