Le Doare K, Hullah E, Challacombe S Fifteen-minute consultation: a structured approach to the management of recurrent oral ulceration in a child. Arch Dis Child. 2014; 99:82-86
Porter SR, Leao JC. Review article: oral ulcers and its relevance to systemic disorders. Aliment Pharmacol Ther. 2005; 21:295-306
Crighton AJ. Oral medicine in children. Br Dent J. 2017; 223:706-712
Porter SR, Hegarty AM, Kaliakatsou F, Hodgson TA, Scully C. Recurrent aphthous stomatitis. Clin Dermatol. 2000; 18:569-578
Sircus W, Church R, Kelleher J. Recurrent aphthous ulceration of the mouth; a study of the natural history, aetiology, and treatment. Q J Med. 1957; 26:235-249
Field A, Longman L. Tyldesley's Oral Medicine.Oxford: Oxford University Press; 2007
Bagan JV, Sanchis JM, Milan MA Recurrent aphthous stomatitis: a study of the clinical characteristics of lesions in 93 cases. J Oral Pathol Med. 1991; 20:395-397
Wray D, Rees SR, Gibson J, Forsyth A. The role of allergy in oral mucosal diseases. QJM. 2000; 93:507-511
White A, Nunes C, Escudier M Improvement in orofacial granulomatosis on a cinnamon- and benzoate-free diet. Inflamm Bowel Dis. 2006; 12:508-514
Patel M, Davis G, John R, Cowie R. Orofacial Granulomatosis in children – a review. Dent Update. 2019; 46:42-48
Healy CM, Thornhill MH. An association between recurrent oro-genital ulceration and nonsteroidal anti-inflammatory drugs. J Oral Pathol Med. 1995; 24:46-48
Carew O'Donnell S, Marshman Z, Zaitoun H. ‘Surviving the sting’: the use of solicited diaries in children and young people with oral mucosal disease. Int J Paediatr Dent. 2013; 33:352-358
Shim YJ, Choi JH, Ahn HJ, Kwon JS. Effect of sodium lauryl sulfate on recurrent aphthous stomatitis: a randomized controlled clinical trial. Oral Dis. 2012; 18:655-660
Wong SS, Yip CC, Lau SK Human enterovirus 71 and hand, foot and mouth disease. Epidemiol Infect. 2010; 138:1071-1089
Hviid A, Rubin S, Muhlemann K. Mumps. Lancet. 2008; 371:932-944
Davis N, McGuire B, Mahon J The increasing incidence of mumps orchitis: a comprehensive review. BJU Int. 2010; 105:1060-1065
Orenstein W, Perry R, Halsey N. The clinical significance of measles: a review. J Infect Dis. 2004; 189:S4-S16
Progress towards global control and regional elimination, 1998–1999. Wkly Epidemiol Rec. 1999; 74:429-434
El-Hajj Aoun N, Toum S. Oral ulcer: an uncommon site in primary tuberculosis. Aust Dent J. 2015; 60:119-122
Lowy G. Sexually transmitted diseases in children. Pediatr Dermatol. 1992; 9:329-334
Gonul M, Ozge Keseroglu H. Pediatric pemphigus. Clin Pediatr Dermatol. 2015; 1:1-3
Gurcan H, Mabrouk d, Razzaque Ahmed, A. Management of pemphigus in paediatric patients. Minerva Pediatr. 2011; 63:279-291
Martinez-De Pablo M, Gonzalez-Ensenat M, Vicente A Childhood bullous pemphigoid, clinical and immunological findings in a series of 4 cases. Arch Dermatol. 2007; 143:215-220
Mendes F, Hissan-Elian A, Morgado de Abreu M, Goncalves V. Review: dermatitis herpetiformis. An Bras Dermatol. 2013; 88:594-599
Chaudhari S, Mobini N. Linear IgA bullous dermatosis, A rare clinicopathologic entity with and unusual presentation. J Clin Aesthet Dermatol. 2015; 8:43-46
Deviations from the normal appearance of pale, pink and healthy mucosa require close monitoring or intervention and may be a sign of an underlying systemic disorder. Therefore, it is important that there is timely identification of abnormalities, appropriate management in primary care and onward referral for investigation to specialist services when required. Oral ulceration is the most common soft tissue abnormality in children, with recurrent aphthous stomatitis being the most common type of ulceration. This article discusses the various causes of oral ulceration in addition to vesiculobullous conditions, which may affect the paediatric patient.
CPD/Clinical Relevance: It is important that GDPs are aware of the range of causes of ulcers and blisters presenting in children and are aware of when to refer.
Article
Oral ulceration is a common condition affecting the oral mucosa and can be described as a full-thickness loss of the epithelium.1 There are many causes of oral ulceration and both local factors and the presence of any underlying systemic conditions need to be considered to reach a working diagnosis. The most common causes of oral ulceration can be found in Table 1.2
Aetiology
Associated features
Initial investigation
Trauma
Physical – traumatic occlusion, dental appliances, factitious trauma Chemical
History of trauma
Recurrent aphthous stomatitis
Idiopathic, normal haematologyMultifactorial precipitating factors: Genetic predisposition, stress, trauma, hormonal factors, sensitivity to foods
Recurrent and healing completely between episodes
FBCHaematinics (B12, ferritin and folate levels)
Vitamin deficiencies
Low iron, B12 and folate
Lack of dietary intake, weight loss, skin and hair changes, pallor, tongue depapillation
Systemic features such as weight loss, lethargy, cycles of fever, myalgia, arthralgiaAbdominal pain, diarrhoea, blood or mucous in stools, tiredness and malaise
FBCHaematinicsESRCRPAutoantibodiesPathergy test of the skin (Behcet's)Coeliac screen: anti-gliadin, anti-endomysial, anti-casein antibodies, IgA anti-tissue transglutaminase antibodies
A structured and concise history is important when considering oral ulceration in the paediatric patient. The following points should be explored with both the child and parent:3
Questions about the ulcer/s: site, size, number, shape, pattern of episodes, frequency and duration of episodes if recurrent. Are there any ulcers elsewhere on the body? The age of first onset should be ascertained. Is there healing with scarring?
Symptoms and effect: are the ulcers painful? Is there any effect on daily activities, eg speech, eating and drinking, school, playing?
Associated factors: is there any link with foods, psychological stress, hormonal changes and menstrual cycles or habits? Are there any potential sources of trauma?
Medical history and medications: complete a full systems enquiry with a particular emphasis on symptoms of fever, temperature, swollen glands, sore throat, tiredness, joint aches and gastrointestinal symptoms, such as abdominal pain, altered bowel habits and weight loss.
Family history: is there any immediate family history of ulceration or systemic illness?
Causes of oral ulceration
Traumatic ulceration
Ulceration as a result of oral mucosal trauma is frequently reported in children. Similarly to adult patients, traumatic ulceration can be categorized into physical or chemical causes, with the former being the most common.4 Physical trauma is often caused by sharp teeth, mamelons, orthodontic wires or appliances, with the most common site of traumatic ulceration being the non-keratinized mucosa. Traumatic ulceration can often present following accidental biting of the tissues after local anaesthetic has been administered (Figure 1).5 Therefore, it is important to provide optimal post-operative instructions to the child and parent/carer.
Figure 1. Traumatic ulcer to lower lip caused by accidental biting following a procedure under local anaesthetic.
Factitious trauma is self-harm to the tissues by the patient themselves and can present due to behavioural disturbances (Figures 2 and 3).6 This is more commonly seen in children and adolescents with the lower lip and tongue being the most frequently affected sites. Because it can pose a clinical challenge to diagnose factitious ulceration, a structured approach to establishing the cause and effect relationship is advised. Factitious trauma may be a sign of underlying psychological stress, therefore if required, the dentist needs to liaise with the general medical practitioner (GMP) to ensure that a multi-disciplinary approach is adopted to assess the patient's wellbeing.5
Figure 2. Gingivitis artefacta presenting as significant recession of maxillary gingivae in a 5-year-old with a picking habit.Figure 3. Six months later, following control of the 5-year-old's picking habit.
Ulcers that are traumatic in origin are most likely to heal or have significant resolution within 10–14 days of the cause being removed or habit stopped. Any ulcer lasting longer than this time requires onward referral and investigation.
Recurrent aphthous stomatitis
Recurrent aphthous stomatitis (RAS) is the most common oral mucosal disease, affecting up to 40% of selected groups of children.7 It usually presents in childhood or adolescence with a peak age of 10–19, and is believed to have a genetic predisposition, with up to 40% of patients reporting a family history.8 However, no specific human leukocyte antigen (HLA) haplotype has yet been identified.7
Clinical features of RAS include recurrent bouts of shallow, painful ulcers that are usually round or oval in shape with a yellowish centre, surrounded by an erythematous border.9 A young child may describe the pain from the ulceration as toothache. There can be single or multiple ulcers at any episode. The defining feature of aphthous ulceration is that the ulcers are recurrent, present in intervals from a few days to months with ulcer-free periods depending on severity. There are three recognized forms of RAS: minor, major and herpetiform.10
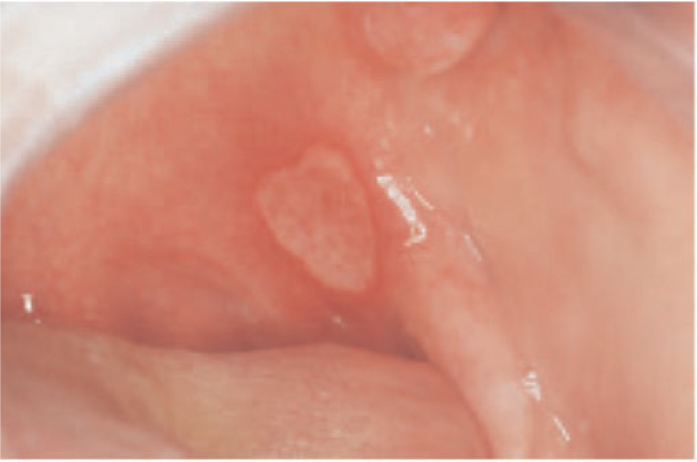
Minor RAS is the most common subtype representing 80% of children with RAS (Figures 4 and 5).7 It is characterized by its size being less than 10 mm across and affecting the non-keratinized mucosal surfaces. These heal in less than 14 days without scarring.11 Major RAS is less common and comprises much larger irregular ulcers, measuring over 10 mm across (Figures 6 and 7). They affect any part of the oral mucosa, including keratinized tissue, last up to 12 weeks and cause scarring.5 Finally, herpetiform RAS presents as multiple small ulcers (1–2 mm), which can coalesce to form irregular ulcers (Figures 8 and 9).11 Herpetiform ulcers are the least common in children, representing only 5–10% of those with RAS.12
Figure 4. Minor aphthous ulcer, upper right labial mucosa.Figure 5. Minor aphthous ulcer, left dorsal surface of the tongue.Figure 6. Major aphthous ulcer, left anterior pillar of the fauces.Figure 7. Major aphthous ulcer, right lateral border of the tongue.Figure 8. Herpetiform aphthous ulcer, lower left labial mucosaFigure 9. Herpetiform aphthous ulceration affecting the mucosa of the floor of mouth and the attached gingivae.
The aetiology of RAS is unclear and is believed to be multifactorial with a number of precipitating factors. For children, these include trauma, stress, hormonal factors and exposure to certain foods.12
Systemic disorders and ‘aphthous-like disease’
Most patients with RAS are otherwise healthy, thus it is a diagnosis of exclusion. There are, however, a number of systemic conditions involving recurrent aphthous ulceration and are, therefore, associated with RAS.11
First, in regard to haematological disorders, a deficiency of haematinics (iron, folate and vitamin B12) has been linked to recurrent ulceration,13 with up to 20% of RAS patients having some haematinic deficiency.11 RAS is also more common in patients with gastrointestinal (GI) disease. This may be primarily due to the GI condition or it may be secondary to haematological deficiencies caused by malabsorption or blood loss, especially in inflammatory bowel diseases, such as Crohn's disease (CD) and ulcerative colitis (UC). There is a well-recognized link between gluten-sensitive enteropathy (GSE, coeliac disease) and recurrent aphthae; however, fewer than 5% of patients initially presenting with RAS are diagnosed with GSE.14
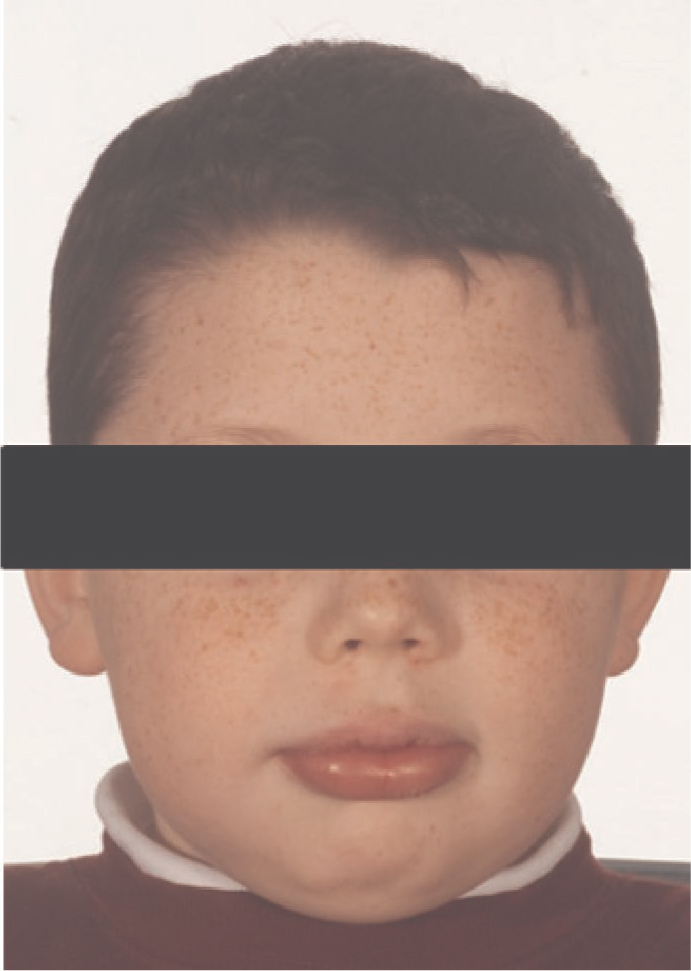
Orofacial granulomatosis (OFG) is a chronic inflammatory disorder of children and young adults characterized by recurrent or persistent swelling of the oral tissues, lips and face (Figures 10 and 11) with non-caseating granulomatous inflammation of the affected tissues.15 Patients may present with RAS-like lesions, but also persistent linear ulcers (non-RAS) at the base of hyperplastic tissue folds (Figure 12). Other clinical features include lip swelling and fissures, angular cheilitis, mucosal ‘cobblestone’ appearance and split-thickness gingivitis (Figure 13). The majority of OFG cases present as a single entity; however, in some cases there is an association with intestinal CD, sarcoidosis and Melkersson–Rosenthal syndrome.16 There is an increased prevalence of atopy in patients with OFG, and it has been linked to intolerance to certain foods, substances and additives, with cinnamon and benzoate compounds being the most common allergens.17
Figure 10. Lip swelling affecting a child with OFG.Figure 11. Facial and lip swelling in OFG.Figure 12. Linear ulceration in the depth of the right buccal sulcus seen in OFG.Figure 13. Cobblestone-like appearance of the right buccal mucosa seen in OFG.
Children suspected to have OFG should be referred to local oral medicine teams. While the patient is awaiting assessment, GDPs can support patients by ensuring that oral hygiene is optimal, advising completion of a diet diary and prescribing analgesia, for example 0.15% benzydamine hydrochloride (Difflam, Mylan, Hertfordshire, UK) spray or mouthwash as indicated, when required.
Management of OFG in secondary/tertiary care usually includes a dietary exclusion programme as the first line, which has been shown to improve disease activity.18 Topical corticosteroid preparations can be helpful to reduce lip inflammation and manage oral ulceration. For example, a 5-mg prednisolone tablet can be dissolved in 10 ml water and used as a rinse. Soluble betamethasone should be avoided as it contains benzoates (E211). A topical tacrolimus ointment on the lips and peri-oral skin and intra-lesional steroid injections (triamcinolone acetonide) into the lips can reduce inflammation. In some severe or unresponsive cases, short courses of oral prednisolone are sometimes required with systemic steroid sparing agents, such as azathioprine or infliximab, needed for chronic active OFG patients or patients with oral manifestations of CD.19
Other systemic conditions with aphthous ulcers include Behcet's disease, cyclic neutropenia and rarer syndromes such as MAGIC (mouth and genital ulcers with inflamed cartilage) and PFAPA (periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis).7 In addition, there can be aphthous ulceration in patients affected by HIV independent of necrotizing ulceration; however, this is very rare in children. Furthermore, certain medicines including non-steroidal anti-inflammatory drugs (NSAIDs) can cause RAS-like lesions.20
Investigations
Following history taking and examination, if the provisional diagnosis is RAS, a full blood count and haematinics screen (serum ferritin, serum B12, serum and red cell folate) is recommended to investigate any deficiencies or anaemia (Table 1).2 If an underlying systemic condition is suspected, onwards referral to an oral medicine or paediatric dentistry department is required.
Management of aphthous ulceration
The management of RAS and the aphthous ulcers of associated systemic conditions can be categorized as preventive, symptomatic and suppressive approaches (Table 2).
Preventive (Primary care)
Remove any source of trauma
Correct haematological deficiencies
Exclusion of any precipitating foods following ulcer diary
Symptomatic (Primary care)
SLS and flavour-free toothpastes (OraNurse)
To aid healing and prevent bacterial and fungal superinfection:
To help prevent an episode of ulceration, any source of trauma should be removed, for example, sharp teeth should be smoothed and orthodontic wires covered with wax. Haematological deficiencies should be corrected with the appropriate supplementation. An ulcer diary is a useful tool for the child and their parents to complete.21 This may highlight factors such as precipitating foods, which should be excluded from the diet.
Symptomatic
Toothpastes without sodium lauryl sulphate (SLS) may also help to reduce the pain associated with RAS.22 Mint and flavour-free toothpaste, such as OraNurse toothpaste (Welwyn, Hertfordshire, UK) can be recommended for those who are sensitive to mint.
Chlorhexidine gluconate mouthwashes (0.2%) can help prevent secondary bacterial infection and accelerate healing. This can be diluted to reduce any flavour and soreness.
Covering agents such as 0.2% hyaluronic acid (Gengigel, Dent-O-Care Ltd, London, UK) and Orabase (ConvaTec, Reading, UK) (active ingredient carmellose) can help to relieve symptoms. Gelclair (Helsinn, Switzerland), also containing hyaluronate, is an alternative covering agent.
Topical anaesthetic-containing sprays and mouthwashes to numb ulcer pain include:
- 0.15% benzydamine hydrochloride (Difflam) mouthwash is suitable from age 13 and over, the spray is recommended from 1 month and above;
- Lidocaine hydrochloride (Anbesol gel, Alliance Pharmaceuticals Limited, Wiltshire, UK) – age 12 and over, (Anbesol liquid) – for children from age 5 months;
- Benzocaine (Orajel, Church & Dwight, Canada) – for children aged 12 and over;
- Bonjela gel (Reckitt Benckiser Healthcare (UK) Ltd, Slough, UK) and Bonjela complete plus gel are contraindicated in children under the age of 16 due to the theoretical risk of Reye's syndrome because they contain salicylate salts. Bonjela junior gel contains lidocaine hydrochloride and cetylpyridinium chloride. It is suitable for children over the age of 5 months to relieve ulcer pain.
Suppressive
Many RAS patients can be treated in primary care, with the GMP supporting investigations. For some patients however, following referral to oral medicine clinics, suppressive treatment is required and topical corticosteroids are prescribed with their use closely monitored. There is a range of different topical steroids that can be used in a variety of preparations, including sprays or mouthwashes. It is important that, if topical steroids are used as a mouthwash, the child is able to rinse and spit the solution.5 A further topical adjunct that can be used as a mouthwash is doxycycline, which may aid healing. This should only be used for children over the age of 12 owing to the effects of tetracycline on the developing dentition. For severe non-responsive cases, systemic corticosteroids, such as a short course of oral prednisolone, may be required to control a flare up. Steroid-sparing immunosuppressant agents may be needed because long-term use of systemic corticosteroids can cause multiple complications, including stunted growth, elevated blood pressure and a reduction of bone density.
Management needs to be tailored to the specific child's needs and, at the time of writing, there is no evidence of a superior therapy.23 If an underlying systemic condition has been diagnosed, appropriate multidisciplinary care of the child is required via liaison between specialities and oral medicine. The treatment of the underlying condition will aid the management of the oral manifestations.
Viral infections
Herpes simplex virus
Many infections, mainly viral in origin (Table 3), can present with oral ulceration after the associated blisters break down, with herpes simplex 1 (HSV-1) being the most common precipitant. Ulcers caused by viral infection can present similarly to herpetiform RAS; however, they can be easily distinguished because they often do not recur, and are usually accompanied by systemic symptoms of fever and restlessness.
Clinical condition
Virus name
Virus type
Primary herpetic gingivostomatitisHerpes labialis
Herpes simplex virus 1
Human herpes virus (HHV) 1
Chicken poxShinglesRamsay–Hunt syndrome
Varicella-zoster virus
HHV3
Infectious mononucleosis
Epstein–Barr virus
HHV4
Oral ulceration in immunocompromised
Cytomegalovirus
HHV5
Kaposi sarcoma
Kaposi sarcoma-associated herpesvirus (KSHV)
HHV8
Hand foot and mouthHerpangina
Coxsackie A viruses
Picornavirus
Measles
Measles morbillivirus
Paramyxovirus
Mumps
Mumps orthorubulavirus
Paramyxovirus
Primary HSV-1 infection is mainly regarded as an infection of childhood with the majority of affected patients aged 6 months to 5 years.5 In most cases, infection with HSV-1 is subclinical, or can cause a mild pharyngitis. Others present with primary herpetic gingivostomatitis, which involves numerous small vesicles, affecting the oral mucosa and lips followed by ulceration (Figure 14). The gingivae are erythematous, and other clinical features include malaise, fever and lymphadenopathy.24 The oral lesions resolve after approximately 7–10 days, and management includes symptomatic relief with antipyretics/analgesics, rest and encouragement of fluid intake. Chlorhexidine gluconate mouthwashes and gels may reduce secondary infection, and some patients may require analgesic mouthwashes to reduce pain. Plain-ice popsicles or iced water may provide some relief. Antiviral medication is not usually required, but should be considered if the disease is severe, atypical25 or if the patient is immunocompromised.
Approximately 5% of patients previously infected by primary HSV-1 can develop recurrent herpes simplex infections whereby the virus is reactivated.4 Triggers for reactivation include stress, exposure to sunlight and an immunocompromised state.26 Recurrent HSV classically affects the mucocutaneous junction whereby vesicles rupture to form a crusted lesion, more commonly known as a cold sore. Recurrent HSV infections can also occasionally present intra-orally, usually affecting the hard palate or gingivae and are usually unilateral. Topical antiviral cream, for example 5% aciclovir, can be of benefit and has been shown to decrease the duration of lesion pain.27 Systemic antiviral treatment, eg aciclovir suspension is helpful for frequent episodes of recurrent HSV ulceration.
Varicella-zoster virus
Varicella-zoster virus (VZV) is another member of the herpes virus family. The primary viral infection causes chickenpox (varicella), which is a highly contagious disease, common in childhood. Skin lesions are characterized by maculopapular, pruritic lesions, which are followed by vesicles. Oral lesions are similar to those caused by HSV, and systemic symptoms are also present. Supportive treatment is all that is required for a child with chickenpox. Antiviral medications may be considered for immunocompromised patients.26 Reactivation of the virus presents as shingles (herpes zoster). Most patients with herpes zoster, however, are middle age or older, and therefore, it is less common in children. Initial symptoms include pain and tenderness along the distribution of the sensory nerve, and the trunk is the most common site to be affected. When the facial skin or oral mucosa is involved, the virus affects the peripheral branches of the trigeminal nerve and vesicular lesions erupt unilaterally. High-dose systemic antivirals are required and can accelerate healing,28 in addition to symptomatic treatment of any intra-oral lesions. Assessment by an ophthalmologist is required to assess any corneal scarring if the ophthalmic branch is involved.
Epstein–Barr virus
Epstein–Barr virus (EBV) plays a role in the aetiology of infectious mononucleosis (glandular fever), but is also linked to several malignancies, including nasopharyngeal carcinoma and lymphomas (non-Hodgkin and Burkitt's).
Most EBV infections in younger children are asymptomatic or associated with mild symptoms, whereas infectious mononucleosis tends to affect adolescents. Symptoms include fever, lymphadenopathy, pharyngitis and fatigue.29 Non-specific oral ulceration and palatal petechiae may also be present. The severity of symptoms can vary and the disease is usually self-limiting and supportive measures are sufficient.24
Coxsackievirus
Hand foot and mouth disease is caused by coxsackie A viruses, usually type 16 and enterovirus 71. It is highly contagious and tends to occur in mini-epidemics, typically in primary school children.30 Affected individuals display a macular rash with vesiculation on the palmar surfaces of the hands and the plantar surfaces of the feet, in addition to oral vesicles and ulceration. General malaise and discomfort accompanies the disease and the symptoms resolve after approximately 14 days. Isolation of children is required to avoid the spread of infection.
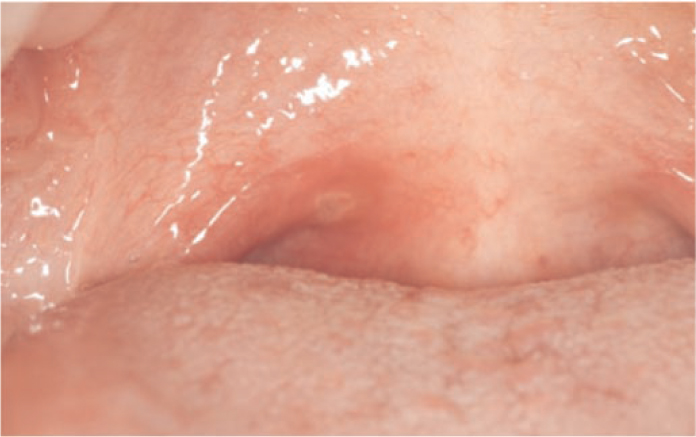
Herpangina is a further condition caused by coxsackie A viruses and predominately affects children. It is characterized by grey-white vesicular lesions that present on the posterior regions of the oral cavity, usually the soft palate, tonsillar or pharyngeal regions (Figure 15). The patient may also have mild to moderate malaise, headache or back pain. The condition is short-lived, lasting up to 1 week.
Figure 15. Vesicles, which break down to ulceration affecting the soft palate in herpangina.
Paramyxovirus
Paramyxoviruses include the mumps orthorubulavirus and also the morbillivirus that causes measles, both of which are transmitted via direct contact and droplet spread.
Mumps can occur at any age, but most commonly affects children. It is usually characterized by a prodromal illness of malaise and pyrexia followed by bilateral swellings of the parotid glands, with unilateral swellings occurring less frequently.31 The duct of the parotid salivary glands appear inflamed, with trismus and tenderness in the glandular region. Diagnosis is made on clinical presentation and the management is symptomatic and supportive in nature. Complications of infection with mumps virus can lead to encephalitis, pancreatitis, orchitis and oophoritis.32
Prior to vaccination, measles affected 95–98% of children under the age of 18.33 It usually affects infants and young children, and presents systemically with a fever and nasal discharge, followed by a maculopapular rash which lasts up to 7 days. Blue-white pinpoint spots on an erythematous base can appear on the buccal mucosa. These lesions, known as Koplik's spots, usually appear prior to the skin rash and resolve after 2–3 days. Management is symptomatic and supportive because the disease is self-limiting. There are, however, serious complications resulting from infection, including encephalitis and pneumonia.
The measles, mumps and rubella (MMR) vaccination is included in the World Health Organization's ‘Expanded programme on immunization’ and, since its introduction, there has been a significant reduction in the incidence of the diseases worldwide.34 Questions regarding the progress of the child's immunization programme should be asked as part of the medical history, with direction to the GMP if needed.
Bacterial infections
Tuberculosis is usually a pulmonary disease, but rarely there can be extra-pulmonary manifestations. Oral tuberculosis (TB) lesions are uncommon and usually present as a painless ulcer, due to secondary infection of the oral mucosa from pulmonary disease. Primary oral TB is extremely rare, but when present, it affects younger patients, and usually affects the gingivae or buccal sulcus accompanied by cervical lymphadenopathy.35
Syphilis is also a rare systemic bacterial cause of oral ulceration. Acquired primary syphilis can present with a chancre affecting the lips or tongue. It is particularly important from a paediatric safeguarding perspective because of the risks of transmission during sexual abuse.36
Vesiculobullous diseases
Pemphigus
Pemphigus is a rare group of autoimmune disorders caused by the development of autoantibodies, which target intra-epithelial or intercellular desmosomal complexes, leading to acanthylosis (loss of intercellular connections and separation of desmosomes, resulting in loss of cohesion between keratinocytes) and the formation of intra-epithelial bullae. Clinically this presents as blisters, followed by ulcers of the skin and mucous membranes, with the oral mucosa being the most frequently affected mucosal site.37 Pemphigus usually affects middle-aged patients and is extremely rare in children. Similarly to adults, pemphigus vulgaris is the most common type of vesiculobullous disease in the paediatric patient and childhood cases accounts for approximately 1.4–3.7% of total cases of pemphigus vulgaris.37 There is a significantly higher involvement of genital mucosa in children when compared to affected adults.38 Pemphigus can be life threatening and urgent referral for investigation is required. Immunosuppression with steroids or steroid-sparing agents is the mainstay of treatment.
Pemphigoid
Pemphigoid is another group of autoimmune vesiculobullous conditions causing blistering of the mucocutaneous surfaces. However, unlike in pemphigus, the autoantibodies target proteins in the basement membrane, thus causing subepithelial bullae. Again this condition is rare in childhood because it is normally seen in elderly patients. Specialist investigation and steroid treatment is required with steroid-sparing immunosuppression being important in the longer term.39
Dermatitis herpetiformis
Dermatitis herpetiformis presents with pruritic rashes and blisters affecting the skin of young adults and occasionally children. It is a subepidermal autoimmune disease that is strongly associated with gluten hypersensitivity because most patients have some abnormality of the jejunal mucosa.40 Oral manifestations are uncommon, but can include erythematous areas or erosions, affecting the oral mucosa. A gluten exclusion diet should be part of patient management. Diaminodiphenyl sulfone (dapsone) is a sulphonamide antibacterial medication. It acts as an anti-inflammatory drug and is a valid therapeutic option.
Chronic bullous dermatosis of childhood
This is another rare immune sub-epidermal blistering disease and is on the spectrum between pemphigoid and dermatitis herpetiformis. At the electron microscopic level there is linear deposition of IgA autoantibodies seen at the basement membrane zone. This results in linear IgA disease in adults and chronic bullous dermatosis of children.41 It usually presents in pre-school children (average onset at age 5 years), there are skin and oral vesicles/bullae, or ulcers, and there can sometimes be scarring. Most patients respond to corticosteroids or dapsone.
Erythema multiforme
Erythema multiforme (EM) is an acute-onset disease, which is variable in its clinical features. It can present with mucosal (including oral) vesicles and bullae leading to ulceration and circumoral haemorrhagic crusting. Skin lesions include erythematous maculopapular rashes and a classical target lesion, especially on extremities. EM usually affects young adults with approximately 20% of cases affecting children.42 It is thought that EM is a hypersensitivity reaction to infective agents, particularly herpes viruses, drugs (eg sulphonamides, anticonvulsants, such as phenytoin, and rarely anti-pyretic analgesics have been reported), in addition to food containing benzoates. Diagnosis is usually made clinically and treatment is mainly symptomatic, antivirals (if the suspected aetiology is viral) and topical and systemic corticosteroids may be helpful.43
Epidermolysis bullosa
This is a rare genetic group of blistering mucocutaneous conditions that are characterized by exacerbated skin and or mucosal fragility. It is caused by a mutation in genes coding for keratins in basal epithelial cells, collagens or other attachment proteins in the basement membrane. Over 30 subtypes have been reported, ranging in severity. The most severe forms can have variable survival of birth because of the severe sloughing of skin during passage through the birth canal and only those with milder forms survive to adulthood. Skin bullae form at birth or shortly afterwards owing to friction/mechanical trauma, or they can arise spontaneously. Peripheral limbs and pressure points are the most common sites affected, leading to scarring and limb deformity.44 Intra-oral bullae, which rupture resulting in painful erosions, may occur in babies when feeding and simple toothbrushing can present a challenge. Patients often develop multiple carious teeth because of their soft and high calorific diet, added to the difficulties with mechanical cleaning of plaque.45 A comprehensive and enhanced oral health preventive programme is essential. Special precautions and a multidisciplinary approach to complete dental treatment should be adopted, in addition to genetic counselling.
Conclusion
Primary care practitioners play a crucial role in the recognition of oral mucosal pathology in paediatric patients. It is appropriate for them to provide simple topical and supportive measures supported by referral to the appropriate specialist services when required.