Hobson RS, Carter NE, Gilgrass TJ The interdisciplinary management of hypodontia: the relationship between an interdisciplinary team and the general dental practitioner. Br Dent J. 2003; 194:479-482
Brook AH. Dental anomalies of number, form and size: their prevalence in British schoolchildren. J Int Assoc Dent Child. 1974; 5:37-53
Mitchell D, Mitchell L. Oxford Handbook of Clinical Dentistry, 6th edn. : Oxford University Press; 2014
Patel K, Woolley A, Kelleher M. Clinical tips to improve the restorative management of hypodontia: part 1. Dent Update. 2022; 49:192-196
Gulati JS, Tabiat-Pour S, Watkins S, Banerjee A. Resin-bonded bridges – the problem or the solution? Part 1: assessment and design. Dent Update. 2016; 43:506-521 https://doi.org/10.12968/denu.2016.43.6.506
King PA, Foster LV, Yates RJ Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital. Br Dent J. 2015; 218:423-428 https://doi.org/10.1038/sj.bdj.2015.250
Jepson NJ, Nohl FS, Carter NE The interdisciplinary management of hypodontia: restorative dentistry. Br Dent J. 2003; 194:299-304 https://doi.org/10.1038/sj.bdj.4809940
Djemal S, Setchell D, King P, Wickens J. Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. Oral Rehabil. 1999; 26:302-320
Al-Ani AH, Antoun JS, Thomson WM Hypodontia: an update on its etiology, classification, and clinical management. Biomed Res Int. 2017; 2017 https://doi.org/10.1155/2017/9378325
Murray MC, Brunton PA, Osborne-Smith K, Wilson NH. Canine risers: indications and techniques for their use. Eur J Prosthodont Restor Dent. 2001; 9:137-140
Holliday R, Lush N, Chapple J Hypodontia: aesthetics and function part 2: management. Dent Update. 2014; 41:891-898
Pini NI, Marchi LM, Pascotto RC. Congenitally missing maxillary lateral incisors: update on the functional and esthetic parameters of patients treated with implants or space closure and teeth recontouring. Open Dent J. 2015; 8:289-294
Gervais MJ, Wilson PR. A rationale for retrievability of fixed, implant-supported prostheses: a complication-based analysis. Int J Prosthodont. 2007; 20:13-24
Clinical Tips to Improve the Restorative Management of Hypodontia: Part 2 Kajal B Patel Julian Woolley Martin Kelleher Dental Update 2024 49:4, 707-709.
Authors
Kajal BPatel
MChd/BChd, BSc, MFDS RCS (Ed)
Dental Core Trainee 2, King's College Dental Hospital
Hypodontia is defined as the developmental absence of one or several teeth. Management of cases of hypodontia can appear to be complex, but many aspects of the treatment could be managed in primary care. This article aims to enhance understanding and improve confidence in managing hypodontia cases in an appropriate way. This article is the second part of a two-part series offering clinical tips to help to improve the restorative management of hypodontia. The prevalence, aetiology, common features and some of the challenges in treating hypodontia cases were discussed in part 1.
CPD/Clinical Relevance: Many aspects of hypodontia can be managed effectively by interested and experienced GDPs who wish to treat suitable cases, while more complex cases can be referred for management by multidisciplinary teams in secondary care.
Article
Hypodontia is defined as the developmental absence of one or several teeth. It can be further subcategorized into oligodontia and anodontia. Oligodontia is a term that is often used in cases with more than six missing teeth. Anodontia is a rare condition characterized by the absence of all of the adult teeth.1 The prevalence of hypodontia is estimated as being between 0.1% and 0.9% in the primary dentition and between 3.5% and 6.5% in the secondary dentition.2 The aetiology of hypodontia is multifactorial although often follows a polygenic mode of inheritance.3 Patients with hypodontia can pose a range of challenges, but interested practitioners can help to achieve predictable, functional and aesthetic treatment outcomes for many of these patients.
General dental practitioners (GDPs) have an important role in the early diagnosis and possible referral to secondary care for advice or further treatment. Experienced practitioners can certainly manage many cases, and most GDPs should feel able to help with long-term maintenance.
Clinical challenges
Clinical challenges that need to be addressed when managing patients with hypodontia include:
When to refer to secondary care and the timing of interceptive treatment;
Making decisions about whether to open or close spaces;
Managing tooth size discrepancies, shades and positions (maxillary canines and microdonts);
Resolving issues about the design, materials and timing of resin-retained bridges (RRBs);
How to manage missing mandibular premolars;
Retention or removal of deciduous molars;
Managing infra-occlusion;
Timing of implant placement and the appropriateness of this treatment option;
Issues around long-term orthodontic retention/relapse.
Clinical tips for challenges 1–3 were covered in part 1 of the series,4 while challenges 4–9 are covered in this second part of the series.
Resolving issues about the design, materials and timing of resin-retained bridges
Resin-retained bridges (RRBs) have become increasingly popular, and there is significant evidence to demonstrate their survival rates.5 When designing the RRB, achieving adequate aesthetics can be challenging. When choosing the shade for the pontic, as with all tooth-coloured restorations, the dentist should first discuss whether the patient has any future aspirations about bleaching their teeth because bleaching after fitting an RRB can lead to a discrepancy between the tooth and pontic colour (Figures 1 and 2).
Figure 1. Note the yellow canines and the contrasting colours of the distally cantilevered pontics and anterior teeth. Although selective bleaching prior to bridge cementation should have resolved this issue earlier, it is still possible to selectively ‘retro-bleach’ the canines by producing labial reservoirs and cutting a window in the bleaching tray over the adjacent teeth.Figure 2. Note the unsatisfactory outcome due to the multiple colour and shape discrepancies (UL3 colour, UL4 pontic shape) and the poor posterior occlusal relationship at the end of this prolonged multidisciplinary treatment.
The use of double abutments is not advocated due to the increased risk of failure. Fixed-fixed RRBs have approximately double the rate of failure of a direct cantilever design with one tooth supporting one pontic.5,6 However, in cases where the upper central incisors have been orthodontically aligned, the so-called ‘Bristol Bridge’ design has been associated with successful outcomes. This design involves splinting of the two central incisors, and these serve as abutments for the missing upper lateral incisors. This design reduces the chances of orthodontic relapse, and the reported failure rate for this design in orthodontically treated hypodontia patients was only 8.7% over a 15-year follow up period.6
Figure 3 demonstrates a case with a positive outcome with a different style of adhesive bridgework at 26 years. The left side one was a direct mesial cantilever design. A TP retainer held the centrals together. The right side had double abutted premolars holding one pontic unit forward. The access screw hole to an implant can be seen at the bottom left of the picture.
Figure 3. Adhesive bridgework (replacing UL2 and UR3) reviewed 26 years after placement. The screw retained implant at UR6 was placed 15 years previously.
In cases where relapse is likely, such as cantilevering a replacement pontic forward from an orthodontically distalized canine, it is sensible to increase the surface area of the contact point between the pontic and anterior tooth (Figure 4). Firm, wide, wrap-around contacts on the distal surface of the adjacent central incisor reduced the chances of the pontic slipping. An example of a case with the pontic slipping mesially and relapse is illustrated in Figure 5.
Figure 4. The metal wing on the distalized canine (UL3) occupied the maximum surface area for adhesion. The firm wide contact between the pontic (UL2) and the central incisor stopped forward slippage.Figure 5. Relapse with mesial movements of the UL3 and UR3 meant that the pontics crossed over the distal surfaces of the upper central incisors and opened gaps between the canines and first premolars. The case had to be retreated.
For supplementary retention, a fixed retainer ought to be bonded to the palatal surfaces of the anterior teeth when they are not included within the indirect prosthesis.7
The design of the metal wing for RRBs in hypodontia
Retainers, that is the sandblasted metal wing of a RRB, should cover as much of the surface area of the abutment tooth as possible to maximize the bonding area (Figure 4). Extension to the interproximal areas and over the incisal edges should be considered.8
The patient should be warned about the metal incisal edge overlap prior to construction of the RRB. The use of guide planes may help to provide a suitable path of insertion and aid location. The connector height and width needs to be substantial to provide increased rigidity of the bridge.4 This can be difficult to achieve in cases involving microdont teeth, and the tooth with the greatest surface area should be chosen as the abutment tooth for any bridge.
The ‘shine through’ of the metal wing on the abutment tooth is a common aesthetic concern for patients. One clinical tip is to use a black ink pen (eg Stabilo Permanent Black Ink, Staedtler) to draw on the palatal surface of the abutment tooth before doing the shade matching. This helps to visualize the effect of a metal retainer before taking the final shade. The use of customized opaque resin cements can act as a useful adjunct to minimize metal shine through, particularly with very thin teeth with translucent enamel.
In the case of RRBs, although there are high survival rates, there is always a risk of failure. It is advised the patient has an Essix retainer made with a composite pontic. In the scenario of bridge failure, the patient should be instructed to wear their retainer recementation or construction of a new RRB depending on the reason for bridge failure. Wearing an Essix retainer with a pontic will prevent relapse and closure of the space.
Another acceptable method of filling the missing space of a lateral incisor is a fibre-reinforced composite bridge, particularly in adolescents. To construct a cantilever bridge, EverStick fibres (GC Corporation, Tokyo, Japan), or other fibres, can be used to provide a scaffolding structure. These fibres are bonded on to the palatal/lingual surface of the abutment tooth and extend in to the interproximal space, and the overlapping fibres are made rigid with flowable composite. This sub-structure can then be built with composite resin in to a pontic tooth shape as seen in Figure 6.
Figure 6.
(a) Pre-operative photograph demonstrating a missing lateral incisor (UL2) after selective bleaching of the maxillary canines and premolars. Note that the midline is 2 mm to the right and the central incisors are not vertically inclined. (b) Post-operative photograph. Occlusal view: UL2 (pontic)–UL3 fibre reinforced bridge. (c) Post-operative photograph. The UL2 is the pontic and the UL3 is the retainer for a fibre-reinforced bridge.
A section of Wedjet cord or a study model can be used in the planning stage to cut the required length of EverStick fibres prior to the patient attending the appointment. This process can be completed in one appointment, and does not require a laboratory stage, unlike a conventional RRB.
All-ceramic or zirconia RRBs are sometimes promoted as providing an aesthetic, biocompatible option for replacement of missing upper lateral incisors. However, there is a shortage of long-term studies to support their use. Anecdotally, there is a higher failure risk associated with all-ceramic RRBs, with fracturing of the framework being a commonly encountered problem. Increased thickness of the all-ceramic wing is required, and that requirement can run the risk of over-preparation of the abutment tooth and reduced bond strength owing to the exposed dentine.
Managing missing mandibular premolars
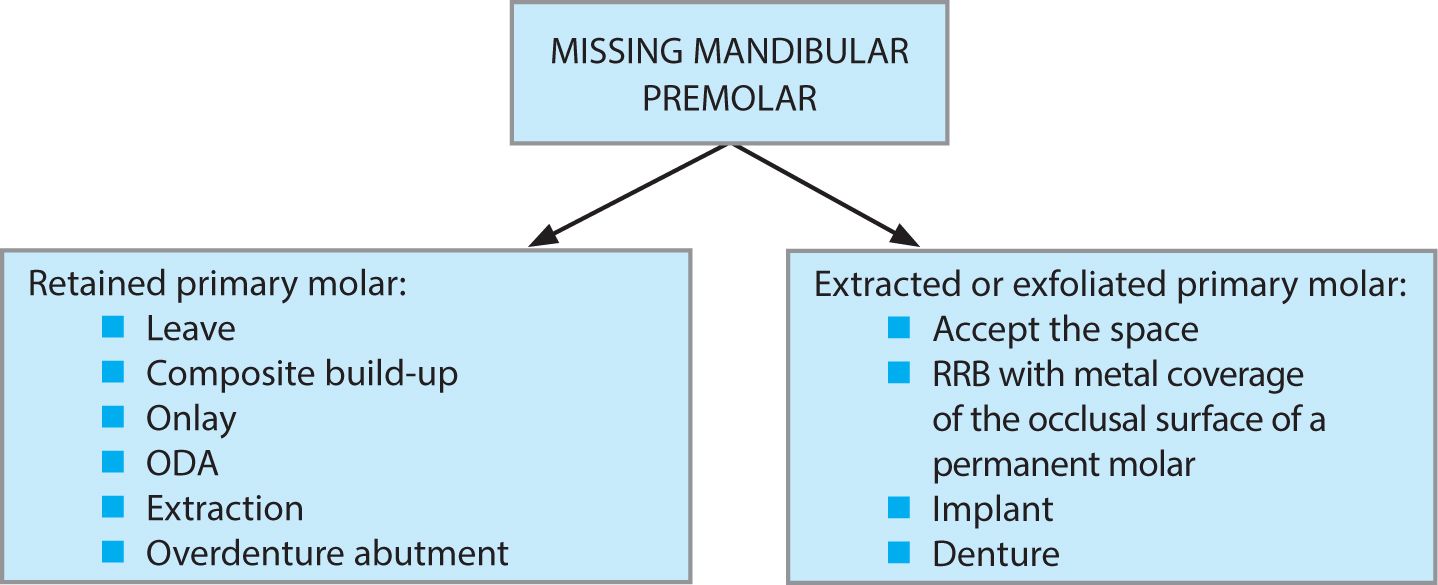
Hypodontia may result in missing premolars. The lower second premolars are the most likely to be missing.9 There are various management modalities dependent upon clinical presentation (Figure 7).
Figure 7. Flowchart demonstrating an overview of options for missing premolars
Making decisions about retaining or removing deciduous molars
In adults who have had no orthodontic intervention, when the primary molar has to be extracted or has exfoliated, the pontic space may be restored with an adhesive bridge. The pontic space may be split in to two, to provide two RRBs, each carrying one pontic.
The best retention is obtained by covering the occlusal aspect of the first permanent molar with an extensive metal wing.10 However, the patient and parent both need to be warned – in advance and in writing – that the metal wing will then be visible when the mouth is open. Minimal coverage types of retainers, which do not cover the occlusal surface of the molar tooth, but instead are held on the lingual surface of the molar, have had high failure rates. In all probability, this is because the wing is not made thick enough to prevent flexing, and resin composite performs poorly when it is subjected to shear and/or tensile forces.
A ‘canine riser’ resin composite restoration may be used to provide canine guidance and reduce excessive loading forces on the restored tooth/teeth. This involves composite being bonded to the palatal and incisal surfaces of the maxillary canines to produce canine guidance.10
There are multiple considerations for cases with missing premolars if the retained primary tooth is present. Retained primary second molars (Es) may remain in occlusion or become infra-occluded if they become ankylosed.
The retained primary molar is wider than its adult successor. In some cases, the contour of the retained second deciduous molar can cause difficulties in cleaning effectively, occasionally leading to caries, but only if frequency of sugar is a problem. In other cases, with patients with good oral hygiene practice and a low sugar diet, the shape discrepancy is often not that much of a concern. Direct composite resin may be added to the teeth to create a more desirable shape. Challenges include reduced bond strength to deciduous enamel. That can be overcome by gentle macro-mechanical roughening with a bur before etching and bonding. The short roots are often divergent and may be ankylosed; they can frequently be retained for many years whether built up or not.
If the treatment plan includes the maintenance of deciduous teeth for an extended period, the patient should be warned about the possible risk of loss of the primary tooth at some point. Should this occur, one option is to accept the space, but alternative options are illustrated in Figure 7.
Managing infra-occlusion
If the deciduous molar is infra-occluded, the gingival and occlusal levels may lie in an apical position.11 An onlay, resin-composite build up or an extraction can be considered in cases of infra-occlusion. Early extraction may be considered if the infra-occlusion is progressive and space closure is desired. However, full space closure may be challenging given the width of a deciduous molar in mesial–distal dimensions in comparison with an adult premolar.
An ankylosed deciduous molar acts virtually like an implant and preserves the bone. Conversely, a traumatic extraction to remove it grossly reduces the remaining bone and produces ‘alveolar necking’ with a minimal zone of attached gingival tissue often then being left. This combination can make subsequent implant placement much less predictable.
If undergoing orthodontic treatment, ‘interproximal stripping’ could be considered to reduce the mesial–distal space and possibly allow for more options for replacement. With this treatment approach, one must be mindful of root angulation if considering removal, as many retained deciduous second molars will have divergent roots.
Timing of implant placement and appropriateness of this treatment option
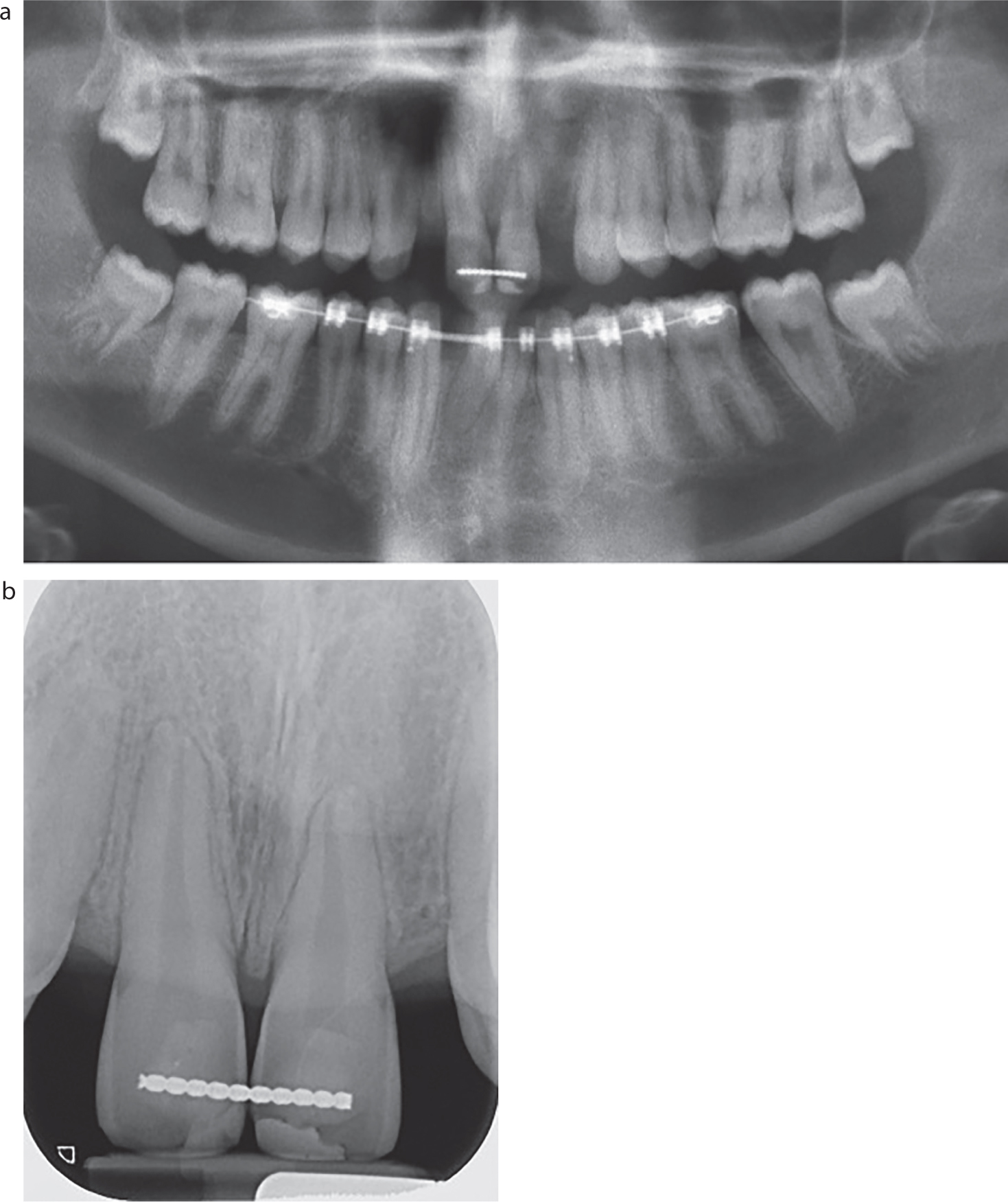
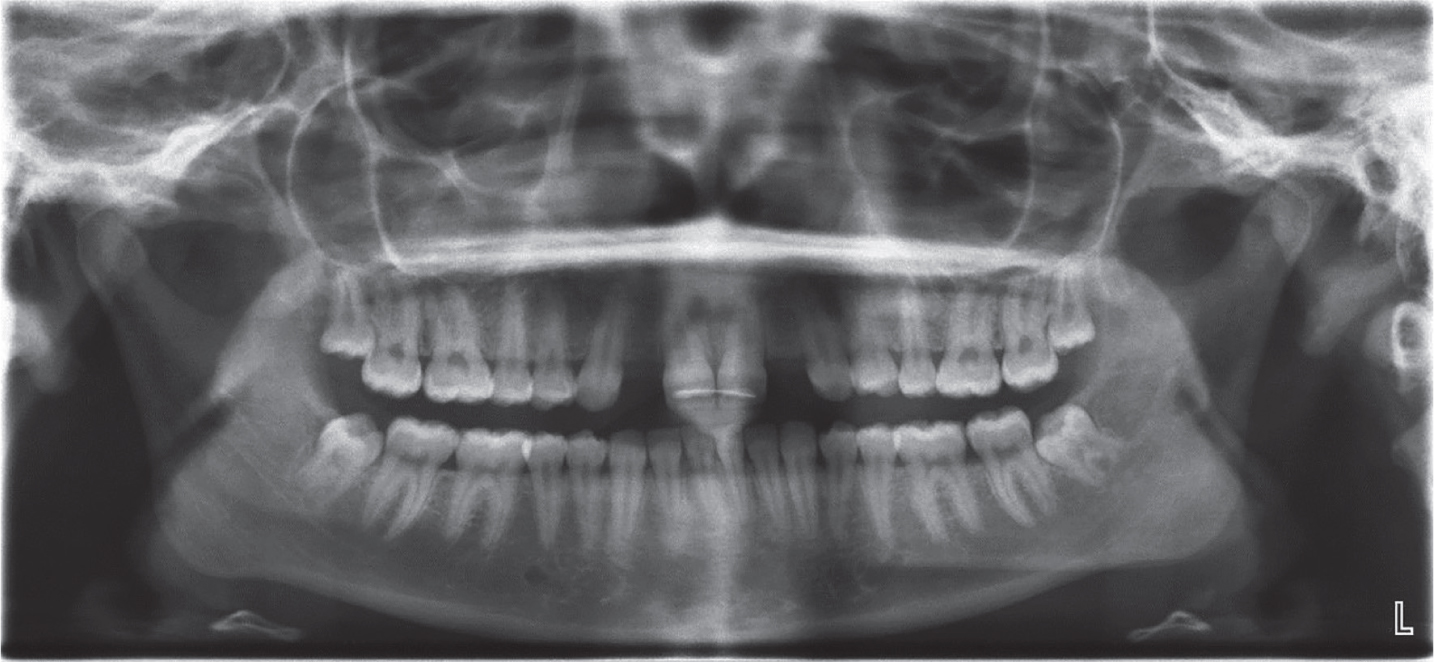
The use of implants to replace maxillary lateral incisors is just one of many treatment options. The requirements for implant placement can result in a very long course of preparatory treatment, and can only be completed after growth cessation in a patient in their late teens or early twenties (Figure 8).
Figure 8. Two implants have been placed in the premolar regions.
The use of implants as a treatment modality is often considered initially to be the most desirable one by some patients and by their parents. However, that view is often based on very limited knowledge of the many negative issues that implants can have in the medium and long term. One must ensure that both the patient's and parents' expectations are realistic and that the patient is fully aware that implants will be ‘neither perfect nor permanent’.
Many mechanical and biological complications have been reported, including osseo-integration failure and peri-implantitis. Therefore one must be cautious and mindful that implants do not always provide a high success rate, especially when there is scarcity of good quality bone and soft tissue.12
If an implant approach is to be viable, then sophisticated fixed appliance orthodontic skills need to be readily available to move the roots away from one another, and for them to be kept parallel to one another all the way to the apices. There has to be adequate clearance maintained until implant placement.
This was not achieved in the cases in Figures 9 and 10, thus preventing the implant option that had been planned.
Figure 9.
(a) Distalized maxillary canines with inadequate clearance for implants due to central incisor apical positions in both upper and lower arches. (b) Distalized maxillary canines with inadequate clearance for implants.Figure 10. Mesial root inclination of the UR3 and UL3 resulting in lack of space for an implant.
If choosing this treatment modality, the roots need to be adequately torqued and not encroach upon the minimum required space of approximately 7 mm for implant placement in the maxillary lateral incisor region at the appropriate angulation.13
The presence or absence of maxillary bone in the lateral incisor region is a major consideration. If, as is usually the case with missing maxillary incisors, there is deficiency of either hard or soft tissues or of both, then grafting may well be required to facilitate successful implant placement. The placement of the implants needs to be restoratively driven, with sophisticated clinical skills and excellent technical support being available, both before and after implant placement and restoration.
Following implant placement, maintenance by a general dental practitioner or by a specialist is desirable. One major complication with implants is peri-implant diseases. It is important that this is diagnosed when presenting in primary care. Peri-implant diseases include peri-implant mucositis and peri-implantitis. The British Society of Periodontology's guidelines advocate regular monitoring of peri-implant health in the form of clinical assessment and radiographs.14
Clinicians should note that probing around implants with a periodontal probe does not inflict damage to the implant or surrounding mucosa, and so this should not be avoided.14 Baseline probing depths should be recorded and compared at subsequent recall. If a diagnosis of peri-implantitis is derived, specialist referral is advisable.14
Long-term orthodontic retention/relapse
For patients who have undergone orthodontic treatment, there is always a risk of relapse. This means that patients must accept a lifetime of indefinite retention with associated costs. Patients need to understand and accept that fully. Some patients may claim not to have understood that risks were involved when problems manifest. In such cases, clearly documented evidence that there were many honest discussions and a signed copy of a consent form can provide the best defence.
If an implant is planned following orthodontic treatment, there will be a requirement for very effective space maintenance in three dimensions to prevent orthodontic relapse prior to restorative rehabilitation. This effectively means that treatment for a couple of missing teeth can easily extend in to a patient's very late teenage years when growth has ceased. Many mechanical and aesthetic complications with implants have been reported over many years even when excellent clinical and technical skills have been employed by specialists.15 Caution is advised and modesty in one's promises to patients with hypodontia is prudent.
Another option is a removable partial denture (RPD). RPDs aid in improving appearance and can provide a more than acceptable aesthetic solution for cases with multiple missing teeth in the maxillary and mandibular arches. The main disadvantage is that they are removable rather than fixed. However, that insecurity can be allayed to some extent by having spare dentures made in the case of damage to their initial set.
Discussion
Prior to the commencement of treatment, liaising with an orthodontic department will help to ensure appropriate, timely care is provided and hopefully lead to better patient outcomes.
Treatment extends over a number of years in primary and secondary care. Given the wide range of treatment options available, for consent to be valid, the patient must understand the Montgomery ‘material risks’ and limitations as well as the possible benefits of each viable treatment option.16
Following treatment in secondary care, patients need to be able to develop a functional working relationship with a GDP for ongoing maintenance. Composite restorations will deteriorate over time, but can be refreshed at recall visits to maintain aesthetics. A fairer reward system within the new NHS contract might have allowed for the assessment of indirect restorations or implants if used, but unfortunately, those pilot schemes are now history. Although some GDPs might not wish to engage with addressing some of the more complex issues, they have an important role in recognizing problems and instigating referrals to colleagues for further management as appropriate.
Conclusion
A wide number of restorative challenges present in hypodontia cases. The various clinical tips described may be helpful in achieving aesthetic and functional outcomes and facilitate long-term maintenance.