Brånemark PI, Hansson BO, Adell R Osseo-integrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977; 16:1-132
White DA, Tsakos G, Pitts NB Adult Dental Health Survey 2009: common oral health conditions and their impact on the population. Br Dent J. 2012; 213:567-72 https://doi.org/10.1038/sj.bdj.2012.1088
Bragger U, Heitz-Mayfield LJA. ITI Treatment Guide Volume 8. Biological and Hardware Complications in Implant Dentistry.Berlin: Quintessence; 2015
Schulte W. Implants and the periodontium. Int Dent J. 1995; 45:16-26
Kazemi M, Geramipanah F, Negahdari R, Rakhshan V. Active tactile sensibility of single-tooth implants versus natural dentition: a split-mouth double-blind randomized clinical trial. Clin Implant Dent Relat Res. 2014; 16:947-955 https://doi.org/10.1111/cid.12053
Luo Q, Ding Q, Zhang L, Xie Q. Analyzing the occlusion variation of single posterior implant-supported fixed prostheses by using the T-scan system: a prospective 3-year follow-up study. J Prosthet Dent. 2020; 123:79-84 https://doi.org/10.1016/j.prosdent.2018.12.012
Madani AS, Nakhaei M, Alami M Post-insertion posterior single-implant occlusion changes at different intervals: a T-scan computerized occlusal analysis. J Contemp Dent Pract. 2017; 18:927-932 https://doi.org/10.5005/jp-journals-10024-2151
Stoichkov B, Kirov D. Analysis of the causes of dental implant fracture: a retrospective clinical study. Quintessence Int. 2018; 49:279-286 https://doi.org/10.3290/j.qi.a39846
Urdaneta RA, Rodriguez S, McNeil DC The effect of increased crown-to-implant ratio on single-tooth locking-taper implants. Int J Oral Maxillofac Implants. 2010; 25:729-743
Montero J, Manzano G, Beltrán D Clinical evaluation of the incidence of prosthetic complications in implant crowns constructed with UCLA castable abutments. A cohort follow-up study. J Dent. 2012; 40:1081-1089 https://doi.org/10.1016/j.jdent.2012.09.001
Sheridan RA, Decker AM, Plonka AB, Wang HL. The role of occlusion in implant therapy: a comprehensive updated review. Implant Dent. 2016; 25:829-838 https://doi.org/10.1097/ID.0000000000000488
Graves CV, Harrel SK, Rossmann JA The role of occlusion in the dental implant and peri-implant condition: a review. Open Dent J. 2016; 10:594-601 https://doi.org/10.2174/1874210601610010594
Lee JH, Kweon HH, Choi SH, Kim YT. Association between dental implants in the posterior region and traumatic occlusion in the adjacent premolars: a long-term follow-up clinical and radiographic analysis. J Periodontal Implant Sci. 2016; 46:396-404 https://doi.org/10.5051/jpis.2016.46.6.396
Gibbard LL, Zarb G. A 5-year prospective study of implant-supported single-tooth replacements. J Can Dent Assoc. 2002; 68:110-116
Di Stefano DA, Arosio P, Pagnutti S Distribution of trabecular bone density in the maxilla and mandible. Implant Dent. 2019; 28:340-348 https://doi.org/10.1097/ID.0000000000000893
He J, Zhao B, Deng C Assessment of implant cumulative survival rates in sites with different bone density and related prognostic factors: an 8-year retrospective study of 2,684 implants. Int J Oral Maxillofac Implants. 2015; 30:360-371 https://doi.org/10.11607/jomi.3580
Nagpal S, Kamath S, Thakur S, Kulkarni S. Correlation between occlusal forces and marginal bone levels around implant-retained restorations: a clinico-radiological study. J Oral Implantol. 2012; 38:261-269 https://doi.org/10.1563/AAID-JOI-D-10-00024
Misch CE, Bidez MW. Implant-protected occlusion: a biomechanical rationale. Compendium. 1994; 15:1330-1334
Byrne G. Implant biomechanics.Iowa, USA: Wiley-Blackwell; 2014
With the rise in popularity of dental implants to replace missing teeth, there are also increasing concerns surrounding complications. Within the plethora of complications and associated aetiologies, occlusion is possibly the least understood. The biomechanical principles shown in this article can provide some suggestions on occlusal schemes for single implants.
CPD/Clinical Relevance: By understanding occlusal considerations for single implant crowns, the risk of complications can be minimized.
Article
Dental implants have been used to replace missing teeth for over 30 years since research conducted by Brånemark allowed understanding of the concept of osseo-integration1, which described the relationship of the living bone to a functional implant. According to the Association of Dental Implantology an estimated 130,000 implants were placed in 2012 in the UK.2 With many more adults retaining the majority of their teeth into their later years,3 it is likely that more people will opt to have single-tooth gaps restored, with implants being a desirable option compared with traditional fixed bridges. With the rise in popularity of implant therapy, there has been increasing research into the diagnosis and management of complications associated with implant borne restorations. The ITI (International Team for Implantology) has a multitude of consensus statements regarding a variety of reasons for such complications,4 occlusion being one of them. Within the ITI Treatment guide Volume 8, occlusal overloading has been attributed to various biological and hardware complications, such as porcelain chipping, screw loosening, potential adverse effects on crestal bone levels, and even possible loss of osseo-integration.4
Why implants are different
Occlusal schemes are likely to vary between an implant and natural tooth due to the lack of periodontal ligament. The ‘functional ankylosis’ term was coined to accurately describe the relationship of bone to implant. Connective tissue attachment occurs only on the supracrestal element of the implant, whereas the entire periodontal ligament (PDL) in a tooth provides connective tissue attachment along the entire root length. The lack of a PDL leads to a reduction in the adaptive capacity of an implant. The PDL will allow a small degree of movement and contains proprioceptors and mechanoreceptors that provide important feedback during function to avoid overload.5 Shulte described these differences in 1995, and showed the axial movement in an implant is approximately 5 mm compared with 25–100 mm for a tooth. Not only would this lead to an implant restoration being unable to manage an occlusal discrepancy, such as the restoration being in supra-occlusion, as easily as a natural tooth, but it would prevent any possibility of orthodontic movement due to occlusal discrepancies. The tactile sensitivity of an implant has also been shown to be less than that of even a root-filled tooth that has lost some proprioception within the pulp.6
Changes to implant occlusion over time
Studies have been carried out to assess the occlusion of patients with implant-borne crowns over time.7,8 Over time, there was a significant increase in the relative occlusal force on implants. Interestingly, the occlusal forces around a natural tooth remain consistent over time. These studies suggest that this change in occlusion over time is due to the opposing dentition continuing to erupt to occlude with the implant crown in a similar manner to that with a natural tooth.
It is known that the minimum axial movement afforded by the PDL is approximately 25 mm.5 This can then be used as a basis of considering how ‘light’ the occlusion needs to be on an implant crown. When attempting to adjust the occlusion to within microns, a clinician's ability to accurately use the appropriate articulating foil will help greatly with assessing and adjusting the occlusion. If this concept is extrapolated further, then as the occlusion develops over time, it may indicate that further restorative treatment will be needed in the future to correct the altered occlusion. This highlights a need for potential long-term data in this area to help to assess how clinically relevant the redistribution of forces is, and how likely it is for occlusal overloading to occur.
Correlation of occlusal forces to prosthetic complications
As mentioned earlier, a variety of prosthetic complications can be linked to occlusal forces, the most severe of which being fracture of the implant itself. The common factors associated with the complications with single-implant crowns in particular are parafunction and a lack of ‘implant-protected occlusion’.9 This concept of implant-protected occlusion is discussed later in the article.
A more commonly found complication is loosening of the abutment screw. Fortunately, this is a relatively easily managed complication that simply requires tightening of the screw. However, the potential cause of this relatively minor issue should not be ignored. Cohort studies10,11 have, in particular, linked the dimensions of the implant crown to an increased incidence of screw loosening. The crown to implant ratio, as well as the mesio-distal width of the crown, have an impact on screw loosening, particularly with long-crown crowns (such as in anterior restorations, where significant vertical bone loss has occurred) or single implants replacing large edentulous spaces.
Consideration should also be given to what the restoration will be occluding against. The adaptive capability of the opposing structure should be factored in when setting the occlusal scheme. For example, a restoration opposing another implant will require a slightly different occlusal scheme to one opposing a natural tooth.
Effects of occlusal forces on peri-implant bone levels
The lack of a PDL around an implant results in reduced axial and buccolingual movement.5,12 Within a natural tooth, the PDL allows for some adaptation to loading prior to that force being transferred to the alveolar bone. The forces applied to an implant are applied to the bone with little capacity for shock absorption as is afforded by the PDL.
Cortical bone is significantly stronger under compressive forces rather than shear forces.13,14 These compressive forces can be applied with occlusal forces directed along the long axis of the implant. Non-axial loading, such as during excursive movements, interferences or premature contacts will lead to an increase in stress and shear forces around the crestal bone, which can result in crestal bone loss.15 From a biomechanical perspective, it would be reasonable to add that consideration therefore needs to be given to the surgical placement of the implant itself. If an implant is placed at an angle, then what may be perceived as axial loading on the prosthesis is in fact non-axial loading on the implant itself, which will result in increased shear forces on the crestal bone. This review does not cover this area of inquiry; however, it is obvious that reasons for complications are wide ranging and multifactorial,4 thus it would be pertinent to have a well-rounded understanding to minimize such complications.
The direction of the occlusal forces is a common issue that is raised within the literature with many ‘ideal’ schemes avoiding lateral or non-axial loading where possible. Many of the prosthetic complications found by Urdaneta et al were associated with the anterior maxillary teeth where they are naturally angled and therefore loaded non-axially.10 Work by Gibbard and Zarb found that more marginal bone loss was observed in implants involved in excursions.15 It may be possible that the position of maxillary anterior implants predisposes them to possible complications in addition to the potential for force distribution to be disadvantageous in larger crown to implant ratios. The maxilla often has a lower bone density than the mandible,16 and a reduced bone density has been linked to lower long-term implant survival rates.17
It is noted within the literature18 that in implants involved in excursions and heavy occlusal contacts, outcomes were still favourable if the there was no overall occlusal derangement, such as interferences, premature contacts and underlying parafunction.
Implant-protected occlusion
The biomechanical principles mentioned earlier underpin the concept of ‘implant-protected occlusion’, a term coined by Misch19 in 1994, whereby the aim is to reduce forces at the junction of the crestal bone and implant. Much of the literature refers to this principle and it is referred to as the occlusal scheme of choice. Stress analysis studies have underpinned these biomechanical principles on which occlusal schemes are based. With respect to the occlusal scheme, the idea of implant-protected occlusion involves light centric contacts to allow for the natural teeth to displace axially in a heavy bite. If the implant contact is heavy, the majority of the occlusal force will be placed through the implant with almost no ability for it to displace axially. The implant should ideally not be involved in lateral or protrusive guidance to minimize non-axial loading, because the implant discludes during any excursive or protrusive movements. Consideration should be given to implant positioning, length and width, further adding that the occlusal table should be kept narrow.
Conclusion
Study designs are extremely limited when assessing occlusal overload in implants owing to the ethical issues involved, thus high-quality data from robust clinical trials are scarce. Further research is paramount in this field because of the ever-increasing popularity of implant dentistry among patients and clinicians alike. There needs to be a higher quality of evidence, such as through clinical randomized controlled trials, ideally, to consider specific effects of occlusal overload that can help to formulate a more definitive set of guidance surrounding implant dentistry. Once these data are obtained, their clinical relevance must be determined. For example, some studies found a difference of less than 1 mm of bone loss. Clinically, it would be difficult for the average clinician to distinguish such a small change, which could make the research clinically irrelevant. In addition, the multifactorial nature of implant dentistry can make it difficult to ascertain exactly what can cause a particular complication, especially in the long term. Using the existing evidence, it is clear that a good understanding of the biomechanical principles affecting both natural teeth and implants, and the differences between them, is needed when prescribing the most appropriate occlusal scheme during treatment planning. Despite the lack of clarity as to exactly how occlusion will affect clinically significant complications, it makes sense to avoid heavy excursive contacts on single-implant crowns to avoid a myriad of biological and prosthetic complications.20 Consequently, it may be useful for the clinician to assign a level of risk with respect to occlusal overload. While commenting on the dimensions and position of the implant itself are outside the scope of this review, it would be wise to carry out further study into the role these elements have in occlusal management. Some general recommendations for single implant crown occlusal scheme can be made:
Avoid implant treatment on patients with parafunction
Consider an occlusal splint in these patients.
Mutually protected occlusion
Canine guidance for lateral excursions and anterior guidance for protrusion;
Posterior disclusion during excursive movements;
For anterior implants, guidance should be moved to natural teeth where possible.
No premature, guiding or interfering contacts on the implant crown
Reduce cusp inclines, crown/implant ratio;
Narrow the occlusal table.
Very light contacts in intercuspal position on the implant crown
Tight shimstock holds on natural teeth;
Loose or no shimstock hold on implant crown (ie implant crown is free of occlusion by at least 8 mm).
Consider the use of provisional restorations to finalize the occlusal scheme
Evenly distributed contacts around the whole mouth
Regular assessment of a patients occlusion
Adjustments should be made where required
Shorter recall intervals may be required depending on the risk of occlusal overload.
For any clinician to implement these considerations, it is important that they have a thorough understanding of general occlusal principles also, in particular, the initial occlusal analysis.21 While there is no agreed upon, definitive, evidence-based occlusal scheme for implant restorations, it is important careful consideration is given to the assessment and treatment planning is restoratively driven. Without this, an inappropriate treatment plan will be more likely to result in complications.
Clinical case
Figures 1–6 illustrate the points made previously.
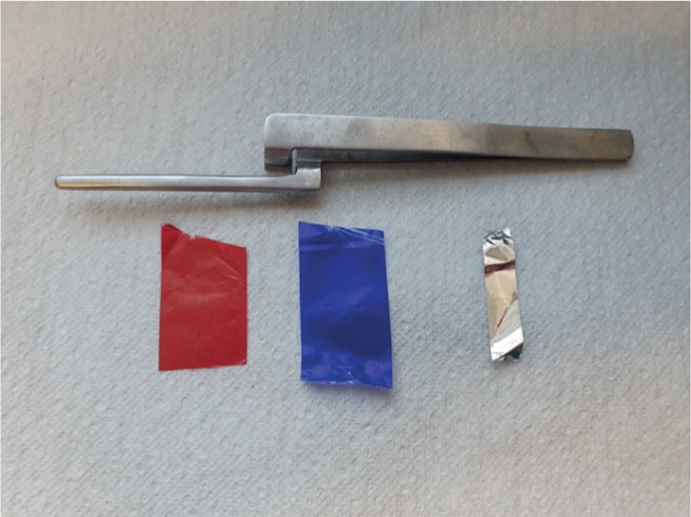
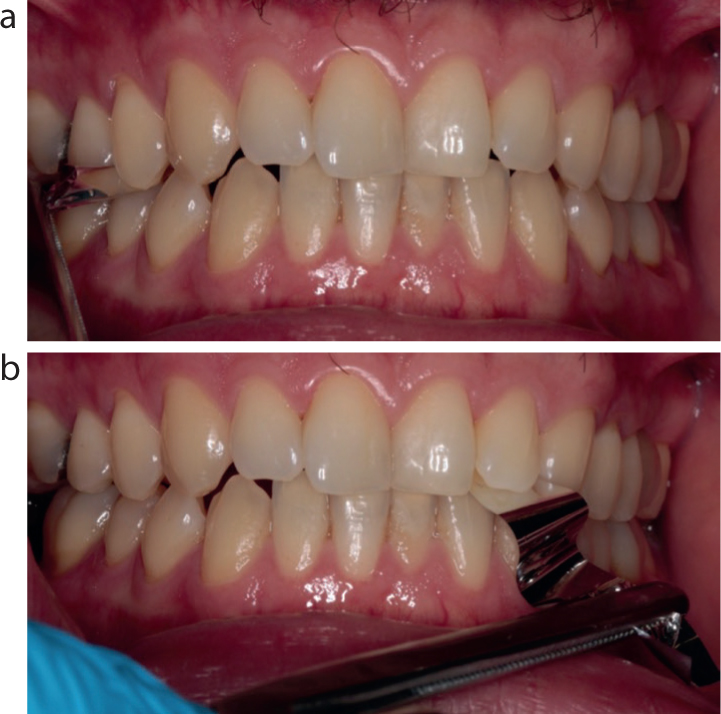
Figure 1. Replacement of UL6. Pre-operative occlusal assessment shows group function in lateral excursions.Figure 2. Use of red and blue articulating foils (12 µm) can help to mark static and dynamic contacts. Shimstock foil (8 µm) can be used to identify strength of occlusal contacts. Miller's forceps can be used to hold the foil to gain adequate tactile feedback.Figure 3. Red GHM articulating foil used to mark occlusal contacts. There was a slight high spot buccally, which was adjusted.Figure 4.
(a, b) No change to shimstock holds on natural teeth.Figure 5. No change to guidance with the implant restoration at UL6 not taking on any guiding contacts.Figure 6. Single shimstock sheet does not hold on implant crown at UL6 doubled up to hold firmly (16 µm) to allow for PDL movement of opposing tooth.