Ward DH. A study of dentists' preferred maxillary tooth width proportions: comparing the Recurrent Esthetic Dental Proportion to other mathematical and naturally occurring proportions. J Esthet Restor Dent. 2008; 19:324-329
Kelleher M. Dental Bleaching. Quintessentials of Dental Practice – 38.London: Quintessence Publishing Co Ltd; 2007
Rosenstiel SF, Gergafuff AG, Johnson WM. Randomised clinical trial of the efficacy and safety of a home bleaching procedure. Quintessence Int. 1996; 27:413-424
Russell CM, Dickinson GL, Johnson MH Dentist-supervised home bleaching with 10% carbamide peroxide gel: a 6 month study. J Esthet Dent. 1996; 8:177-182
Fordham N, Lewis M, Naseem S. Aesthetic midline re-alignment using CADCAM technology and Straumann Zerion. Dentistry. 2012; Spring:10-11
Saunders WP, Saunders EM. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:137-140
Felton D, Madison S, Kanoy E Long term effects of crown preparations on pulp vitality. J Dent Res. 1989; 68
Edelhoff D, Sorenson JA. Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent. 2002; 87:503-509
Burke FJT, Lucarotti PSK. Ten year outcome of crowns placed within the general dental services in England and Wales. J Dent. 2009; 37:12-24
Burke FJT, Lucarotti PSK. Ten year outcome of porcelain laminate veneers placed within the general dental services in England and Wales. J Dent. 2009; 37:31-38
Kelleher MGD. The ‘daughter test’ in aesthetic (‘esthetic’) or cosmetic dentistry. Dent Update. 2010; 37:5-11
Ethical marketing in ‘aesthetic’ (‘esthetic’) or ‘cosmetic dentistry’ part 1 Martin G D Kelleher Serpil Djemal Nicholas Lewis Dental Update 2024 39:5, 707-709.
Authors
Martin G DKelleher
BDS, MSc, FDS RCPS, FDS RCS
Consultant in Restorative Dentistry, King's College Hospital, London SE5 9RS, UK
Prior to undertaking any elective, ‘cosmetic’ dental procedures, it is vital for the treating dentist to discuss the merits and drawbacks of all viable options. It is important that the patient understands what the consequences and limitations of treatment are likely to be, and what the potential failures could entail later in his/her life. Informed consent should be obtained (preferably in writing) and the clinical notes and records should be clearly documented, with accurate and concise details provided of all the investigations carried out, and their findings, as well as including details of the various discussions that have taken place. Dentists need to be aware of the existence of heightened expectations in this group of patients and be cautious about accepting patients who have unrealistic ‘cosmetic’ expectations. Where possible, cosmetic or aesthetic dental treatment should be provided which is minimally destructive and, in the long term, be in the ‘best interests’ of the patient. Important matters such as the gaining of informed consent and maintaining meticulous, contemporaneous dental records will also be emphasized. It is hoped that the article will provide clear definitions of some commonly used terms such as ‘ethical marketing’, ‘ethics’, and ‘values’, which are often used in association with the marketing, planning and undertaking of supposedly ‘cosmetic’ dental procedures. The important role of less invasive alternative treatment options will also be emphasized.
Clinical Relevance: The aims of this article are to consider the common pitfalls that may arise when contemplating the marketing and provision of invasive, ‘cosmetic’, dental restorations and to discuss how best to avoid a dento-legal claim where such treatment plans may not fulfil the patient's desired outcome.
Article
Introduction and general considerations
The ethical marketing of aesthetic or cosmetic dentistry is a complex, difficult and potentially dangerous subject. It is complex because of the range of problems that present. It is difficult because of the perceptions of the patients who have those problems. It is dangerous because, in this particular arena, opinions are abundant and facts are rare.
It is possible sometimes to see quickly that the problem is an obvious physical one. However, more often than not, the reasons for the patient seeking cosmetic treatment are less obvious, or why the patient is seeking such treatment at this time may be shrouded in mystery.
Furthermore, these patients do not represent the ‘average patient.’ Their hopes, aspirations and expectations are sometimes difficult to discern. Some patients think that a change in their dental appearance will markedly improve their life. While this is possible, particularly if they have an obvious, easy to spot, physical problem, their expectation can be that beautifying the appearance of their teeth will lead to a better job, an improvement in their love life, or even long term success and happiness. Such patient hopes, wishes or aspirations need to be gently teased out in discussions with the patient early on and then challenged as appropriate.
It is unethical to provide treatment for patients whose ‘cosmetic’ aspirations are completely unrealistic, particularly if any such treatment involves destructive dentistry. It is important to understand an individual patient's hopes and expectations. If these are in any way unrealistic it is important to challenge these expectations early and sometimes brutally. This is part of the diagnostic and discussion process in aesthetic or ‘cosmetic’ dentistry. A finding at the beginning of treatment is called ‘a diagnosis’ and a finding at the end of treatment is called ‘an excuse’. The patient is the only person who can make the judgement as to whether a ‘cosmetic’ treatment is successful for them in the longer term. The unknown views of partners, lovers, friends, family and work colleagues all add to the dangers in treating such patients. Mild narcissism is one thing, but body dysmorphic disorder is a dangerous psychiatric condition of which dentists need to be very aware. The plastic surgery literature is replete with descriptions of the psychiatric state of patients presenting for plastic surgery and with the details of the very real problems that these can cause for the patients themselves and those who choose to deal with them.
The meaning of the word ‘cosmetic’
It is relevant to point out that the term ‘cosmetic’, while it is in common use in dentistry, actually has a specific meaning. The word is derived from the Greek ‘cosmetikos’, meaning adornment and, strictly speaking, should be used in relationship to things that are temporary, superficial and readily reversible. Cosmetics should not alter the material on which they are placed. Cosmetics do not damage the underlying structure on which they are placed. They have to be replaced every time one wants a particular look. ‘Cosmetic’ would usually relate to something like lipstick or eye shadow which will temporarily alter the area on which the cosmetic is placed. Such ‘cosmetics’ do not adhere to the underlying tissue and if one doesn't like the appearance, it is easy to remove the cosmetic and replace it with something that is more acceptable. There is a huge, lucrative, international cosmetic industry founded on this principle, much of which profits from, and preys on, some people's self image, vanities, or insecurities. Such cosmetics are exhaustively tested in various ways prior to their development and, following their manufacture, prior to being supplied. They are rarely dangerous as they have to be made available to a very wide range of consumers. In terms of dentistry, a diagnostic bond up with some direct composite being cured on to un-etched enamel in order to allow assessment by the patient and dentist could be considered to be ‘cosmetic’ because, used in that way, it is temporary, superficial, readily reversible, and does not, at that stage, adhere to, or change, the underlying tooth surface.
Fashions and ‘aesthetic dentistry’
The provision of aesthetic dentistry is usually undertaken to improve the beauty of the teeth, the smile, or the face, as perceived by the patient, or his/her partner, family or friends. The word aesthetic is derived from the Greek word ‘aisthetikos’ and is concerned with the perception, the philosophy or the study of beauty. There is nothing more controversial in dentistry than what constitutes ‘a beautiful smile’. If you were to ask 10 dentists to look at a patient's smile or teeth and ask for their comments about the attractiveness of that dental appearance, you would probably get 11 different opinions.1 These will range from the dentists who like the ‘natural look’ to dentists who prefer the ‘false teeth’ look. As in most areas of life there are fashions. Fashions come and go. In the early years of this century, ie from about the year 2000 to the present time, there has been an American dominated ‘All Teeth and Have a Nice Day’ look. This has led to the provision of ultra white, very even and sometimes big teeth. The whiteness of the teeth and their regularized, formulaic size changes, usually extending out widely, often has the effect of making the teeth and the mouth a really dominant part of the face. This ‘look’ has been popularized by various actresses, models and minor celebrities.
Very few of these actresses, celebrities or models would be candidates for Mensa and some people would call them ‘airheads’. However, many gullible, especially younger, people worship their celebrity status, money and lifestyle. There appears to have been a rise in the acceptance of the views of such ‘airheads’ on a variety of topics. Airheads are superficial and self absorbed. They are not concerned about themselves in the future and want provision of ‘The Look’ here and now. Many images appearing in glossy magazines, some of which deliberately target young people, are of airbrushed models that are heavily made up. The images are often ‘cropped and improved’ by various bits of computer technology before appearing in these magazines. This media bombardment often has a hard commercial edge and is likely to produce unrealistic expectations in younger, or gullible, people who, as a consequence, may well seek elective ‘cosmetic dentistry’.
However, unlike changing someone's hair or the colour of their skin with cosmetics or tanning (either by real sun or fake tan with various chemicals), the provision of dentistry for such patients is often a much more complex, irreversible and dangerous process. The promotion of such dentistry requires a very delicate balance between improving the patient's appearance and avoiding doing inappropriate and unnecessary biologic damage to the teeth, especially when any such treatment is viewed in the much longer term.
Aesthetic options and the range of treatments available
At one end of the spectrum is the provision of nightguard vital bleaching, which has been scientifically proven to be effective, safe and an excellent option for the removal of discoloration from dark teeth.2–4
In spite of such evidence from multiple, randomized, double blind, controlled clinical trials, it would be wrong to say that this technique never has any problems. For instance, if nightguard vital bleaching is used to bleach teeth that have got multiple composite restorations in them, then those composite restorations will not change colour and will require removal or, at the very least, to be resurfaced. The patient needs to know this before bleaching treatment is considered, because the costs of the removal and replacement of the restorations, including their biologic and financial costs, can be much greater than that involved in the provision of the nightguard vital bleaching itself.
It is part of a dentist's responsibility to provide that information to a patient before he/she is allowed to go away with the idea that this is a treatment that is completely lacking in risk. It has some risk, but this is very little if low concentration (10% carbamide peroxide gel) within a customized tray is used to provide the bleaching (Figures 1 and 2).2
Figure 1. Discoloured enamel due to fluorosis.Figure 2. Nightguard vital bleaching removes the brown discolorations without damaging the structure or strength of the teeth.
The potential problem of replacing existing composites in anterior teeth that are to be bleached is a relatively straightforward one. However, if there are teeth with much larger restorations, such as crowns, bridges or implant-retained crowns, in the same or in the opposing arch, which currently match the existing teeth, then bleaching adjacent or opposite teeth to make them look lighter will cause a mismatch in colour between the newly bleached teeth and the previously well-matched restorations. This change in colour may be acceptable, particularly if the crowns or bridges were lighter than the unbleached natural teeth (Figures 3–7). However, if these colour changes are unacceptable to the patient, this can then require them to have much more extensive dental treatments which can pose variable biologic risks and can have significant financial implications.
Figure 3. Patient presented with an existing bridge at UL3, UL4, UL5 and discoloured incisor teeth with existing composites.Figure 4. Lighter and opaque looking existing bridge with some local inflammation due to lack of interdental cleaning. No periapical radiolucencies.Figure 5. Bleaching of the natural teeth and replacement of the composites with lighter ones means that the existing bridge on the upper left-hand side does not need to be replaced because the bleached and bonded incisors and upper right canine are now an ‘acceptable’ match for it. Ethically, patients need to know that this is a viable alternative to replacing the bridge and veneering or crowning the other front teeth, which would be unnecessarily destructive of sound tooth tissue.Figure 6. Palatal view of upper arch showing defective composites and existing fixed-fixed PFM bridge.Figure 7. Palatal view of the bleached and direct composite bonded incisors which minimizes biologic and structural risk to the teeth in the longer term. Ethically, dentists need to remember to ‘firstly do no harm’. There has been minimal biological risk with this approach which maintains existing sound tooth structure unlike multiple veneers or crowns.
If bleaching has been provided, without a patient appreciating the consequences of that potential colour mismatch, then an individual patient might well expect those extensive restorations to be replaced by the dentist, or by any other provider of the bleaching, at the dentist's, or that other provider's, expense. This can often run into thousands of pounds. In this context, the colour mismatch problem has certainly been the source of litigation when dentists have refused to provide new restorations to match the newly bleached teeth. It is clear that over-the-counter, or internet-supplied, bleaching products have great potential to provide problems in this area. This is probably why it is prudent for patients wishing for an aesthetic improvement of their teeth to seek the advice and care of a responsible, well educated, sensible, honest and balanced dentist. Sadly, not all dentists fulfil these criteria. Few, if any, ‘beauticians’ or others providing supposed bleaching in shopping malls, ‘beauty spas’ or cruise ships would have the appropriate knowledge or skills to make these subtle judgements in advance of undertaking dental bleaching.
Problems of promotion and the media
A number of dentists are concerned, at least to some extent, with the ‘business of dentistry’ and seek to promote their practices mainly to gain ‘market share’ of a patient's disposable income and thereby to improve their own income. Some such dentists do this by means of advertising in various media, including their website, practice leaflets, signage, letters to patients and sometimes radio and television advertisements. Various articles showing ‘before and after’ pictures are promoted in a plethora of un-refereed, unscientific, glossy, ‘free’ dental publications.5
The probable intention of such articles in these advertisement strewn ‘dental business publications’ is to be able to demonstrate to potential patients that a wider audience has seen their work. What is missing in virtually all of these articles in these publications are the images of the prepared teeth showing, equally clearly, the damage that has been done to the teeth in order to provide the ‘before’ and ‘after’ supposedly cosmetic treatment (Figure 8).
Figure 8. This is a picture of what veneer preparations can look like. Patients ought to be able to visualize this as part of the consent process.
Television programmes, such as ’10 Years Younger’ and ‘Extreme Makeover’ provide evidence of a somewhat vacuous, mindless, cavalier, or what some might regard as a reckless approach to ‘cosmetic dentistry’. In these programmes it is clear that the provision of dental treatment is undertaken in a short period of time and that the speed of delivery is the dominant driving motivation for such treatments. There appears to be little evidence, in such programmes, of a serious attempt being made to provide balancing information to the patient in order to obtain his/her informed consent. Possibly, even if this is provided, it is often edited out of the final transmitted programmes to give the illusion to the general population and, indeed, to some watching, somewhat gullible, often younger dentists, that this is an acceptable ‘quick fix’ approach for aesthetic problems which does not have any long-term biologic consequences for the teeth.
Bearing in mind the destructive nature of the procedures undertaken to these teeth (frequently aggressively prepared for ceramic veneered restorations) in order to provide these changes rapidly, it is almost inevitable that there will be some longer term consequences caused by this amount of destruction of the residual sound tooth structure of the prepared teeth. A cursory glance at the dental literature will provide copious evidence of the long-term consequences of full coverage restorations. For instance, approximately 18% of teeth that are prepared for full coverage restorations may well be dead at five years, as shown by Saunders and Saunders6 and Felton, Madison and Kanoy, et al,7 respectively. Edelhoff and Sorenson have shown, in some elegant laboratory studies, that somewhere between 63% and 72% of tooth tissue is removed during the preparation for an anterior full coverage crown. It has also demonstrated that up to 30% of the sound tooth tissue may be removed by undertaking an extended veneer preparation (Figure 8).8 It is important that a patient should have a realistic understanding of these latter ‘balancing facts’, prior to embarking upon electively destructive dental treatment which may well have a profound impact on their future long-term dental health and appearance (Figures 9–11).
Figure 9. The preparation for all-ceramic crowns destroyed tooth structure and pulps. Was this ethical marketing? Did the patient really understand that this was a likely outcome? There were also a large number of other full coverage ceramic restorations present.Figure 10. A post preparation can help rescue the situation but has to destroy even MORE tooth structure.Figure 11. Ethical responsibility discharged? Was the patient told that they would lose 62–73% of the sound structure of his/her teeth for all-ceramic crowns?
Disclosing potential long term problems with aesthetic dentistry as part of informed consent
The ethical perspective is that patients do need to know the balancing ‘negative’ information before consenting to any elective ‘cosmetic’ dental treatment. Any marketing of procedures or products involved in the delivery of restorations such as full coverage, ceramic veneered, crowns need to be approached with extreme caution. Patients need to know (and it needs to be clearly documented that they did know and understood) what the risks were to their teeth in the long-term in having, or agreeing to have, such destructive things done to their teeth for short-term or medium-term improvement in their dental appearance. The younger the patient is when such treatment is done, the more likely it is that this will have an adverse, long-term outcome for the teeth. For instance, the provision of crowns below the age of 30 has been shown to have higher complication rates.9 It also needs to be fully appreciated by both dentist and patient that the removal of a huge amount of the structure of the tooth for a full coverage restoration will have long-term structural, not to mention pulpal, consequences.
Any dentist who promotes his/her practice and its interest in ‘cosmetic’ dentistry (especially when that often necessitates significant destruction of the crown of the tooth in order to provide, for example, a full coverage restoration just for cosmetic reasons) needs to remain aware that it is necessary to obtain the fully informed consent of a patient prior to doing that preparation. Not to tell the trusting patient in advance about the actual, or likely, amount of destruction involved in the provision of such restorations is likely to be considered unethical. If there are any problems, when such a patient finds out that there was a large amount of damage done to his/her tooth in order to provide the unacceptable outcome, they are frequently furious as to why they weren't clearly informed, and in writing, of the necessary preparations undertaken in order to provide such a restoration. Furthermore, if the tooth dies, abscesses, or becomes in any way painful after treatment and the patient didn't realize they had about a 20% chance of that happening with such a heavy preparation of the tooth, he/she is likely to become disillusioned, angry or litigious, or all of these.5
Recession around crown margins is a frequent long-term outcome of subgingival placement of crown margins, especially in patients with a thin periodontal biotype. Patients should be made aware of the probability of this long-term negative aesthetic outcome.
Justifying the need for ‘cosmetic’ dental intervention
The more elective the procedure, the wider the safety margin needs to be. For instance, if a patient presents with a very carious tooth where the caries is now very close to pulp, the reasons for treatment are usually obvious, both to the patient and to the dentist. The need for treatment of such a problem is equally obvious to other dentists and probably defensible under most circumstances. If the tooth dies as a consequence of the radiographically provable carious process and/or treatment and, if subsequently, the tooth needs root-filling or possibly extraction, then that outcome would probably be accepted, by most reasonable dentists and by most patients' lawyers, as a known, if unfortunate, outcome. One would hope that it wouldn't happen. It doesn't happen in all cases, but it does happen in some cases. In such cases, it could be argued that the patient presented with a readily recognizable disease and that a representative, responsible, body of dental opinion, in practice at that time, would have agreed with the diagnosis and would have carried out similar treatment. In other words, it would pass a ‘Bolam’ test. It would probably also pass a ‘Bolitho’ test which requires that the opinion and the associated treatment withstands ‘logical scrutiny’.
In some cases, the death of teeth occurs as a result of an identifiable pathologic disease such as caries. Caries is a slow process which produces various changes in the pulp. When the pulp detects the products of the invading bacteria, probably as part of an evolutionary protective mechanism, the pulpal/dentinal complex sends the invading bacteria off on a wild goose chase around the amelodentinal junction, thereby leaving the pulp enough time to recede and lay down secondary, or reparative, dentine.
Many dentists, when providing elective aesthetic dentistry, do not seem to realize fully that an unprovoked attack with an air rotor, on a tooth that was previously virtually intact, involves an entirely different scenario. An elective air rotor strike on a tooth that was previously relatively sound involves the underlying healthy pulpal-dentinal complex getting no time or real chance to defend itself.
When the attack happens, millions of dentinal tubules are opened up in minutes by these aggressive high-speed diamond bur preparations for these putative ‘cosmetic’ restorations. The odontoblastic tubules inevitably get physically damaged and then contaminated by the subsequent micro-leakage into the vast amounts of dentine which has been freshly opened and often not effectively sealed. Much of the damage is done in the fortnight or so when the teeth are ‘temporized’ while the oxymoronic ‘permanent cosmetic’ restorations are being made.
Sadly, some dentists still provide very poor temporary restorations which do not seal the freshly wounded dentinal tubules. Many teeth die because of the micro-leakage around these temporary restorations, most of which are made of plastic and consequently flex. They usually have poorly sealing temporary material holding them in position for ease of removal in order to speed up the process of delivery of the supposedly ‘permanent’ restorations. Teeth often die because the pulp in the region of the necks of the teeth and the pulp horns is very close indeed to the surface after these elective, destructive preparations. It doesn't require any real dental intelligence to realize that bacterial invasion of the residual small amount of dentine will bring the bacteria into very close proximity with the pulp in a very short time. Manufacturers' claims that are sometimes made that, if the dentine is ‘sealed’ with dentine bonding agents immediately after the preparations, there will be no long-term problems, remain speculative. Such bonding may be helpful, or at least better than nothing, but it is certainly not as foolproof as maintaining the ‘enamel overcoat’ in the first place.
Sometimes, while supposedly ‘permanent’ porcelain veneers are being made, poorly sealing temporary veneer material is tenuously ‘spot retained’, possibly leaving any exposed dentine without adequate protection in the critical areas, such as the cervical regions.
Bearing in mind that these destructive procedures are sometimes undertaken for quite tenuous reasons, this is a very unfortunate biologic scenario and poses serious fundamental ethical questions, such as why it should be provided without very good reasons. For instance, some dentists think of teeth as ‘being part of a group’. It is not unusual for dentists to try to match two centrals by doing a matching restoration, in a matching material, on the adjacent central incisor which has, or had, virtually nothing wrong with it. It is done simply because it is part of the ‘pair of central incisors’. It is not infrequent to see dentists apparently thinking of all the incisors as having to be done in the same material, at the same time, for them to ‘match’ what some dentists perceive to be ‘patient's expectations’. Some enthusiastic dentists extend this ‘philosophy’ to include the canines, and sometimes premolars. Increasingly, it has become popular for some ‘cosmetic’ dentists to provide porcelain veneered restorations extending from the upper left second premolar to the upper right second premolar or, in some extreme cases, from the first molar around to the other first molar.
These porcelain veneers or other ceramic veneered restorations, that are subsequently placed, are often provided for teeth that have committed no other ‘crime’ than they were slightly in the wrong positions, or committed the very dangerous offence of not providing a wide enough ‘buccal corridor’. In order to treat this ‘cosmetic crime’, many of these, otherwise innocent, teeth are reduced to a cloud of dental dust and have restorations of a lavatorial white colour placed on the much reduced residual tooth tissue with the latest resin cement.
It is deeply unfortunate that many dentists misrepresent extensive veneer preparations for porcelain restorations as being biologically innocuous. Nothing could be further from the truth. If patients are not told very clearly and in writing that there are long-term biologic consequences involved in the provision of such restorations, they will have every right to seek redress, either financial or legal, from the dentist who provided such an ‘ear to ear mutilectomy’ (Figure 12). Many ‘new’ or ‘newly fashionable’ ceramic restorations still require vast amounts of sound tissue to be removed in order to use them and some of these materials have little sound clinical long-term evidence for their use (Figure 17). Much of the ‘evidence’ is from short-term, biased, often sponsored, or otherwise tainted, ‘research’ of the materials involved.5
Figure 12. Preparations for zirconia/ceramic crowns ‘AN EAR TO EAR MUTILECTOMY’ NOTE THE STRUCTURAL DESTRUCTION TO THE UPPER TEETH. Pulpal health following this? Was there informed consent for this elective destruction? What is this very strange dental disease that only affects top teeth? Was the damage done by some ‘northern hemisphere only’ lactobacilli or colonies of Streptococcus mutans that do not attack lower (‘southern hemisphere’) teeth? Ethical issues in marketing this approach?Figure 13. Preparations for most of the ‘new ceramic’ full crown systems still require massive amounts of sound tooth destruction. (These were repreparations following fracture of the previous porcelain jacket crowns placed in 1976).Figure 14. Ethical marketing? Do patients get shown this on dentists’ websites before agreeing to have the ‘NEW’ ceramic full crowns? Are they told about the probable requirements for remakes later on in their lifetime? Would they agree to have this treatment if they really knew and understood? Acceptable treatment in the 1970s but not now?5Figure 15. Do potential patients just get shown this sort of picture instead rather than a mix of Figures 13, 14, 15, 16.Figure 16. It is unethical in marketing ‘cosmetic’ dentistry to imply that losing two thirds of the sound tooth tissue for ceramic crowns is irrelevant (Edelhoff and Sorenson 20027).Figure 17. Shows a newish material – Procera which was used to crown some ERODED front teeth. Two years later four pulps were dead and a lot of the porcelain had chipped off in return for 62–73% of the structure of the remainder of the eroded teeth. The patient is now biologically and financially much worse off. Is it ethical to promote this as just ‘cosmetic’ dentistry?
The arguments for a less destructive approach in solving aesthetic problems
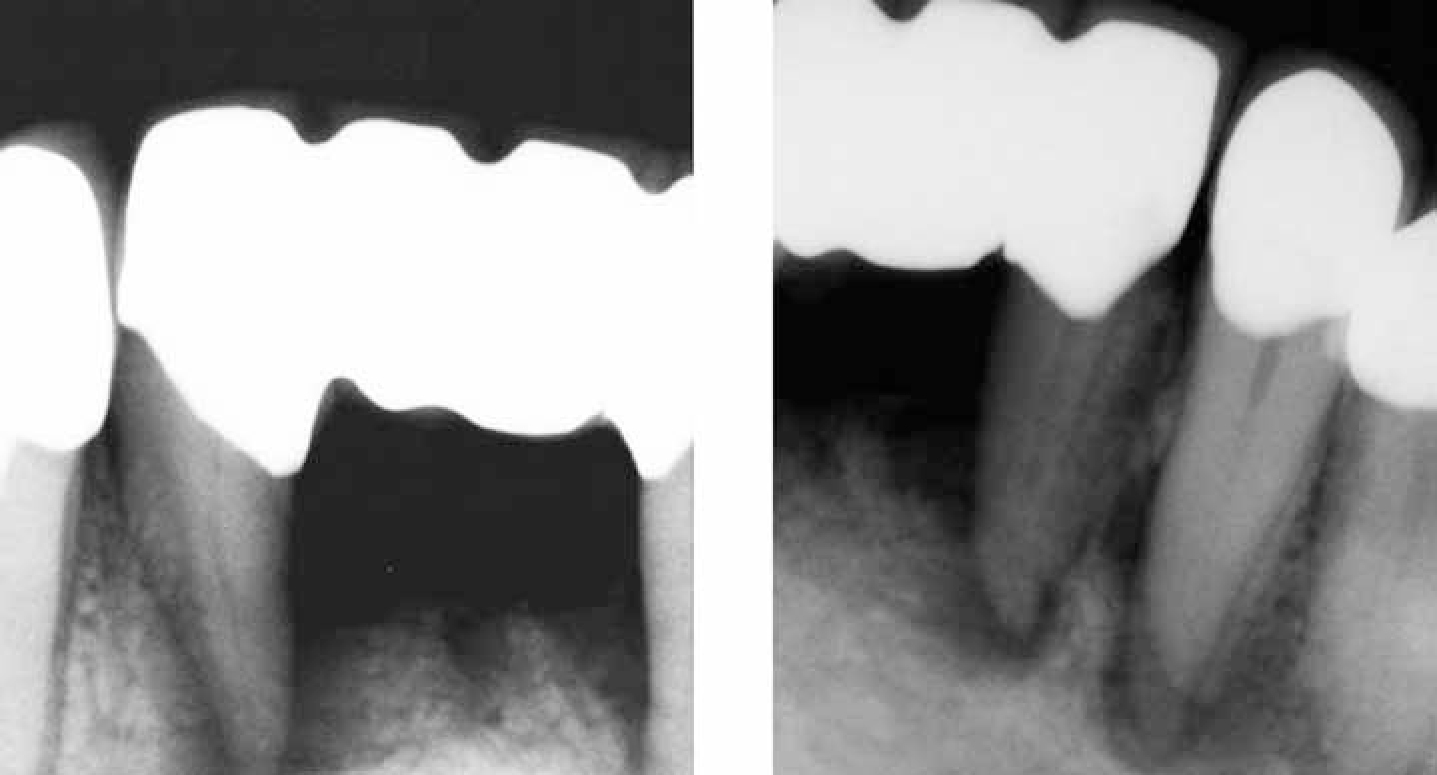
Contrast the extreme make-over scenario shown in Figures 18–22, if you will, with the alternative sensible approach of using low concentration (10% carbamide peroxide) nightguard vital bleaching with the subsequent provision of acid-etched, retained, directly-bonded, composite resin restorations shown in Figures 26–30. Directly-bonded composite applied to the outside of problematic teeth can change the shape of these teeth quite dramatically but structurally the strength of the tooth is not impaired in any way. Preparation for a porcelain veneer would involve the loss of somewhere between 3% and 30% of the structure of the tooth, while application of composite to the outside of unbleached or bleached enamel will not damage the strength or structure of the underlying tooth structure in any way. The pulp will remain unaffected as the ‘enamel overcoat’ is still present.
Figure 18. Patient cured of a serious case of ‘porcelain deficiency disease’ at huge biologic cost and financial benefit, short term, to the dentist.Figure 19. Periapical radiographs of the dead teeth because they were prepared 2 years previously as part of ‘a makeover’ shown in Figure 18.Figure 20. A section of the OPT radiograph showing endodontic and periapical status of the ‘prepared’ teeth as well as evidence of an apicectomy at LR4 which resulted in mental nerve dysaesthesia.Figures 21. Radiographs showing the endodontic treatment being undertaken, probably as a direct result of a ‘cosmetic’ dentistry makeover. Did the patient realize this might happen when they ‘gave their (supposedly) ‘ informed consent’ for this elective ‘cosmetic’ treatment? (Endodontic treatment courtesy of Mr Tony Hoskinson.)Figures 22. Radiographs showing the endodontic treatment being undertaken, probably as a direct result of a ‘cosmetic’ dentistry makeover. Did the patient realize this might happen when they ‘gave their (supposedly) ‘ informed consent’ for this elective ‘cosmetic’ treatment? (Endodontic treatment courtesy of Mr Tony Hoskinson.)Figure 23. Prior to orthodontics. Peg-shaped UR2. Hypoplastic UL1, retained deciduous canines, impacted canines, fluorosis.Figure 24. Impacted upper permanent canines and UL5.Figure 25. The canines and upper left second premolars aligned in the arch by fixed orthodontic therapy.Figure 26. Unstable peg-shaped lateral, surrounded by M-shaped dark space and dark canine.Figure 27. Phosphoric acid gel just over the hypoplastic part of UL1.Figures 28. Bleaching of the canines preferentially was followed by bonding to UR2 and UL1, UL2, UL3 one week later.Figures 29. Bleaching of the canines preferentially was followed by bonding to UR2 and UL1, UL2, UL3 one week later.Figure 30. Ethical marketing? Bleaching and bonding (B&B) provides an aesthetic improvement with preservation of sound tooth tissue. It also stabilizes the post orthodontic position of the peg-shaped upper right lateral incisor.
Composite bonding should be delayed for at least a week after the cessation of bleaching in order for the colour of the newly bleached teeth to stabilize and also for any residual oxygen left in the tooth from the bleaching not to interfere with the composite bond strength. In this possible treatment scenario it needs to be clearly understood by the patient that the composite material is not a ‘once and for a lifetime’ restoration. Patients need to know in advance that the composite can, and probably will, need to be re-polished, resurfaced or replaced, at whatever intervals are deemed to be appropriate by the patient. However, the biological benefit of this approach is that this can be done without expecting any long-term pulpal or structural damage to the composite bonded teeth themselves. That said, in terms of ethical marketing, the very real limitations of the material, including its high free surface energy, have to be clearly understood by the patient (Figures 3–7 and 26–30).
Staining or chipping are occasional complications of direct composite resin, especially if the material is in thin section, and the teeth may well appear to be ‘less shiny’ than enamel or porcelain. In the ‘ethical marketing’ of such a ‘conservative’ approach, an appropriate fee structure needs to be agreed, in advance, with the patient for the polishing, repairs and any renewals of the bonded composite for whatever the agreed period involved is in this approach to solving his/her aesthetic problem. The patient needs to understand his/her responsibility for the problems in advance of this style of ‘minimally destructive’ treatment being undertaken. In that way patients know what they are getting into, including the need for maintenance at their own expense. However, when undertaking this style of minimally destructive dentistry, it is often sensible practice to include a reasonable fee early on in the initial financial negotiations for the expected cost of such polishing/minor repairs for an agreed number of years. Most patients are happy enough with this approach, particularly when it is pointed out to them that it is the composite material that is partially failing but that composite can be ‘recycled’, repaired or ‘repointed’ as required in the future. This is in stark contrast to their own precious enamel and dentine which cannot be renewed as sound tooth tissue is a finite and non-renewable source.
This detailed discussion in relation to the dentist's and the patient's obligations for polishing, repairs and renewals needs to be undertaken well in advance of the provision of any such bleaching and bonding. However, this approach presents less of an ethical dilemma provided the patient is clearly informed of the limitations of the material and is equally informed of its relative benefits of safety for the pulps and preservation of the strength of his/her underlying tooth or teeth. It is all a matter of balance in providing all the relevant information in a neutral, unbiased way in order for the individual patient to be in a position to exercise his/her autonomy (Figures 3–7).
Autonomy, in simple terms, means that patients have a right to have treatment done to their bodies that they wish to have done, provided they are in full possession of all the relevant facts and accept the good and bad consequences of their decisions. For instance, many young people have lived to regret having had the name of their current lover tattooed on some part of their anatomy. When that relationship ceases, they often want the tattoo removed or undone. Some, curiously, think that the state should, somehow, be responsible for the removal of the tattoo because of the visually embarrassing evidence of their former lover, possibly interfering with their ‘new’ love life.
In dentistry, if fashions should change and, at some point in the future, some patients, who previously regarded their teeth as a sort of fashion accessory and had very even ‘lavatorial white’ teeth, then decide that they want more natural looking teeth with more irregularity or more evidence of a ‘natural look’, it is extraordinarily difficult, not to mention biologically quite dangerous, to change extended veneers or full coverage restorations. Such changes may involve large amounts of previously provided porcelain veneers or all-ceramic or zirconia-based crowns, or Procera crowns being drilled off in order to change the appearance once again. This is a very tedious and arduous task that most dentists, or their patients, rarely enjoy very much (Figures 17 and 18).
If the dentist had been unwise enough to describe in any correspondence to the patient, in advertising, eg in practice leaflets or on their website, or in any other way to give the impression that the patient was being supplied with ‘permanent veneers’ or ‘permanent crowns’ and there are subsequent problems of gingival recession, cracks, chips or wear, then the restorations clearly lack ‘permanency’. Permanent is an absolute term like ‘virginity’ or ‘sterility’. One cannot be ‘a bit of a virgin’ or things cannot be ‘a bit sterile’. It is or it isn't. Lawyers, in particular, are good with the real meaning of words and they know what the word ‘permanent’ really means. To them at least, a porcelain veneer is not ‘permanent’ when, in some studies, about half of the porcelain veneers placed are either deficient, have had some sort of repair, or are no longer present at all at 10 years.10
Helpful hints on managing patients requesting ‘Cosmetic Improvement’
In discussing aesthetic problems with patients it is often useful to ask patients whether they are into:
‘Self-preservation’ (ie keeping what sound tooth tissue the patient has got for his/her longer term requirements); or
‘Self-improvement’ (ie doing something to the teeth that would, hopefully, improve their appearance; or
‘Self-destruction’ (ie having destructive procedures done to the teeth, mainly being undertaken to provide an improvement in the appearance of the smile and face).
Sadly, patients are often not asked to think about any such ‘self categorization’.
Most sane patients with a dental aesthetic problem want variable amounts of ‘self-improvement,’ preferably with lots of ‘self-preservation’. Often, they have not had anyone point out the ‘self-destructive’ aspects of crowns or veneers as, in many mindless dental advertorial type publications or celebrity obsessed fashion publications, these essentially balancing negative aspects get blissfully (or conveniently) forgotten, possibly for financial reasons.5
Visual analogue scales as a method of assessment of patients' views
A series of simple visual analogue scales can be useful to help to evaluate patients' views on these conflicting aspects of ‘cosmetic’ dentistry in their own unique value system.
Please ask the patient to place an ‘X’ along each of the scales from 0–100 to reflect his/her views on particular priorities in relation to ‘self-preservation’, ‘self-improvement’ or ‘self-destruction’.
Self-preservation
How important is ‘self-preservation’ (keeping your own teeth strong and healthy) to you?
1…………………………………………100 Not important Important Very Important
Self-improvement
How important is ‘self-improvement’ (making the teeth look better) to you?
1…………………………………………100 Not important Important Very important
Self-destruction
How important is it to you to avoid damaging your teeth in the long term?
1…………………………………………100 Not important Important Very Important
What worries you most about your teeth?
Colour
1…………………………………………100 Not important Important Very Important
Position
1…………………………………………100 Not important Important Very Important
What are you really after?
………………………………………………
………………………………………………
………………………………………………
………………………………………………
………………………………………………
………………………………………………
………………………………………………
The potential for real conflicts between patient expectations and clinical reality needs to be discussed in detail and preferably agreed in writing prior to agreeing to undertaking any destructive procedures.
There are some patients who still do want the most destructive procedures undertaken in order to try to ensure the ‘greatest possible self-improvement’. In other words, they are so obsessed about their appearance, at that time, that they say that they ‘don't care’ what the consequences of their decision are in having destructive procedures and what this might mean for their currently sound teeth in the longer term. That is their view expressed, at that time, before treatment is undertaken. It often changes, if and when problems occur. Many such ‘airhead’ patients subsequently deny that they understood all the risks properly, or completely, at the time of the initial treatment. The detailed notes of all the discussions in such cases are absolutely critical if the case is to have any chance at all of being defended on consent issues.
Summary
In considering the ethical marketing of aesthetic or cosmetic dentistry the critical questions still remain:
What are the benefits and real risks involved?
What are the real problems with the possible solutions?
What is the motivation for offering this service or treatment?
Is this a fair description of what is really being offered?
Is it reasonable?
Is it sensible?
Is it an honest description of what is really involved in the long term?
Are there viable alternatives?
What would their costs be in terms of teeth, time and, lastly, money?
What are the fallback positions, when and if it goes wrong?
Would I be happy for this treatment to be done to me or one of my own family or good friends?
Would I regard any proposed treatment as the best thing to do if this were my own daughter?11
Figures 23–30 illustrate the use of these critical questions.
If these questions can be answered honestly and fairly, then there is a strong chance that what is being offered is as a result of ethical marketing, ie finding out what someone really wants and tailoring the best plan/solution to satisfy those aspirations while still minimizing biologic problems for the patient in the longer term.