Kobler P, Borcic J, Filipvic Zore I Case report: primary non-Hodgkin's lymphoma of the oral cavity. Oral Oncol Extra. 2005; 41:12-14 https://doi.org/10.1016/j.ooe.2004.10.002
Walter C, Ziebart T, Sagheb K Malignant lymphomas in the head and neck region – a retrospective, single-center study over 41 years. Int J Med Sci. 2015; 12:141-145 https://doi.org/10.7150/ijms.10483
Storck K, Brandstetter M, Keller U, Knopf A. Clinical presentation and characteristics of lymphoma in the head and neck region. Head Face Med. 2019; 15 https://doi.org/10.1186/s13005-018-0186-0
Caponetti G, Bagg A. Demystifying the diagnosis and classification of lymphoma: a hematologist/oncologist's guide to the hematopathologist's galaxy. J Community Supportive Oncol. 2005; 15:43-48
Quintanilla-Martinez L. The 2016 updated WHO classification of lymphoid neoplasias. Hematol Oncol. 2017; 35:37-45 https://doi.org/10.1002/hon.2399
Swerdlow SH, Campo E, Pileri SA The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016; 127:2375-2390 https://doi.org/10.1182/blood-2016-01-643569
Epstein JB, Epstein JD, Le ND, Gorsky M. Characteristics of oral and paraoral malignant lymphoma: a population-based review of 361 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:519-525 https://doi.org/10.1067/moe.2001.116062
Hassona Y, Almuhaisen G, Almansour A, Scully C. Lymphoma presenting as a toothache: a wolf in sheep's clothing. BMJ Case Rep. 2017; 2017 https://doi.org/10.1136/bcr-2016-218686
van der Waal RI, Huijgens PC, van der Valk P, van der Waal I. Characteristics of 40 primary extranodal non-Hodgkin lymphomas of the oral cavity in perspective of the new WHO classification and the International Prognostic Index. Int J Oral Maxillofac Surg. 2005; 34:391-395 https://doi.org/10.1016/j.ijom.2004.08.009
Kemp S, Gallagher G, Kabani S Oral non-Hodgkin's lymphoma: review of the literature and World Health Organization classification with reference to 40 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:194-201 https://doi.org/10.1016/j.tripleo.2007.02.019
Shetty D, Shenai P, Chatra L Numb chin syndrome: a subtle clinical condition with varied etiology. Gulhane Med J. 2015; 57:324-327 https://doi.org/10.5455/GULHANE.44276
Galán Gil S, Peñarrocha Diago M, Peñarrocha Diago M. Malignant mental nerve neuropathy: systematic review. Med Oral Patol Oral Cir Bucal. 2008; 13:616-621
Eisenbud L, Sciubba J, Mir R, Sachs SA. Oral presentations in non-Hodgkin's lymphoma: a review of thirty-one cases. Part II. Fourteen cases arising in bone. Oral Surg Oral Med Oral Pathol. 1984; 57:272-80 https://doi.org/10.1016/0030-4220(84)90183-x
Poulopoulos A, Papadopoulos P, Andreadis D. Chemotherapy: oral side effects and dental interventions – a review of the literature. Stomatol Dis Sci. 2017; 1:35-49 https://doi.org/10.20517/2573-0002.2017.03
Lalla RV, Sonis ST, Peterson DE. Management of oral mucositis in patients who have cancer. Dent Clin North Am. 2008; 52:61-77 https://doi.org/10.1016/j.cden.2007.10.002
Giudice A, Liborio F, Averta F Oral lichenoid reaction: an uncommon side effect of rituximab. Case Rep Dent. 2019; 2019 https://doi.org/10.1155/2019/3154856
You TM, Lee KH, Lee SH, Park W. Denosumab-related osteonecrosis of the jaw: a case report and management based on pharmacokinetics. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015; 120:548-553 https://doi.org/10.1016/j.oooo.2015.07.017
Tolentino Ede S, Centurion BS, Ferreira LH Oral adverse effects of head and neck radiotherapy: literature review and suggestion of a clinical oral care guideline for irradiated patients. J Appl Oral Sci. 2011; 19:448-454 https://doi.org/10.1590/s1678-77572011000500003
Lymphomas in the head and neck region (HNR) can be a diagnostic challenge owing to their indistinctive oral manifestations that frequently mimic other pathologies. This case report highlights a young male who experienced spontaneous paraesthesia of his lower lip with an accompanied localized dull ache. Initial clinical examination and investigations were inconclusive. A definitive diagnosis of extranodal low-grade B-cell non-Hodgkin lymphoma (NHL) was only confirmed after the second incisional biopsy, which was 15 months after onset of symptoms. This report offers insight of NHL in the HNR and its clinical presentation. It aims to improve awareness amongst dental practitioners to aid early diagnosis.
CPD/Clinical Relevance: The reader should consider lymphomas as a differential diagnosis for unexplained symptoms, including paraesthesia, mucosal ulceration and soft tissue swelling.
Article
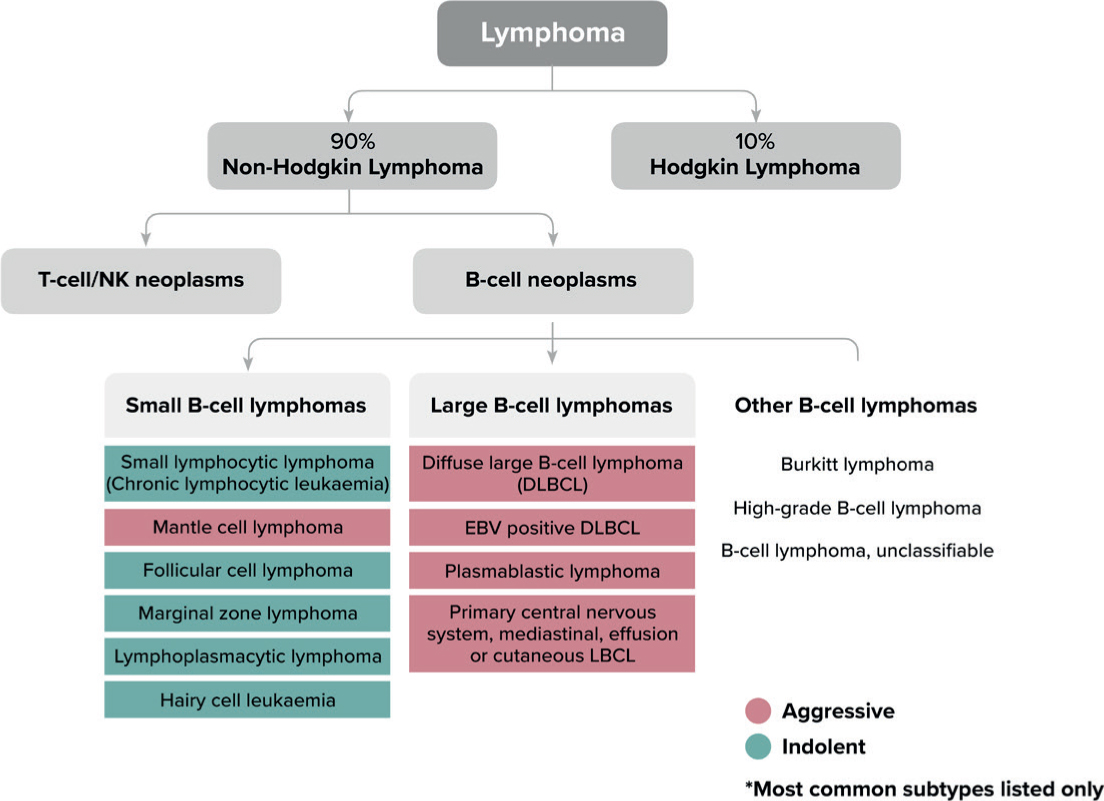
Lymphomas are malignant neoplastic proliferations of the lymphatic system.1 They can be divided into two entities: Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL), depending on the presence or absence of Reed-Sternberg cells, respectively. NHL comprises 90% of all cases, with over 20 different subtypes described in the World Health Organization (WHO) 2016 classification, according to the type of lymphoid cell involved.1,2,34 The majority of NHLs are derived from B-lymphocytes (85–90%), with the remaining arising from T-lymphocytes or natural killer (NK) cells.3 This large group of B-, T- or NK-cell neoplasms can also be subclassified according to their predicted clinical behaviour (Figure 1).5,6,7,8
Figure 1. Lymphoma classification showing subgroups of non-Hodgkin lymphoma.5,6,7,8
Lymphomas are the third most common cancer worldwide, accounting for 3% of all malignant tumours.1,4 They constitute 2.2% of malignancies in the head and neck region (HNR) and are the second most frequent malignancy found in this region, surpassed only by epithelial malignancies.1,9 Although often part of metastatic disease, lymphoma may also present as primary extranodal disease within the oral cavity.10
Lymphomas in the HNR are often difficult to diagnose owing to their non-specific signs and symptoms, which may resemble a number of conditions, including other malignant disease. This case report highlights the complexity in diagnosing lymphoma specific to the oral cavity.
Case report
A healthy 22-year-old male was referred to the oral surgery department at Guy's Dental Hospital by his general dental practitioner (GDP) in April 2019 after developing daily, intermittent, spontaneous numbness and electric shock-type pains on the left side of his lower lip for over 1 month. He was a non-smoker and rarely consumed alcohol. His previous dental history consisted of simple restorative treatment and the extraction of four premolars 9 years earlier for orthodontic treatment.
At assessment, the patient was able to clearly delineate the affected area of altered sensation in the left lower lip extending to the midline, and also reported a localized dull ache in the left anterior mandible. However, there was no history of dental pain, associated swelling or infection. There were no known aggravating or relieving factors, and the dull ache led to disturbed sleep. Prior to his attendance, he had consulted his general medical practitioner (GMP) who prescribed gabapentin 100 mg once daily, which improved the patient's symptoms by reducing the frequency and intensity of the daily episodes.
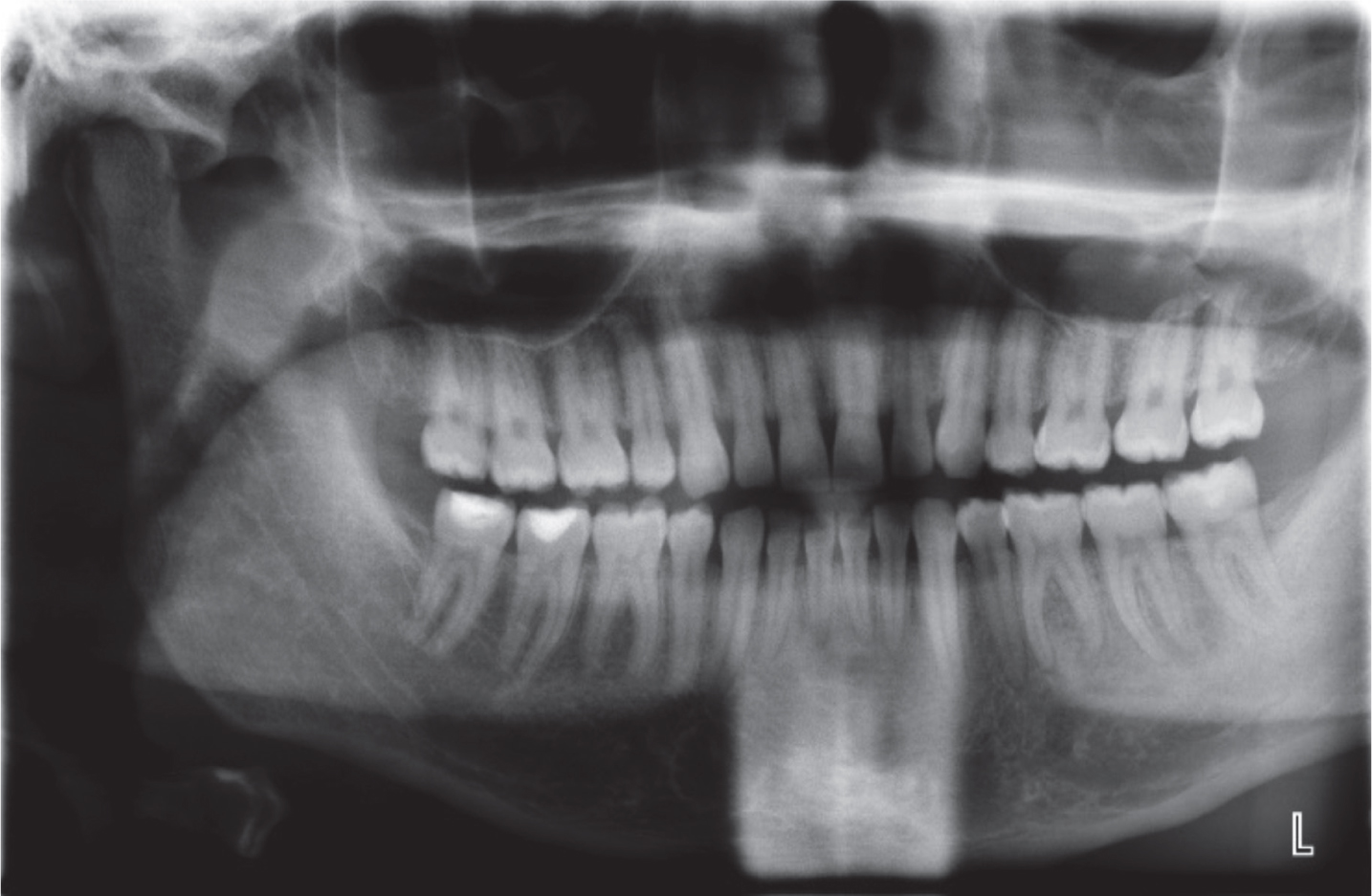
Clinical examination and objective testing of the left inferior dental nerve (IDN) distribution via sharp probing, cotton wool touch and two-point discrimination confirmed altered sensation of the full height of the lower lip to the midline, as well as the buccal gingivae of the lower left canine (LL3) and premolar region (LL5). In addition, there was a mild diffuse fullness of the buccal sulcus of the LL3–LL5, compared with the right side. Specific to the lower left first molar (LL6), there was a firm localized circumferential bucco-lingual enlargement of the alveolus. The enlargement was smooth to palpate with normal overlying mucosa, similar in appearance to bony exostoses. All the teeth in the lower left quadrant were unrestored, with no periodontal pocketing or mobility. Sensibility testing with ethyl chloride gave a delayed response from the LL5. The panoramic radiograph (Figure 2) showed an intact ID canal with no obvious dental or bony pathology. A cone beam CT scan of the mandible and MRI scan of the brain and jaws revealed no clear identifiable cause or pathology affecting the mandibular division of the trigeminal nerve.
Figure 2. Dental panoramic tomograph showing a healthy dentition with no obvious dental or bony pathology.
The uncertainty in diagnosis indicated the need for an incisional biopsy, focusing on the firm swelling in the LL6 region. Interestingly, upon raising a full-thickness mucoperiosteal flap in this region, it became apparent that the firm mass resided within the soft tissues, particularly in the subperiosteum, deep in the sulcus. Dissection through the periosteum to the palpable enlargement allowed a sample of tissue to be obtained for histopathological analysis.
Initial interpretation was suspicious of low-grade B cell non-Hodgkin lymphoma (NHL) and the specimen was sent to the lymphoma team for further analysis and definitive diagnoses. However, following further clonality studies, PET/CT scan and extensive discussions at the lymphoma multidisciplinary meeting, lymphoma was excluded as a diagnosis. The patient's symptoms continued, and he therefore remained on close watchful surveillance.
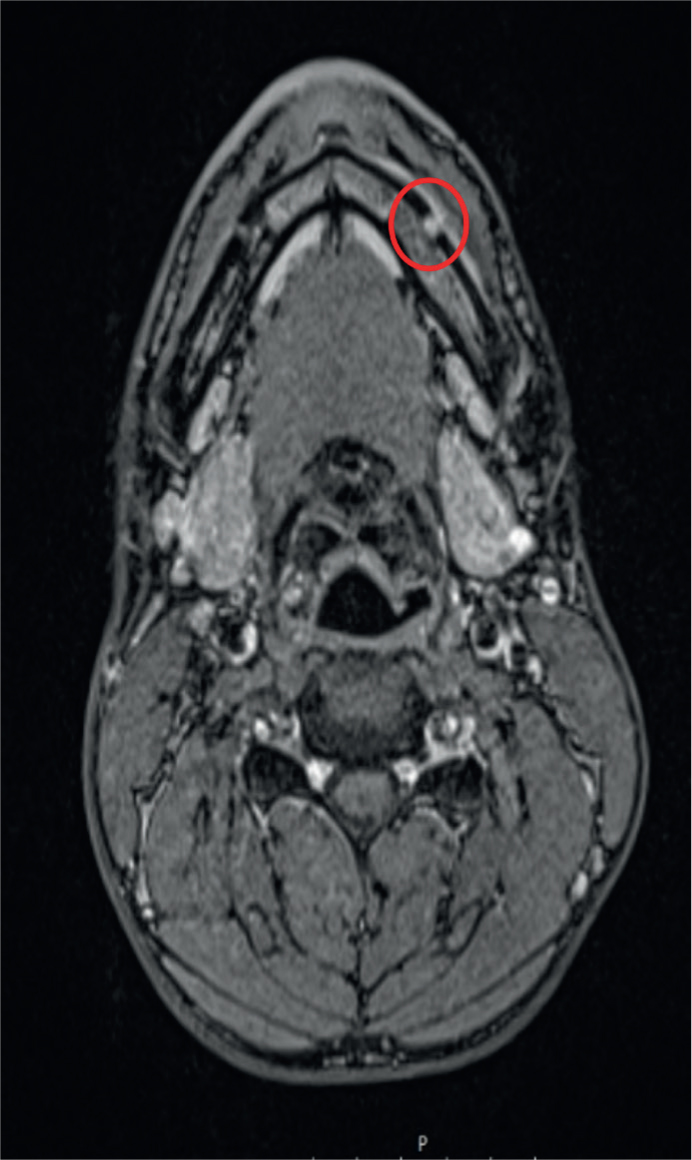
At a subsequent review, 13 months following initial presentation, the patient complained of a new lump, pointing towards the buccal sulcus of the LL3–LL5 region, on the background of continued altered sensation of the left IDN distribution. A new MRI showed abnormal tissue extending through the left mental foramen, 3–4 mm in depth (Figure 3). A further biopsy was performed, and at the time of procedure, a firm soft tissue lesion was evident, encapsulating the mental nerve and extending into the buccal periosteum. Histopathological analysis of the new specimen, including clonality studies, confirmed a marginal zone B cell NHL. No further sites of lymphoma beyond the oral cavity were identified. Owing to the indolent nature of the diagnosis, very low dose (4 Gray) radiation treatment was planned. Due to the unusual nature and presentation of marginal zone B cell NHL, it took 15 months to reach a definitive diagnosis and treatment.
Figure 3. MRI axial view showing abnormality in region of left mental foramen.
Discussion
Lymphoma can arise in any lymph node or organ. It can spread to organs from lymphatic sites or present as a manifestation of primary extranodal disease.11 HL occurs mainly in the lymph nodes (>90%) and often involves lymph nodes of the neck and mediastinum.1,11 In contrast, extranodal HL is uncommon (<5%), whereas the opposite is true for NHL with an estimated 40% of cases presenting extranodally.1,2,3 Extranodal NHL most commonly arises in the gastrointestinal tract, followed by the head and neck region (Waldeyer's ring).1,2,4 Diffuse large B-cell lymphoma is the most common subtype affecting the oral cavity, followed by small lymphocytic lymphoma and Burkitt's lymphoma.1
NHL can occur at any age; however, it typically affects those aged over 50 years, with a higher prevalence in males.1,2 There is also a higher frequency reported in those with acquired or inherited immunodeficiency, including for those with HIV, organ and stem-cell transplantation.1,2,3 The cause of NHL remains unclear, but there is evidence implicating viruses, such as Epstein–Barr virus, as a potential cause.2,3
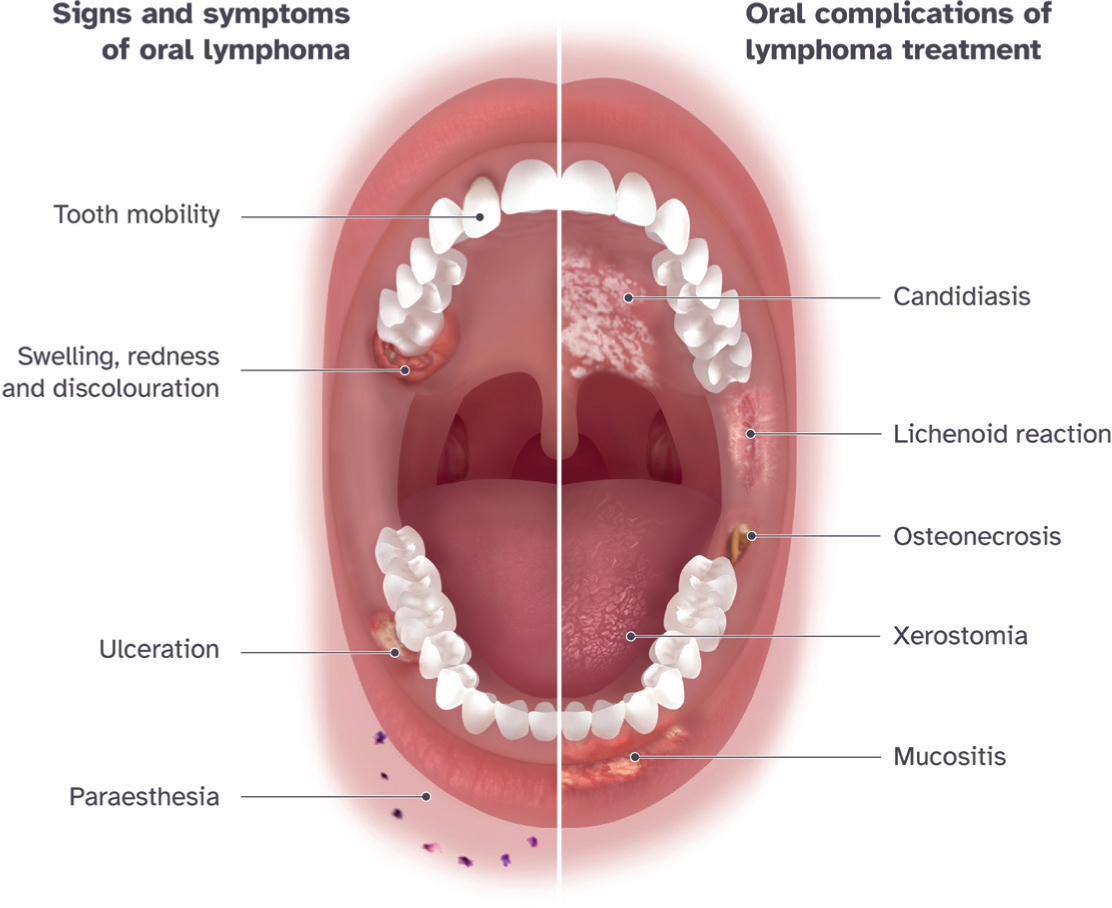
The manifestations of lymphoma in the oral cavity can mimic conditions such as dental abscesses, periodontal disease, osteomyelitis, and other malignancies.1,3 Frequently reported presentations include localized soft tissue swelling, mucosal ulceration or discolouration, paraesthesia, facial asymmetry and mobility of teeth (Figure 4).2,3,12 NHL primarily affects the palate, gingivae and base of tongue.18 In the case presented, the only significant objective symptom was paraesthesia of the lip. Mental nerve neuropathy is often referred to as ‘numb chin syndrome’,18 and a wide range of conditions13,14 can cause these symptoms (Table 1). Galán Gil et al15 reported that 40% of cases presenting as numb chin syndrome are due to cancer metastasis from breast or prostate, with NHL of mandible or skull base accounting for a further 20% of cases. Therefore, in the absence of any intervention, a spontaneous occurrence of paraesthesia should alert a clinician to a high possibility of malignancy until proven otherwise. The presented case is a good example of this, with rapid referral from the GDP.
Figure 4. A split mouth depicting oral signs and symptoms of lymphoma2,3,12 and the oral complications associated with lymphoma treatment.19,20,21,22,23,24
Primary extranodal NHL that originates in the mandible usually arises from bone, whereas those in the maxilla are more likely to arise from soft tissue, and typically originate in the palate.11,16 Those of soft tissue nature may not be clearly evident or palpable, as encountered in this case at initial presentation. As for those originating in bone, various radiographic features may be seen, such as a diffuse pattern of bone destruction, a solitary radiolucent defect or loss of lamina dura of the teeth.11 However, these features can resemble a number of dental or bony pathologies and could, therefore, be overlooked. In such scenarios, the clinician should be vigilant to a differential diagnosis of lymphoma, particularly with non-resolved symptoms following intervention, or clinical and radiographic features that do not align to the initial diagnosis.
The treatment of lymphoma may involve chemotherapy, radiotherapy and biological therapies, such as monoclonal antibodies. Hodgkin lymphoma is often treated with chemotherapy, either alone or in combination with radiotherapy or steroid medication.17 Early stage NHL, where the condition is localized, is often treated with radiotherapy alone. The majority of other NHL are managed with chemotherapy, with or without adjunctive steroid medication or monoclonal antibody therapy.18 Rituximab is the most common monoclonal antibody used to treat NHL, and is also used in the management of lymphocyte-predominant Hodgkin lymphoma, a rare form of Hodgkin lymphoma.
Chemotherapy has several oral complications because of both its direct effect on the oral tissues, and as a result of immunosuppression. Oral mucositis is the most common adverse effect and can arise within a week of commencing a high-dose course. It usually subsides within a month of treatment being completed.19,20 It is a painful inflammatory reaction of the oral mucosa and can present as erythematous or ulcerative lesions. Mucositis significantly affects nutritional intake, mouth care and quality of life.20 Management involves soothing agents, such as saline mouth rinses, crushed ice and topical benzydamine.20
Chemotherapy-induced neutropenia leads to an increased susceptibility to infection.19 To prevent these, a thorough dental examination should be completed prior to chemotherapy and teeth of poor prognosis should be extracted. The most common fungal infections are candidiasis and angular cheilitis, which can be treated with topical or systemic antifungals, such as nystatin or miconazole. Patients are more likely to develop herpetic and varicella-zoster infections, and the extent of the resultant conditions is usually related to the degree of immunosuppression. Antiviral medications, such as acyclovir, are often prescribed. Chemotherapy can also impair salivary gland function; however, this is usually temporary and reversible.
Both chemotherapy and monoclonal antibody therapy, such as rituximab, are associated with lichenoid reactions.19,21 The clinical appearance of lichenoid reactions mimics that of lichen planus; however, they can sometimes regress with removal of the causative agent.19 Features include white reticular striae or papules, homogeneous plaques or erythematous erosions. Where these lesions are symptomatic, and the causative agent cannot be stopped or the condition persists beyond its use, corticosteroids can be used to manage the condition.19
Monoclonal antibodies inhibit angiogenesis and bone turnover by suppressing osteoclast formation. Rituximab, along with several other monoclonal antibodies, can be associated with osteonecrosis, although this is rare.22,23 Medication-related osteonecrosis (MRONJ) can manifest clinically as exposed necrotic bone, pain, orofacial fistulas and pathological fractures.24 These late effects are difficult to manage and can be detrimental to quality of life.
Radiation-induced effects can be separated into early and late effects. Radiation mucositis is an acute reaction, like that experienced with chemotherapy. Another early complication is xerostomia, which arises from radiation damage to the salivary glands, and causes altered salivary composition and decreased salivary flow rate.24 Impaired salivary function can impede oral function, lead to a burning sensation, taste disturbances and increased susceptibility to oral infections and dental caries.25 Moistening agents and saliva substitutes are advised for symptomatic relief and to aid function. A high-fluoride regimen should be implemented to prevent development of dental caries. Late effects of radiation include trismus and osteoradionecrosis. Trismus develops 3–6 months after radiation and is often life-long. It is attributed to muscle and ligament fibrosis and scarring, which causes a loss of flexibility and extension.24,25 Osteoradionecrosis has a similar clinical presentation to MRONJ and arises as a result of the irreversible damage to the osteocytes and microvascular system of the jaw from the radiation. In the current case these are unlikely as very low radiation doses were delivered compared to those routinely given.
Conclusion
This case demonstrates the difficulty in diagnosing lymphomas in the HNR and consequent delay in necessary treatment. Although lymphomas are an uncommon diagnosis, they cannot be dismissed when diagnosing HNR pathologies due to their diverse clinical presentation.