Oosterink FM, de Jongh A, Aartman IH. What are people afraid of during dental treatment? Anxiety-provoking capacity of 67 stimuli characteristic of the dental setting. Eur J Oral Sci. 2008; 116:44-51 https://doi.org/10.1111/j.1600-0722.2007.00500.x
Armfield JM, Stewart JF, Spencer AJ. The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health. 2007; 7 https://doi.org/10.1186/1472-6831-7-1
Locker D, Shapiro D, Liddell A. Negative dental experiences and their relationship to dental anxiety. Community Dent Health. 1996; 13:86-92
Nusstein J, Reader A, Beck FM. Anesthetic efficacy of different volumes of lidocaine with epinephrine for inferior alveolar nerve blocks. Gen Dent. 2002; 50:372-375
Renton T. Optimal local anaesthesia for dentistry. Prim Dent J. 2019; 7:51-61
Malamed SF. Handbook of Local Anesthesia, 7th edn. : Elsevier Health Sciences; 2019
Kaufman E, Weinstein P, Milgrom P. Difficulties in achieving local anesthesia. J Am Dent Assoc. 1984; 108:205-208
Meechan JG. How to overcome failed local anaesthesia. Br Dent J. 1999; 186:15-20
Meechan JG. The use of the mandibular infiltration anesthetic technique in adults. J Am Dent Assoc. 2011; 142:19S-24S
You TM, Kim K-D, Huh J The influence of mandibular skeletal characteristics on inferior alveolar nerve block anesthesia. J Dent Anesth Pain Med. 2015; 15:113-119
Takasugi Y, Furuya H, Moriya K, Okamoto Y. Clinical evaluation of inferior alveolar nerve block by injection into the pterygomandibular space anterior to the mandibular foramen. Anesth Prog. 2000; 47:125-129
Kim C, Hwang K-G, Park C-J. Local anesthesia for mandibular third molar extraction. J Dent Anesth Pain Med. 2018; 18:287-294
Afsar A, Haas DA, Rossouw PE, Wood RE. Radiographic localization of mandibular anesthesia landmarks. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 1998; 86:234-241
Hannan L, Reader A, Nist R The use of ultrasound for guiding needle placement for inferior alveolar nerve blocks. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 1999; 87:658-665
Harris SC. Problems of experimental algesimetry and a comment on the tooth pulp method. J Chron Dis. 1956; 4:52-58
McLean C, Reader A, Beck M, Meyers WJ. An evaluation of 4% prilocaine and 3% mepivacaine compared with 2% lidocaine (1:100,000 epinephrine) for inferior alveolar nerve block. J Endod. 1993; 19:146-150
Mikesell P, Nusstein J, Reader A A comparison of articaine and lidocaine for inferior alveolar nerve blocks. J Endod. 2005; 31:265-270
Certosimo AJ, Archer RD. A clinical evaluation of the electric pulp tester as an indicator of local anesthesia. Oper Dent. 1996; 21:25-30
Vreeland DL, Reader A, Beck M An evaluation of volumes and concentrations of lidocaine in human inferior alveolar nerve block. J Endod. 1989; 15:6-12
Hinkley SA, Reader A, Beck M, Meyers WJ. An evaluation of 4% prilocaine with 1:200,000 epinephrine and 2% mepivacaine with 1:20,000 levonordefrin compared with 2% lidocaine with:100,000 epinephrine for inferior alveolar nerve block. Anesth Prog. 1991; 38:84-89
Renton T. Trigeminal nerve injuries. Aust Endod J. 2018; 44:159-169
Kung J, McDonagh M, Sedgley CM. Does articaine provide an advantage over lidocaine in patients with symptomatic irreversible pulpitis? A systematic review and meta-analysis. J Endod. 2015; 41:1784-1794
Hargreaves KM, Keiser K. Local anesthetic failure in endodontics. Endod Topic. 2002; 1:26-39
Fowler S, Drum M, Reader A, Beck M. Anesthetic success of an inferior alveolar nerve block and supplemental articaine buccal infiltration for molars and premolars in patients with symptomatic irreversible pulpitis. J Endod. 2016; 42:390-392
Nguyen V, Chen Y-W, Johnson JD, Paranjpe A. In vivo evaluation of effect of preoperative ibuprofen on proinflammatory mediators in irreversible pulpitis cases. J Endod. 2020; 46:1210-1216
Wallace JA, Michanowicz AE, Mundell RD, Wilson EG. A pilot study of the clinical problem of regionally anesthetizing the pulp of an acutely inflamed mandibular molar. Oral Surg Oral Med Oral Pathol. 1985; 59:517-521
Roy ML, Narahashi T. Differential properties of tetrodotoxin-sensitive and tetrodotoxin-resistant sodium channels in rat dorsal root ganglion neurons. J Neurosci. 1992; 12:2104-2111
Gold MS, Reichling DB, Shuster MJ, Levine JD. Hyperalgesic agents increase a tetrodotoxin-resistant Na+ current in nociceptors. Proc Natl Acad Sci U S A. 1996; 93:1108-1112
Pulikkotil SJ, Nagendrababu V, Veettil SK Effect of oral premedication on the anaesthetic efficacy of inferior alveolar nerve block in patients with irreversible pulpitis. A systematic review and network meta-analysis of randomized controlled trials. Int Endod J. 2018; 51:989-1004
Shirvani A, Shamszadeh S, Eghbal MJ Effect of preoperative oral analgesics on pulpal anesthesia in patients with irreversible pulpitis-a systematic review and meta-analysis. Clin Oral Investig. 2017; 21:43-52
Corbella S, Taschieri S, Mannocci F Inferior alveolar nerve block for the treatment of teeth presenting with irreversible pulpitis: a systematic review of the literature and meta-analysis. Quintessence Int. 2017; 48:69-82
Kaladi SR, Tegginmani V, Mitta S Effectiveness of pre-operative oral medication of ibuprofen and ketorolac on anesthetic efficacy of inferior alveolar nerve block with irreversible pulpitis: randomized controlled trial. Cureus. 2019; 11
Parirokh M, Ashouri R, Rekabi AR The effect of premedication with ibuprofen and indomethacin on the success of inferior alveolar nerve block for teeth with irreversible pulpitis. J Endod. 2010; 36:1450-1454
Shantiaee Y, Javaheri S, Movahhedian A Efficacy of preoperative ibuprofen and meloxicam on the success rate of inferior alveolar nerve block for teeth with irreversible pulpitis. Int Dent J. 2017; 67:85-90
Saha SG, Jain S, Dubey S Effect of oral premedication on the efficacy of inferior alveolar nerve block in patients with symptomatic irreversible pulpitis: a prospective, double-blind, randomized controlled clinical trial. J Clin Diagn Res. 2016; 10:ZC25-29
Bidar M, Mortazavi S, Forghani M, Akhlaghi S. Comparison of effect of oral premedication with ibuprofen or dexamethasone on anesthetic efficacy of inferior alveolar nerve block in patients with irreversible pulpitis: a prospective, randomized, controlled, double-blind study. Bull Tokyo Dent Coll. 2017; 58:231-236
Aggarwal V, Singla M, Kabi D. Comparative evaluation of effect of preoperative oral medication of ibuprofen and ketorolac on anesthetic efficacy of inferior alveolar nerve block with lidocaine in patients with irreversible pulpitis: a prospective, double-blind, randomized clinical trial. J Endod. 2010; 36:375-378
Oleson M, Drum M, Reader A Effect of preoperative ibuprofen on the success of the inferior alveolar nerve block in patients with irreversible pulpitis. J Endod. 2010; 36:379-382
Shahi S, Mokhtari H, Rahimi S Effect of premedication with ibuprofen and dexamethasone on success rate of inferior alveolar nerve block for teeth with asymptomatic irreversible pulpitis: a randomized clinical trial. J Endod. 2013; 39:160-162
Yadav S. Anesthetic success of supplemental infiltration in mandibular molars with irreversible pulpitis: a systematic review. J Conserv Dent. 2015; 18:182-186
Kanaa MD, Whitworth JM, Meechan JG. A prospective randomized trial of different supplementary local anesthetic techniques after failure of inferior alveolar nerve block in patients with irreversible pulpitis in mandibular teeth. J Endod. 2012; 38:421-425
Haase A, Reader A, Nusstein J Comparing anesthetic efficacy of articaine versus lidocaine as a supplemental buccal infiltration of the mandibular first molar after an inferior alveolar nerve block. J Am Dent Assoc. 2008; 139:1228-1235
Gao X, Meng K. Comparison of articaine, lidocaine and mepivacaine for buccal infiltration after inferior alveolar nerve block in mandibular posterior teeth with irreversible pulpitis. Br Dent J. 2020; 228:605-608
Meechan JG. Infiltration anesthesia in the mandible. Dent Clin North Am. 2010; 54:621-629
Leonard MS. The efficacy of an intraosseous injection system of delivering local anesthetic. J Am Dent Assoc. 1995; 126:81-86
Dunbar D, Reader A, Nist R Anesthetic efficacy of the intraosseous injection after an inferior alveolar nerve block. J Endod. 1996; 22:481-486
Nusstein J, Reader A, Nist R Anesthetic efficacy of the supplemental intraosseous injection of 2% lidocaine with 1:100,000 epinephrine in irreversible pulpitis. J Endod. 1998; 24:487-491
Stabile P, Reader A, Gallatin E Anesthetic efficacy and heart rate effects of the intraosseous injection of 1.5% etidocaine (1:200,000 epinephrine) after an inferior alveolar nerve block. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2000; 89:407-411
Meechan JG. Supplementary routes to local anaesthesia. Int Endod J. 2002; 35:885-896
Olley RC, Renton TF, Frost PM. Intraligamentary local anaesthesia for posterior mandibular extractions. Dent Update. 2020; 47:213-216
Kämmerer PW, Adubae A, Buttchereit I Prospective clinical study comparing intraligamentary anesthesia and inferior alveolar nerve block for extraction of posterior mandibular teeth. Clin Oral Investig. 2018; 22:1469-1475
Webber B, Orlansky H, Lipton C, Stevens M. Complications of an intra-arterial injection from an inferior alveolar nerve block. J Am Dent Assoc. 2001; 132:1702-1704
Haas DA. An update on local anesthetics in dentistry. J Can Dent Assoc. 2002; 68:546-552
Hillerup S, Jensen R. Nerve injury caused by mandibular block analgesia. Int J Oral Maxillofac Surg. 2006; 35:437-443
Tzermpos FH, Cocos A, Kleftogiannis M Transient delayed facial nerve palsy after inferior alveolar nerve block anesthesia. Anesth Prog. 2012; 59:22-27
von Arx T, Lozanoff S, Zinkernagel M. Ophthalmologic complications after intraoral local anesthesia. Swiss Dent J. 2014; 124:784-806
Baldi C, Bettinelli S, Grossi P Ultrasound guidance for locoregional anesthesia: a review. Minerva Anestesiol. 2007; 73:587-593
Jung I-Y, Kim J-H, Kim E-S An evaluation of buccal infiltrations and inferior alveolar nerve blocks in pulpal anesthesia for mandibular first molars. J Endod. 2008; 34:11-13
Brandt RG, Anderson PF, McDonald NJ The pulpal anesthetic efficacy of articaine versus lidocaine in dentistry: a meta-analysis. J Am Dent Assoc. 2011; 142:493-504
Poorni S, Veniashok B, Senthilkumar AD Anesthetic efficacy of four percent articaine for pulpal anesthesia by using inferior alveolar nerve block and buccal infiltration techniques in patients with irreversible pulpitis: a prospective randomized double-blind clinical trial. J Endod. 2011; 37:1603-1607
Parirokh M, Satvati SA, Sharifi R Efficacy of combining a buccal infiltration with an inferior alveolar nerve block for mandibular molars with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endodont. 2010; 109:468-473
Oulis CJ, Vadiakas G, Vasilopoulou A. The effectiveness of mandibular infiltration compared to mandibular block anesthesia in treating primary molars in children. Pediatr Dent. 1996; 18:301-305
Smith T, Urquiola R, Oueis H, Stenger J. Comparison of articaine and lidocaine in the pediatric population. J Mich Dent Assoc. 2014; 96:34-37
Meechan JG, Ledvinka JI. Pulpal anaesthesia for mandibular central incisor teeth: a comparison of infiltration and intraligamentary injections. Int Endod J. 2002; 35:629-634
Jaber A, Whitworth JM, Corbett IP The efficacy of infiltration anaesthesia for adult mandibular incisors: a randomised double-blind cross-over trial comparing articaine and lidocaine buccal and buccal plus lingual infiltrations. Br Dent J. 2010; 209:E16-E16
Corbett IP, Kanaa MD, Whitworth JM, Meechan JG. Articaine infiltration for anesthesia of mandibular first molars. J Endod. 2008; 34:514-518
Heller AA, Shankland WE. Alternative to the inferior alveolar nerve block anesthesia when placing mandibular dental implants posterior to the mental foramen. J Oral Implantol. 2001; 27:127-133
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
Local anaesthesia is a sine qua non for pain management in dentistry. Optimizing local anaesthesia practice reduces intra-operative pain, and ultimately ameliorates patient comfort. Many patients still report experiencing intra-operative pain despite being anaesthetized. This is commonplace with inferior alveolar nerve blocks, the current routine approach to mandibular anaesthesia. This technique has been shown, in many cases, to fail at first attempt and can be uncomfortable for patients. It has a higher positive-aspiration rate than other techniques, increasing the risk of systemic complications.
CPD/Clinical Relevance: Clinicians should be aware of more effective techniques for mandibular anaesthesia for optimal and safe pain management, and ultimately a better patient experience.
Article
Generally, the anticipation of painful or invasive procedures is the greatest source of anxiety for patients in dentistry.1 Evidence suggests that patients who have high levels of dental anxiety avoid appointments, and so may have poor oral health.2 This ‘vicious cycle of dental fear’ (Figure 12) highlights the significance of optimizing pain control in the dental setting.
Figure 1. The ‘vicious cycle of dental fear’ redrawn from Armfield et al.2
Local anaesthesia (LA) is key to pain control in dentistry, and there is a plethora of articles suggesting how its use can be optimized. Nevertheless, the most commonly reported adverse event in dental practice is intra-operative pain.3 In a representative sample of the general population, 71% reported having painful dental experiences,4 implying that pain management in dentistry has yet to reach its pinnacle.
At present, dentists rely mostly on the inferior alveolar nerve block (IANB) for providing mandibular anaesthesia. However, IANBs often fail to provide adequate pulpal anaesthesia at the first attempt.5,6
This article reviews the misconceptions surrounding the use of IANBs, and outlines ways to prevent and manage IANB failures and complications. Evidence-based safe and optimal LA practice is explored.
Tackling IANB misconceptions
There is no standard success rate for IANBs. Failure rates of IANBs vary extensively from 31% to 81%.7 Dentists often struggle to identify the reasons for IANB failure, which could be due to several misconceptions regarding their use. These include:
Aiming for the nerve;
Determining the onset of pulpal anaesthesia;
Waiting for the onset of LA;
Articaine versus lidocaine.
Different procedures may yield different anaesthetic efficacies: it is more probable that exodontia under LA will be less painful compared to endodontic treatment, for which it is more challenging to provide profound anaesthesia.8
Aiming for the nerve
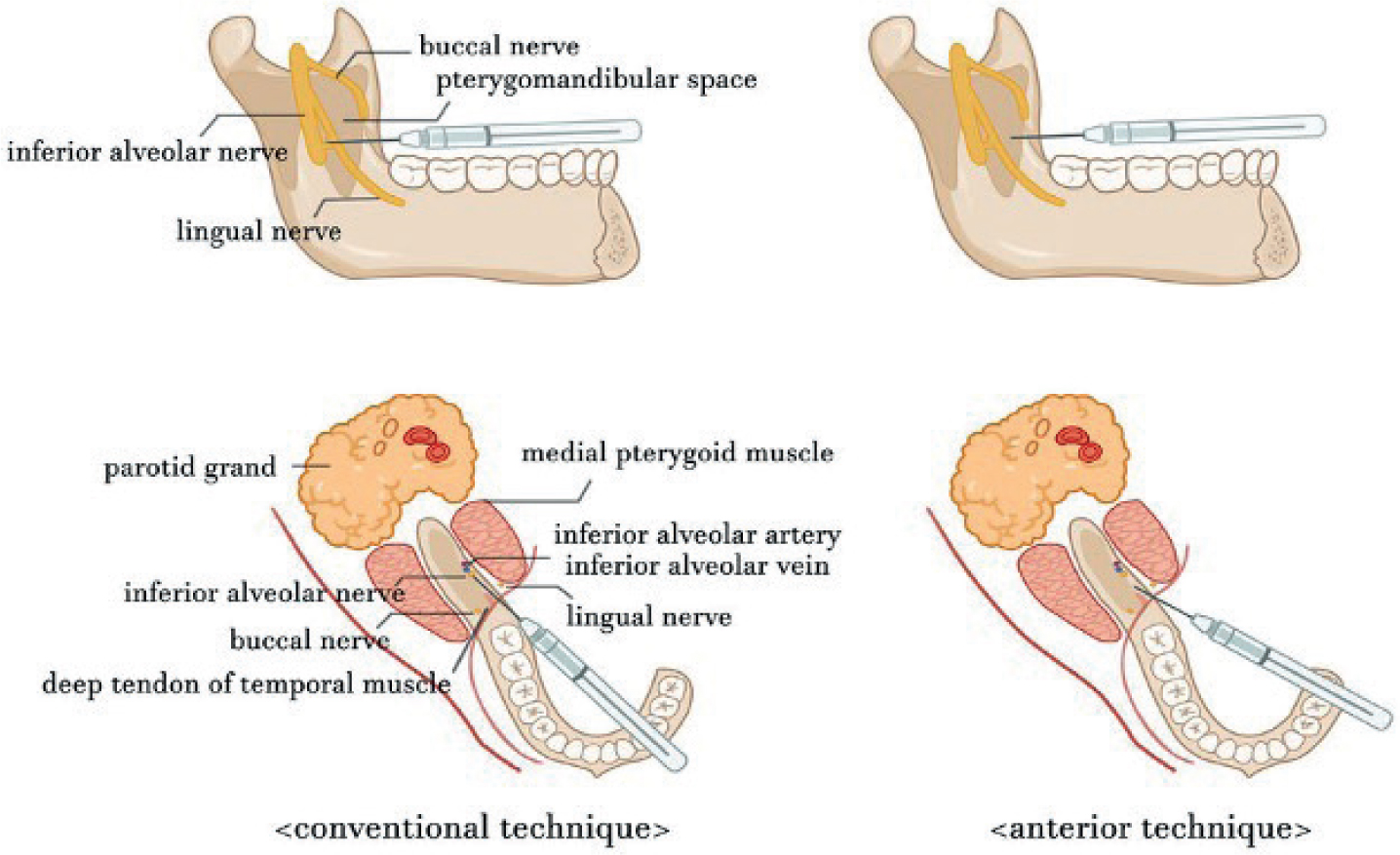
It is thought that an important determinant of a successful IANB is access to the mandibular foramen;7,9,10,11 therefore, some clinicians aim to inject as close as possible to the inferior alveolar nerve.12
Takasugi et al12 studied an alternative method to the conventional IANB, the ‘anterior technique’, involving the injection of the LA more anterior to the mandibular foramen (Figure 2).13 This method relies on the diffusion of the solution towards the inferior alveolar nerve. The results were compared to other studies of the conventional IANB, and it was found that injecting further from the mandibular foramen, as in the anterior technique, does not lower the effectiveness of IANBs. The anterior technique also has a lower risk of nerve injury than conventional IANBs.12
Figure 2. Illustration comparing the conventional IANB with the anterior technique with regards to needle insertion sites. For the anterior technique, the needle should be inserted on the lateral side of the pterygomandibular fold, approximately 10 mm above the occlusal plane. The syringe barrel should be positioned over the contralateral first mandibular molar. The penetration depth is approximately 10 mm.13
Panoramic radiographs14 and ultrasound-guided needle insertion15 can be used by the operator to more accurately locate the mandibular foramen. Yet, neither radiography nor ultrasonography improve the success of IANBs,14,15 implying that anatomically accurate injection sites do not guarantee optimal analgesia.
In summary, evidence supports that there is no need to place the needle tip adjacent to the nerve for optimizing IANB efficacy, as it only increases the risk of inferior alveolar nerve and lingual nerve injury.
Determining the onset of pulpal anaesthesia
It is often assumed that pulpal anaesthesia has been achieved after confirming lip numbness.8 However, soft-tissue numbness is highly subjective, being confounded by the patient's psychological and physiological status.16 Studies have confirmed that the absence of mucosal responsiveness does not always indicate successful pulpal anaesthesia.17,18
A more accurate and objective method to confirm pulpal anaesthesia is electrical pulp testing (EPT). This method has been successfully used in LA efficacy tests for healthy and symptomatic teeth.16,19
However, the ideal way to ensure that maximum pulpal anaesthesia is achieved, is through waiting a sufficient time for the IANB to take effect.
Waiting for the onset of LA
Do dentists wait a sufficient length of time for the onset of pulpal anaesthesia following an IANB?
Lip numbness happens 5–9 minutes after the injection, but the pulp becomes anaesthetized after 15–16 minutes.17,20,21
Delayed onset can occur in 19–27% of cases, and an onset after 30 minutes has been reported for 8% of patients.5 Despite achieving lip numbness, patients may still feel intra-operative pain. In such situations, some clinicians administer an extra IANB. However, this does not improve the analgesia because the operator may not have waited enough time for the first injection to take effect.5 Administering multiple IANBs can also increase the risk of nerve injury.22
In summary, clinicians must wait a longer time for the onset of anaesthesia with IANBs. If the IANB demonstrated success at first attempt after waiting, there is no indication for another injection. The management of a failed IANB will be discussed in the next section of this review.
Articaine versus lidocaine
The efficacy of articaine IANBs is not significantly different to lidocaine for healthy teeth18 or in patients with irreversible pulpitis.23 Furthermore, studies have found there to be a greater risk of nerve injury and paraesthesia associated with 4% articaine IANBs, compared to 2% lidocaine.22
Thus, considering the potential concerns surrounding neurotoxicity, 4% articaine is not routinely recommended for IANBs; 2% lidocaine is as effective.
IANBs and inflammation
The provision of successful anaesthesia is even more challenging in endodontics; inflamed tissue immensely reduces the effectiveness of IANBs.24,25 In a study of patients with irreversible pulpitis, the success rate of lidocaine IANBs for first and second molars was 28% and 25%, respectively.25
This has been ascribed to increasing levels of inflammatory mediators, such as prostaglandin E2 (PGE2). Inflammation also changes sodium channel expression and function in nociceptors.24
Elevated PGE2 levels sensitize nociceptors, reducing their excitability threshold for activation.24,26 Consequently, the LA agent may be insufficient to prevent impulse propagation.27
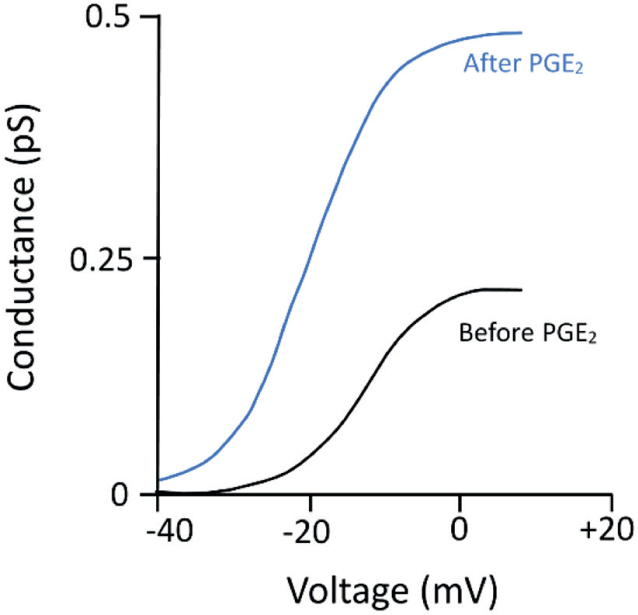
Pulpal nociceptors express various classes of sodium channels including tetrodotoxin-resistant (TTXr) channels, which are four times less sensitive to lidocaine than other channels.28 With inflammation, nociceptors express more TTXr channels, and after exposure to PGE2, the activity of these lidocaine-resistant channels more than doubles (Figure 3).29
Figure 3. The effect of adding PGE2 on the conductance–voltage relationship of TTXr channels. After the addition of 1 µM PGE2, the conductance of TTXr channels approximately doubles, and the activation threshold voltage decreases. Figure redrawn from Gold et al.29
Failure of IANBs in the presence of inflammation calls for measures, such as anti-inflammatory premedication and supplementary LA (additional injections with modified technique/solution), to enhance anaesthesia.
Managing IANB failures
Planning ahead is imperative for optimal LA. Practitioners should identify patients who are more likely to experience poor anaesthesia, such as patients with inflammation, and consider the strategies below before treatment. Patients who have responded poorly to LA in the past are more likely to experience further LA-associated difficulties.24 Thus, history-taking is vital. The following approaches can be taken in these patients:24
Oral premedication with anti-inflammatory drugs (in patients with inflammation);
Supplementary LA.
Premedication
A recent meta-analysis found that pre-operative oral non-steroidal anti-inflammatory drugs (NSAIDs) or dexamethasone can significantly increase the efficacy of IANBs for patients with irreversible pulpitis.30 These drugs reduce pulpal levels of inflammatory mediators (eg PGE2), thus precluding peripheral sensitization and increased activity of lidocaine-resistant TTXr channels.24
NSAIDs
Pre-operative NSAIDs (eg ibuprofen, oxicams, indomethacin and ketorolac) have been reported to significantly increase the success of IANBs in patients with irreversible pulpitis by several meta-analyses.30,31,32 NSAIDs inhibit the cyclo-oxygenase pathway, preventing prostaglandin synthesis.33 A recent study found significantly lower concentrations of inflammatory mediators in the pulp, including PGE2, when 600 mg ibuprofen was given to patients with irreversible pulpitis 1 hour before LA.26
A randomized controlled trial (RCT) found that both 75 mg indomethacin and 600 mg ibuprofen given 1 hour before the IANB significantly increased LA success in patients with irreversible pulpitis.34The two NSAIDs were not significantly different in efficacy. The authors suggested that ibuprofen may be favoured over indomethacin because it has fewer side-effects than the latter. Shantiaee et al35 also reported a significant increase in anaesthesia with 7.5 mg meloxicam or 600 mg ibuprofen 1 hour preceding the IANB. No difference was found between the two NSAIDs.
Ketorolac (10 mg36 or 20 mg33) also increased the effectiveness of lidocaine IANBs in some studies.
Multiple RCTs have demonstrated the increase in anaesthesia with pre-operative ibuprofen.34,35,37 However, in other studies, ibuprofen had no effect on IANB success.38,39 The patients in these latter studies had irreversible pulpitis with spontaneous pain, suggestive of high pulpal levels of prostaglandins released previously. Prostaglandin synthesis is inhibited by ibuprofen, but the antecedent alteration in nociceptor activity still exists. It is proposed that premedication in patients with spontaneous pain is less effective than those with irreversible pulpitis without spontaneous pain.34
Dexamethasone
Dexamethasone (0.5 mg40 or 4 mg37) improves the IANB success in patients with symptomatic and asymptomatic irreversible pulpitis. It is noteworthy that ibuprofen37/NSAIDs30 and dexamethasone are not significantly different in their effect on anaesthesia. Further studies are needed for a more definitive recommendation.
Paracetamol
Meta-analyses have shown that paracetamol monotherapy does not improve anaesthesia at any dose.30,31 However, when combined with NSAIDs (namely 400 mg ibuprofen), IANB success does significantly increase.30
Nevertheless, NSAIDs alone have a comparable efficacy to paracetamol + NSAID combinations. This implies that adding paracetamol to NSAID premedication offers little advantage to the effect of NSAIDs on block anaesthesia.30
Dosage and timing
Shirvani et al31 found no link between the timing and dosage of pre-operative analgesics and the effect on anaesthesia. This meta-analysis included timings between 30 and 60 minutes before IANB administration. It is suggested that giving the premedication 1 hour before the IANB allows the drug to reach satisfactory plasma concentration.38
In another meta-analysis, IANB success was only increased with doses of ibuprofen equal to or greater than 400 mg.30
To summarize, for patients presenting with pulpitis, it is favourable to prescribe pre-operative NSAIDs before IANB administration, to increase the chances of successful anaesthesia – especially for pulpitic molars. However, case selection is imperative. Some procedures that require a greater depth of anaesthesia (eg root canal treatment, or exodontia) will benefit more from anti-inflammatory premedication, compared to others (eg superficial restorations).
Even with pre-operative medication, the studies did not achieve profound anaesthesia, which is necessary for endodontic treatment, potentially owing to the presence of already-sensitized nociceptors. Hence, clinicians may plan to use supplemental LA to further increase the depth of anaesthesia.
Supplementary injections
Supplementary injections have been shown to increase the efficacy of IANBs. These include: intraligamental, intra-osseous and buccal infiltrations.41 In an RCT,42 100 of 182 patients with irreversible pulpitis required supplemental injections following failed IANBs (2% lidocaine with 1:80,000 adrenaline). There was a greater success with articaine buccal infiltrations and intra-osseous injections, compared to intraligamental injections. Repeated IANBs were the least successful (Table 1).42
Injection technique(s)
Success rate (painless treatment)
IANB + ABI
84%
IANB + IO
68%
IANB + PDL
48%
Repeated IANB
32%
In supplementary buccal infiltrations, 4% articaine is more efficacious than 2% lidocaine.43,44 It is unclear whether the higher potency of articaine is related to its thiophene ring enhancing its liposolubility, or its use at higher concentrations.45
Intra-osseous injections after failed IANBs provide 90% successful pulpal anaesthesia lasting an hour for endodontic treatment and first molar extractions.46,47,48 However, the nature of intra-osseous injections may cause the entry of vasoconstrictor-containing solutions into the bloodstream; increased heart-rates have been reported as a result.49
Supplementary intraligamental injections may be useful for exodontia.50 Recently, it has been suggested that intraligamental injections alone can be used as a primary LA technique for non-surgical mandibular molar extractions.51 However, the duration of intraligamental LA is shorter than IANBs, potentially making it unsuitable for long-duration procedures.52
Considering that IANBs can be unpredictable in providing adequate anaesthesia, it is good practice to plan ahead and choose the most appropriate mode of LA to supplement the IANB for that procedure.
Safety of IANBs
Systemic complications
It is known that IANBs have the highest positive aspiration rate (10–15%) out of the LA techniques.7 Even after aspiration, intravascular injections may still occur.53 Adverse reactions are likely to happen as a consequence of high LA concentrations in plasma (Table 2).6,54
Toxic effects
Lidocaine toxicity at different serum concentrations
1–5 μg/ml:Tinnitus, light-headedness, diplopia, disorientation, mood alteration, patient may complain of nausea/vomiting
5–8 μg/ml:Slurred speech, localized muscle-twitching, small tremors, nystagmus
8–12 μg/ml:Focal seizures that may develop into generalized tonic clonic seizures. Respiratory depression/arrest may occur at higher concentrations (20–25 μg/ml); may result in cardiovascular arrest, coma
Methaemoglobinaemia
Relatively uncommon
Associated with:
Articaine
Benzocaine (topical): should be avoided
Prilocaine: not to be used for children under 6 months, patients using oxidizing drugs, pregnant women. Limit dose to 2.5 mg/kg
Low levels of methaemoglobinaemia (1–3%) = asymptomatic
Higher levels (10–40%) manifest as cyanosis, tachycardia, fatigue, breathlessness
Paraesthesia
Evidence suggests that it is more common with articaine and prilocaine
Local complications
Permanent damage to nerves, orofacial tissues and the eyes occur rarely,6 but awareness of their prevention is crucial.
The two nerves most likely to become injured by mandibular blocks are the inferior alveolar nerve and the lingual nerve (LN).55 Administering multiple IANBs can increase the likelihood of LN injuries. The incidence of permanent LA-induced nerve injuries is relatively rare (1:52,000); however, they have life-long impacts on patients. Patients may experience prolonged neuropathies with paraesthesia and allodynia; ‘chronic post-surgical pain’ may persist over the long term.6
Facial palsy has been reported after IANBs, associated with poor technique: injecting into the parotid region through which the facial nerve traverses, if the needle penetrates deeper, towards the mandible's posterior margin.56
Ocular complications occur rarely; incidences of diplopia, amaurosis and reduced visual acuity (due to optic-nerve atrophy) have been reported.57
Prevention and management
Optimizing IANB technique or replacing IANBs with infiltrations can reduce the risk of these complications.6
‘Blind injections' are taught in dentistry. Dental students are not taught to use nerve-imaging techniques to administer blocks, contrary to other healthcare professions.6 A review of 39 studies using ultrasound-guided nerve blocks concluded that they were effective at reducing the rate of nerve injuries and intravascular injections.58 However, this review did not include intra-oral blocks. Despite there being studies that look at the effectiveness of ultrasound-guided nerve blocks in dentistry, more research should be done to evaluate their effect on patient safety.
Reassurance of the patient by the clinician is vital in the management of LA-induced nerve injuries. Medical interventions, such as vitamin B, NSAIDs, and steroids can be implemented; however, these treatments are not yet evidence-based.6
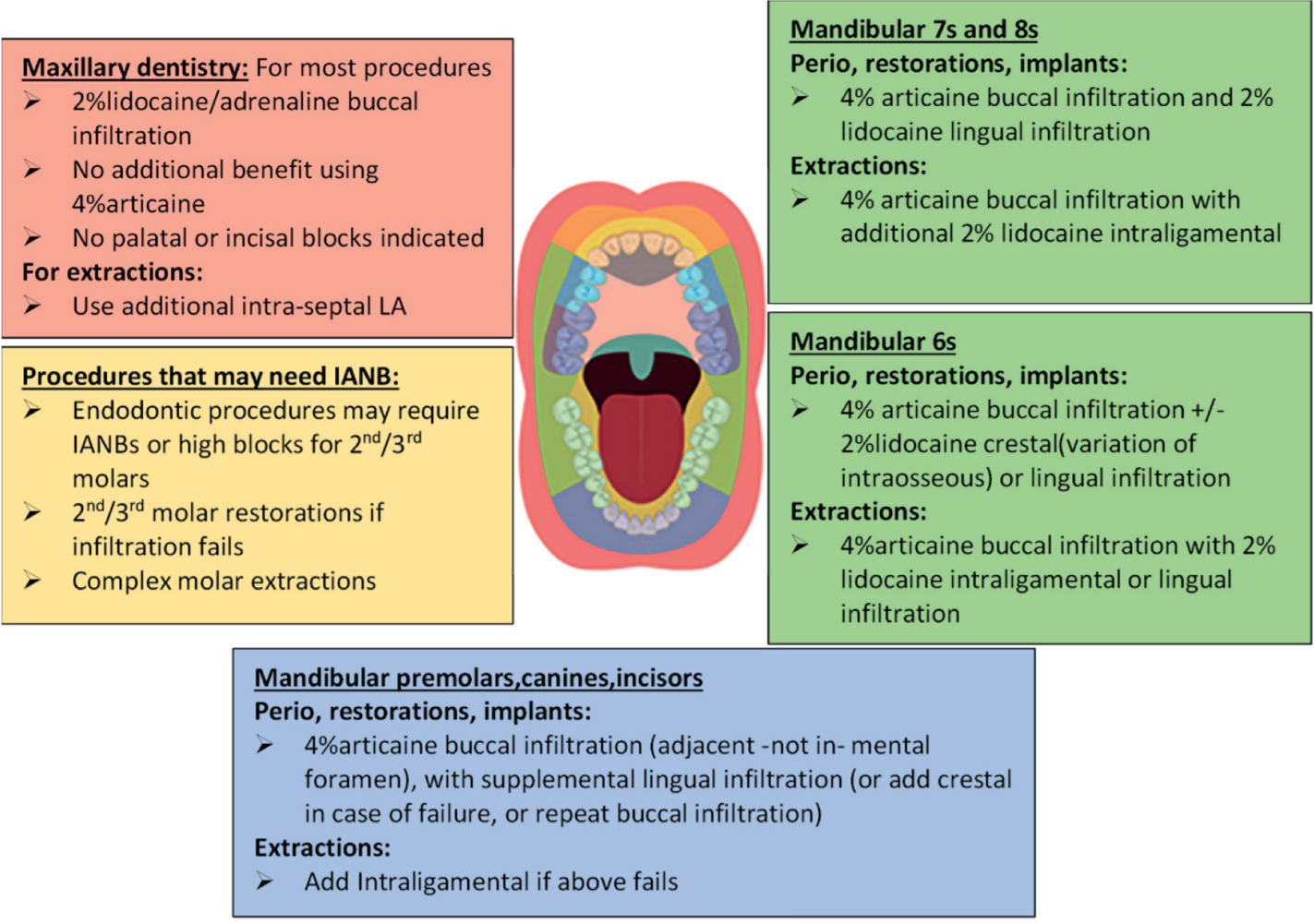
Optimizing LA: ‘smart’ tailored technique
‘Smart’ LA practice can optimize anaesthesia, where the LA solution, volume, concentration and technique are tailored to the site, procedure and patient (recommendations presented in Figure 4).22 Unnecessary use of IANBs should be avoided where infiltrations are safer and more effective. Evidence supports supplementing or replacing IANBs with mandibular infiltrations:23,59,60
The efficacy of buccal infiltrations using 4% articaine (1:100,000 adrenaline) is similar to IANBs with the same formulation or with 2% lidocaine (1:80,000 adrenaline) in first mandibular molars. The onset of pulpal anaesthesia with buccal infiltrations is significantly faster than IANBs.10,59
Buccal infiltrations can be used as an alternative to nerve blocks in pulpitic mandibular molars61 or supplemental techniques should be used.62
Articaine infiltrations are successful for restorative dentistry in paediatric patients, without needing IANBs; they decrease the duration of soft-tissue anaesthesia, hence reducing the risk of self-injury.63,64
In the mandibular incisor region, where the failure rate of IANBs is highest,21 authors advocate combining labial and lingual infiltrations, with a 92% success rate.65,66 The authors have concluded that splitting the LA dose labially and lingually is more effective than one infiltration.
In patients with haemophilia, infiltrations are more likely to be indicated rather than IANBs, to reduce risk of haemorrhage.67
Figure 4. Smart tailored LA practice.22 (Figure courtesy of Andrew Mason, University of Dundee.)
Despite a lack of an adequate evidence base for LA in implant dentistry, optimal LA practice using infiltrations has been taking place in this field for over 30 years. The use of mandibular infiltrations in implantology is both efficacious and safe.6,68
Patients experience much less discomfort and pain during infiltrations compared to IANBs. The full lingual sensation and shorter duration of anaesthesia post-operatively (from infiltrations) is favoured by patients.22
Conclusion
Optimal patient care necessitates optimal LA. This involves evidence-based ‘smart’ practice, where the operator tailors the LA solution, volume, concentration, and technique to the procedure, site, and patient.
Owing to the unpredictable nature of IANBs, clinicians may consider using pre-operative anti-inflammatory drugs (for endodontic patients) and/or supplemental LA to enhance anaesthesia. IANB success is often overestimated, and there is an abundance of evidence to support the transition from IANBs to infiltration dentistry in most procedures. This will improve LA safety and efficacy. Awareness of preventing adverse reactions and LA-associated complications is paramount.
Indeed, it may be difficult for dentists who routinely use IANBs to change their current practice. This does not mean that optimal LA practice is impossible. Changing practice will take time, but the final outcome will significantly enhance patient care.