Tan ECK, Lexomboon D, Sandborgh-Englund G Medications that cause dry mouth as an adverse effect in older people: a systematic review and metaanalysis. J Am Geriatr Soc. 2018; 66:76-84 https://doi.org/10.1111/jgs.15151
Riley P, Glenny AM, Hua F, Worthington HV. Pharmacological interventions for preventing dry mouth and salivary gland dysfunction following radiotherapy. Cochrane Database Syst Rev. 2017; 7 https://doi.org/10.1002/14651858.CD012744
Percival RS, Challacombe SJ, Marsh PD. Flow rates of resting whole and stimulated parotid saliva in relation to age and gender. J Dent Res. 1994; 73:1416-1420 https://doi.org/10.1177/00220345940730080401
Affoo RH, Foley N, Garrick R Meta-analysis of salivary flow rates in young and older adults. J Am Geriatr Soc. 2015; 63:2142-2151 https://doi.org/10.1111/jgs.13652
Gupta A, Epstein JB, Sroussi H. Hyposalivation in elderly patients. J Can Dent Assoc. 2006; 72:841-846
Åstrøm AN, Lie SA, Ekback G Self-reported dry mouth among ageing people: a longitudinal, cross-national study. Eur J Oral Sci. 2019; 127:130-138 https://doi.org/10.1111/eos.12601
Price EJ, Rauz S, Tappuni AR The British Society for Rheumatology guideline for the management of adults with primary Sjögren's Syndrome. Rheumatology (Oxford). 2017; 56:1643-1647 https://doi.org/10.1093/rheumatology/kex163
Bartoloni E, Baldini C, Schillaci G Cardiovascular disease risk burden in primary Sjögren's syndrome: results of a population-based multicentre cohort study. J Intern Med. 2015; 278:185-192 https://doi.org/10.1111/joim.12346
Ramos-Casals M, Brito-Zerón P, Bombardieri S EULAR recommendations for the management of Sjögren's syndrome with topical and systemic therapies. Ann Rheum Dis. 2020; 79:3-18 https://doi.org/10.1136/annrheumdis-2019-216114
Shiboski CH, Shiboski SC, Seror R 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren's syndrome: a consensus and data-driven methodology involving three international patient cohorts. Ann Rheum Dis. 2017; 76:9-16 https://doi.org/10.1136/annrheumdis-2016-210571
Osailan S, Pramanik R, Shirodaria S, Challacombe SJ, Proctor GB. Investigating the relationship between hyposalivation and mucosal wetness. Oral Dis. 2011; 17:109-114 https://doi.org/10.1111/j.1601-0825.2010.01715.x
Jousse-Joulin S, Gatineau F, Baldini C Weight of salivary gland ultrasonography compared to other items of the 2016 ACR/EULAR classification criteria for primary Sjögren's syndrome. J Intern Med. 2020; 287:180-188 https://doi.org/10.1111/joim.12992
Dry mouth has numerous causes, including medications, radiotherapy and rheumatological conditions, such as Sjögren's syndrome. This article presents the common causes of dry mouth, and details the assessment, investigations and management required for patients with dry mouth within primary dental care, in addition to outlining secondary care investigations and management.
CPD/Clinical Relevance: Dry mouth is common in the general population, with widespread implications for dental health and patients' quality of life. Dental professionals have a key role in both its identification and long-term management.
Article
Dry mouth is a common presentation in the dental clinic, requiring thorough assessment and management, both for short-term comfort and long-term disease monitoring and prevention of secondary consequential disease. The causes of dry mouth may be local, systemic or idiopathic; however, irrespective of the underlying cause, maintenance of oral health and prevention of dental disease should underpin management within primary care. Loss of the oral cleansing, antimicrobial, lubricating and buffering capacity of saliva can cause a multitude of problems, including increased susceptibility to dental caries, periodontal disease, mucosal trauma and oral candidosis. Patients may report a deleterious impact on their quality of life, reporting oral discomfort or burning, impaired eating and difficulties with speech.
This article reviews the common causes of dry mouth, the relevant investigations and possible treatment options available.
Subjective xerostomia
The perceived sensation of dry mouth in the context of normal unstimulated and stimulated salivary flow rates is referred to as subjective xerostomia. Changes in the qualitative nature of saliva may contribute towards these symptoms, as can mouth breathing. Subjective xerostomia may also occur as part of conditions such as oral dysaesthesia and burning mouth syndrome. Symptomatic management of dry mouth symptoms may contribute towards an overall improvement in the patient's dysaesthetic symptoms.
Objective xerostomia
Objective xerostomia describes dry mouth in the context of an objective reduction in salivary flow. This may be the result of medications, age-related changes, radiotherapy, or as part of a systemic condition, such as Sjögren's syndrome.
Aetiology
Medications
Many over-the-counter and prescribed medications can cause dry mouth symptoms. These are typically drugs with anticholinergic properties, including commonly prescribed antihypertensives, antihistamines, antidepressants, antipsychotics and reflux medications (Table 1).1 In many instances, it is not clinically feasible or appropriate to switch the patient's medications, and the alternative drugs may also have dry mouth side-effects. This is particularly the case for antidepressant and antipsychotic medications. Moreover, it is often the cumulative burden of polypharmacy that contributes to dry mouth signs and symptoms rather than one specific drug.
Indication for medication
Class of medication
Examples
Hypertension
ACE inhibitors
RamiprilEnalaprilPerindopril
Thiazide diuretics
Bendroflumethiazide
Hypertension, heart failure
Loop diuretics
Furosemide
Urinary frequency, urgency, incontinence
Antimuscarinic
OxybutyninTolterodine
Depression, anxiety
Selective serotonin reuptake inhibitors
FluoxetineCitalopramSertraline
Monoamine oxidase inhibitors
Phenelzine
Depression, neuropathic pain
Tricyclic antidepressants
Amitriptyline
Psychosis, schizophrenia
Antipsychotics
QuetiapineAripiprazole
Allergies/allergic rhinitis
Antihistamines
Cetirizine
Reflux, gastrointestinal ulceration
Proton pump inhibitors
OmeprazoleLansoprazole
Chemotherapy and radiotherapy
Many chemotherapy drugs can cause transient dry mouth symptoms that improve after cessation of treatment. In contrast, head and neck radiotherapy causes long-term acinar loss within the salivary gland architecture, resulting in qualitative and quantitative changes to the saliva.2 The majority of patients will experience dry mouth symptoms due to radiotherapy, with considerable deleterious impact on quality of life.
Gender and ageing
Women have lower unstimulated and stimulated salivary flow rates than men, and this is related to smaller salivary gland size.3,4 There are contrasting reports of the effect of ageing on saliva production in the literature. Some authorities have shown that ageing causes a significant reduction in the volume of unstimulated whole saliva, with preservation of stimulated salivary flow.3 A large meta-analysis found gland-specific reduction in salivary flow, with significant reduction in unstimulated and stimulated salivary flow from the submandibular and sublingual glands in older people.5 Other authorities contend that reduced salivary flow among older individuals is the secondary effect of polypharmacy, systemic disease or radiotherapy, with no significant change in saliva production in healthy older individuals.6 From a clinical perspective, self-reported xerostomia is also a useful metric, with older adults significantly more likely to report xerostomia, particularly if they are taking regular prescribed medications.7
Diabetes
Diabetes mellitus can cause salivary gland dysfunction and hypofunction, resulting in xerostomia.8 Sialosis (non-inflammatory enlargement of the major salivary glands) may be observed in patients with suboptimal glycaemic control. The combination of xerostomia, hyperglycaemia and the relative immunosuppression of diabetes can result in oral candidosis, and may be a presenting feature of undiagnosed diabetes.
Rheumatological
Sjögren's syndrome, a systemic autoimmune condition, has an incidence of 3.9–5.3 cases per 100,000 of the population.9 It may occur in isolation (traditionally referred to as primary Sjögren's syndrome), or may arise in individuals with a pre-existing systemic autoimmune condition, such as rheumatoid arthritis or systemic lupus erythematosus (traditionally referred to as secondary Sjögren's syndrome). The majority of patients are diagnosed in the sixth and seventh decades of life, with women significantly more likely to be affected than men, with female:male ratios of 9:1 reported in the literature.9 Lymphocytic infiltration of the exocrine glands, such as the salivary glands and lacrimal glands results in xerostomia and xerophthalmia, respectively. However, Sjögren's syndrome is a systemic condition and other common extra-glandular features include: inflammatory arthritis, Raynaud's syndrome, fatigue, interstitial lung disease and peripheral neuropathy.10 Less common extra-glandular features include renal and liver involvement.10 In common with other rheumatological conditions, patients with Sjögren's syndrome also have a significantly increased risk of cardiovascular disease compared with the general population.11
Owing to the progressive nature of Sjögren's syndrome, where gland function slowly reduces over time, patients may not present oral symptoms in the earlier onset phases of the condition. They may instead report non-glandular symptoms, or even symptoms of mucosa-associated lymphoid tissue lymphoma (MALT). Patients with Sjögren's syndrome are at significantly increased risk of MALT lymphoma, a type of low-grade non-Hodgkin's lymphoma.12
Diagnosis of Sjögren's syndrome requires holistic patient assessment and in the UK, is currently guided by the 2016 guidelines published by the American College of Rheumatology/European League Against Rheumatism Classification group for primary Sjögren's (Table 2).13
Item
Weight/score
Labial salivary gland with focal lymphocytic sialadenitis and focus score ≥1
3
Anti-SSA (Ro) +
3
Ocular staining score ≥5 (or van Bijsterfeld score ≥4) on at least one eye
1
Schirmer ≤5 mm/5 min on at least one eye
1
Unstimulated whole saliva flow rate ≤0.1 ml/min
1
Items within the assessment receive a weighting score, and a score of 4 or more is indicative of Sjögren's syndrome. The two items with the highest weighting are positive anti-SSA (Ro) and positive labial salivary gland biopsy. Anti-SSA is an autoantibody of the extractable nuclear antigen (ENA) family and is assessed using a blood test. ENA antibodies also include anti-SSB (La), which is commonly detected in patients with Sjögren's syndrome, and antibodies associated with conditions such as systemic lupus erythematosus, systemic sclerosis and mixed connective tissue disease.
Labial salivary gland biopsy can be of particular diagnostic benefit where there are clinical signs of Sjögren's syndrome, but immunology (anti-SSA and anti-SSB) is negative. Although not included in the diagnostic criteria, ultrasound assessment of the major salivary glands can assist diagnosis of Sjögren's syndrome, in addition to providing ongoing monitoring for lymphomatous change.
Management of Sjögren's syndrome can be viewed as either symptomatic therapy or disease controlling. Symptomatic treatment comprises use of salivary replacement and saliva stimulating products, while disease controlling therapies include systemic medications such as hydroxychloroquine (see later).
Clinical features of xerostomia
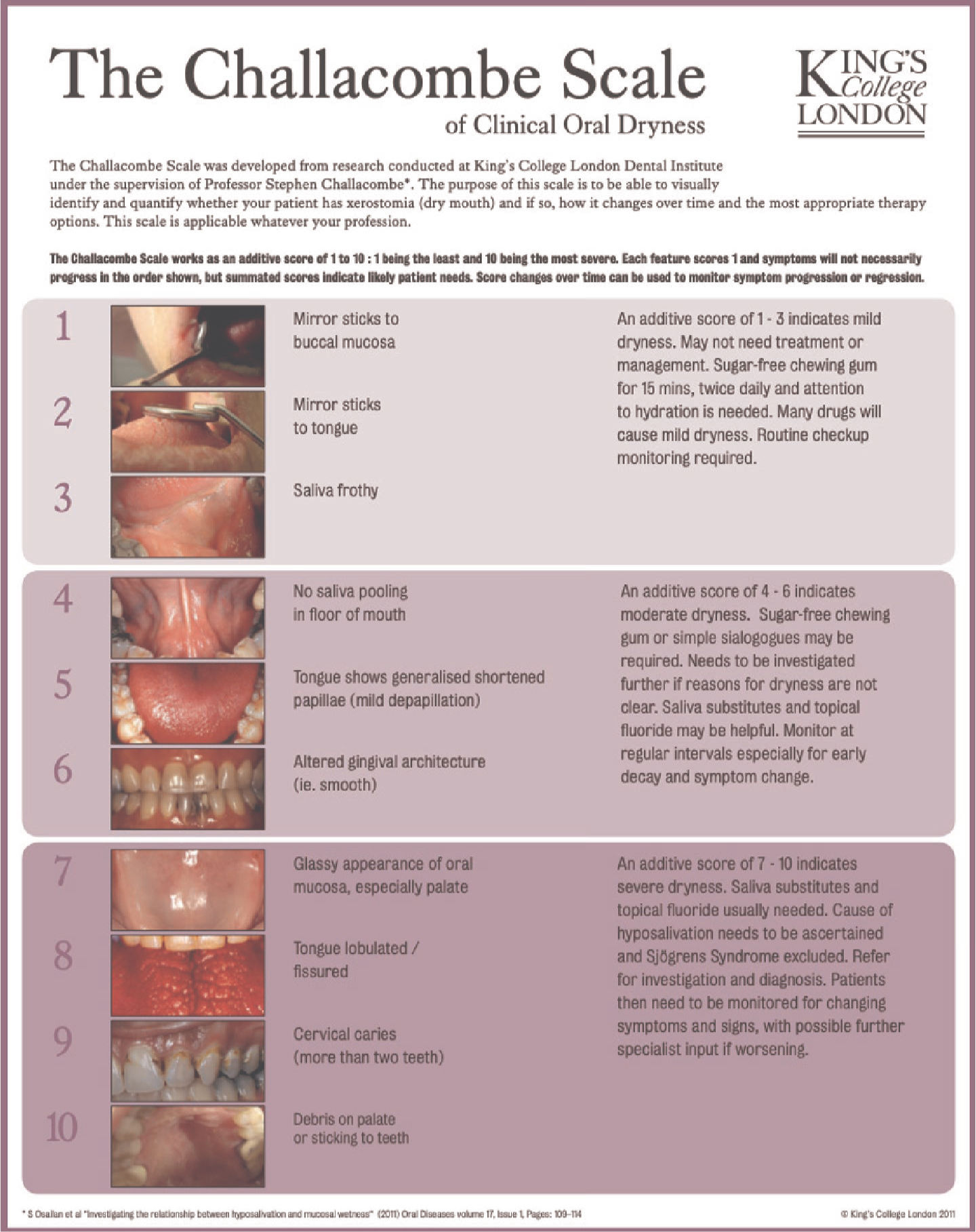
The clinical features of xerostomia are variable (Table 3) and, in some instances, may be subtle and easily missed when viewed in isolation (Figure 1). However, a holistic assessment of oral dryness can be performed using the Challacombe dry mouth scale (Figure 2).14
Clinical signs of xerostomia
Dry oral mucosa
Reduced saliva pooling
Frothy saliva
Depapillation of the tongue
Tongue fissuring
Cervical caries
Debris remnants
Glassy appearance of oral mucosa
Figure 1. Mild fissuring of the tongue in a patient with xerostomia secondary to Sjögren's syndrome.Figure 2. Challacombe dry mouth scale. This poster can be downloaded from: https://fgdpscotland.org.uk/wp-content/uploads/2018/09/Challacombe-Scale-oral-dryness-ENG.pdf
The Challacombe scale is a pictorial guide that can be used by all dental care professionals to grade the severity of xerostomia. The additive score obtained out of 10 provides an objective assessment of the severity of xerostomia, which can guide treatment, assist with patient monitoring and management strategies over time. It represents one of the first attempts to create a clinician reported outcome measure (ClinROM) score to facilitate long-term monitoring of the impact of current and future therapies in a comparable fashion. The groupings were suggested by clinician-perceived severity, but any can occur in any cluster, and all are valid indicators of dryness and management need.
Investigations
Dental assessment
Given the important protective functions of saliva, any reduction in the presence of saliva increases the risk of dental caries and periodontal disease (Figure 3).
Figure 3. Effects of xerostomia on the oral mucosa and dental health of a patient with Sjögren's syndrome. (a) Shows the smooth, glassy appearance of the gingivae due to chronic oral dryness. (b) Shows multiple cervical restorations and evidence of periodontal disease in the same patient.
Patients known to have reduced salivary flow, therefore, require regular surveillance by the general dental practitioner, to detect early dental disease development or change. Bitewing radiographs for periodic assessment of the interproximal regions may be beneficial to detect dental caries. Serial periodontal assessments to detect plaque, calculus accumulation and gingival inflammation can help direct preventive periodontal interventions.
Salivary and lacrimal gland assessment
1Within a secondary care setting, formal assessment of salivary flow can be performed by either unstimulated salivary flow (USF) or stimulated parotid flow rate. USF is often considered unreliable, but is included in the ACR/EULAR Sjögren's classification.13 It is performed over a 10-minute period and a flow of <0.1 ml/min is considered to be a positive test, calculated either by volumetric or gravimetric means (Figure 4a).
Figure 4. Investigations performed for dry mouth symptoms in secondary care. (a) Universal container used to collect unstimulated saliva. The empty container is weighed and the patient is then asked to collect their saliva for 10 minutes by leaning forwards and allowing their saliva to passively drain into the container. The saliva-filled container is weighed again, facilitating calculation of the salivary flow rate. (b) Specialist filter paper for Schirmer test. The filter paper is applied adjacent to the medial canthus of the eye for 5 minutes. (c) Blood bottles for venepuncture.
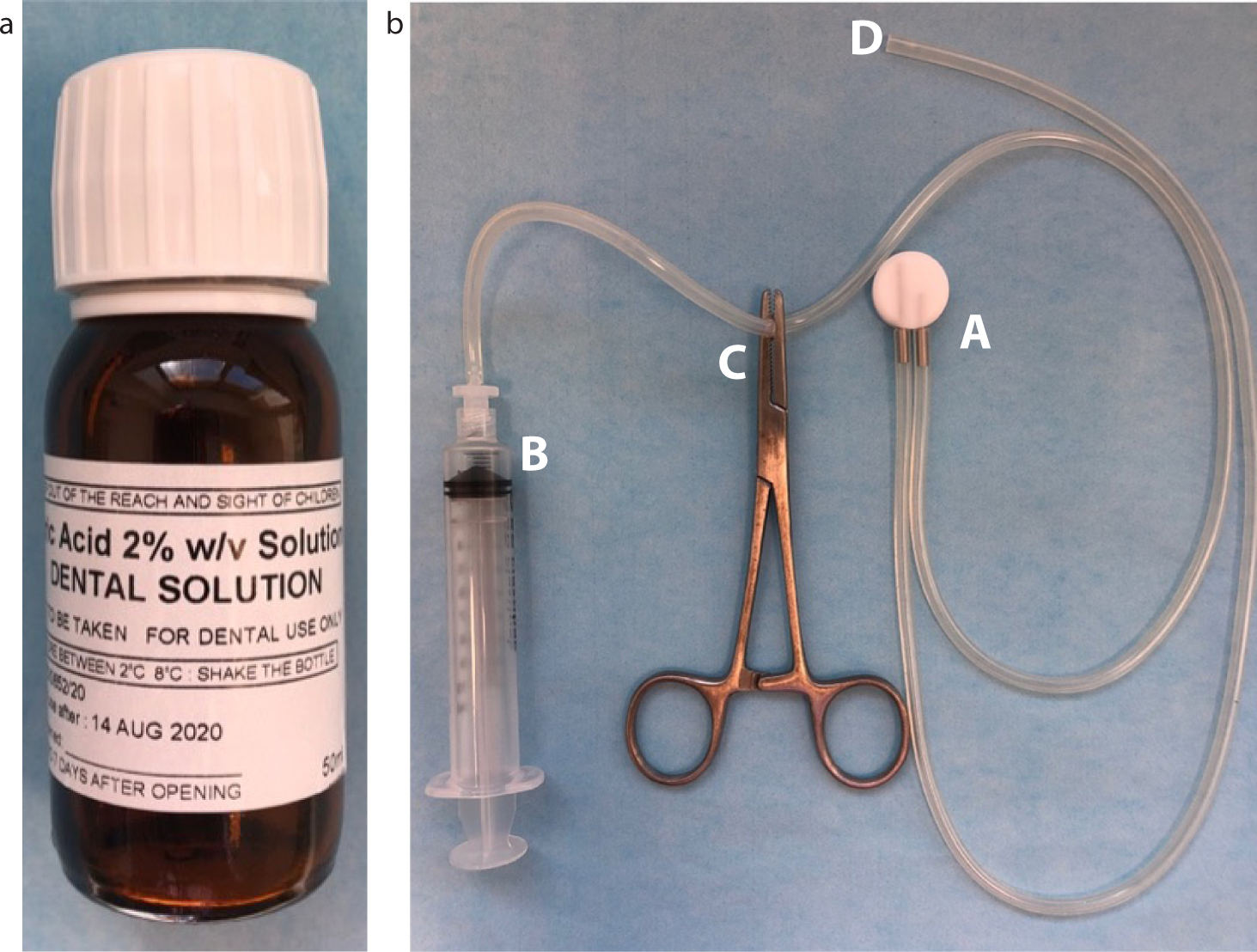
Stimulated parotid salivary flow is performed using a suction cup that is placed over the parotid duct opening (Figure 5). With the patient sitting upright and relaxed, a saliva stimulant (dilute citric acid solution) is dropped onto the tongue and saliva is collected over 10 minutes, and volumetrically or gravimetrically measured, yielding a simple mean flow rate in ml/minute. Schirmer's test is used to determine whether a patient produces enough tears to keep the eyes moist and, therefore, prevent corneal discomfort, pain or injury. This is performed over a 5-minute period using strips of specialist filter paper (Figure 4b). The distance the tears flow down the filter paper by passive capillary uptake is measured at 5 minutes. A moisture front rate of travel of <1 mm/min is considered a positive test.
Figure 5. Equipment required to collect stimulated saliva from the parotid gland. (a) 2% citric acid solution: 1–2 drops are applied to the tongue to stimulate saliva flow. (b) The suction cup A is applied to the parotid duct and suction is applied and maintained using the syringe B and forceps C. Saliva flows through the other arm of the tubing D and can be collected into a universal pot.
Bloods
Patients with dry mouth signs and/or symptoms will often undergo a range of blood tests within a secondary care setting (Figure 4c). These blood tests are particularly important for screening for Sjögren's syndrome (discussed previously).
Salivary Candida screening
Patients with reduced salivary flow are more susceptible to colonization with high levels of Candida albicans and related Candida species. Oral candidosis may be asymptomatic or cause symptoms, including oral discomfort, burning and bad taste. Whole saliva or an oral rinse can be sent for microbiological assessment in specialist centres. In general, whole saliva samples with <1000 cfu/ml (colony forming units/ml saliva) of Candida species are considered to represent ‘normal’ carriage levels, while >2000 cfu/ml is deemed to represent infection (oral candidosis), requiring treatment with antifungal medications.15 Those in the range 1000–2000 cfu/ml might be considered to have elevated carriage and are managed according to symptoms. Oral candidosis can be a recurrent issue for patients with dry mouth, and in specialist settings, patients are often prescribed regular, short courses of antifungal medicines (eg Nystatin oral suspension used during the first week of every month) to balance the need for prophylaxis against oral candidosis, while reducing the risk of drug resistance. Recurrent or resistant oral candidosis may also be the result of infection with organisms such as Candida glabrata and Candida dubliniensis, which can rapidly develop resistance to common azole antifungals, such as fluconazole.
Radiology
In patients with xerostomia routine assessment of major salivary glands can be performed with ultrasound or sialography. While obstruction of the major salivary glands secondary to a sialolith may be assessed using dental radiographs, such as occlusal films, ultrasound enables assessment of the architecture of the major salivary glands. Sialography can aid with assessing the functional aspects of the salivary glands, including salivary clearance, as well as reviewing the ductal system for strictures or obstructions. Anomalies detected using these modalities may prompt further magnetic resonance imaging (MRI) in specific cases.
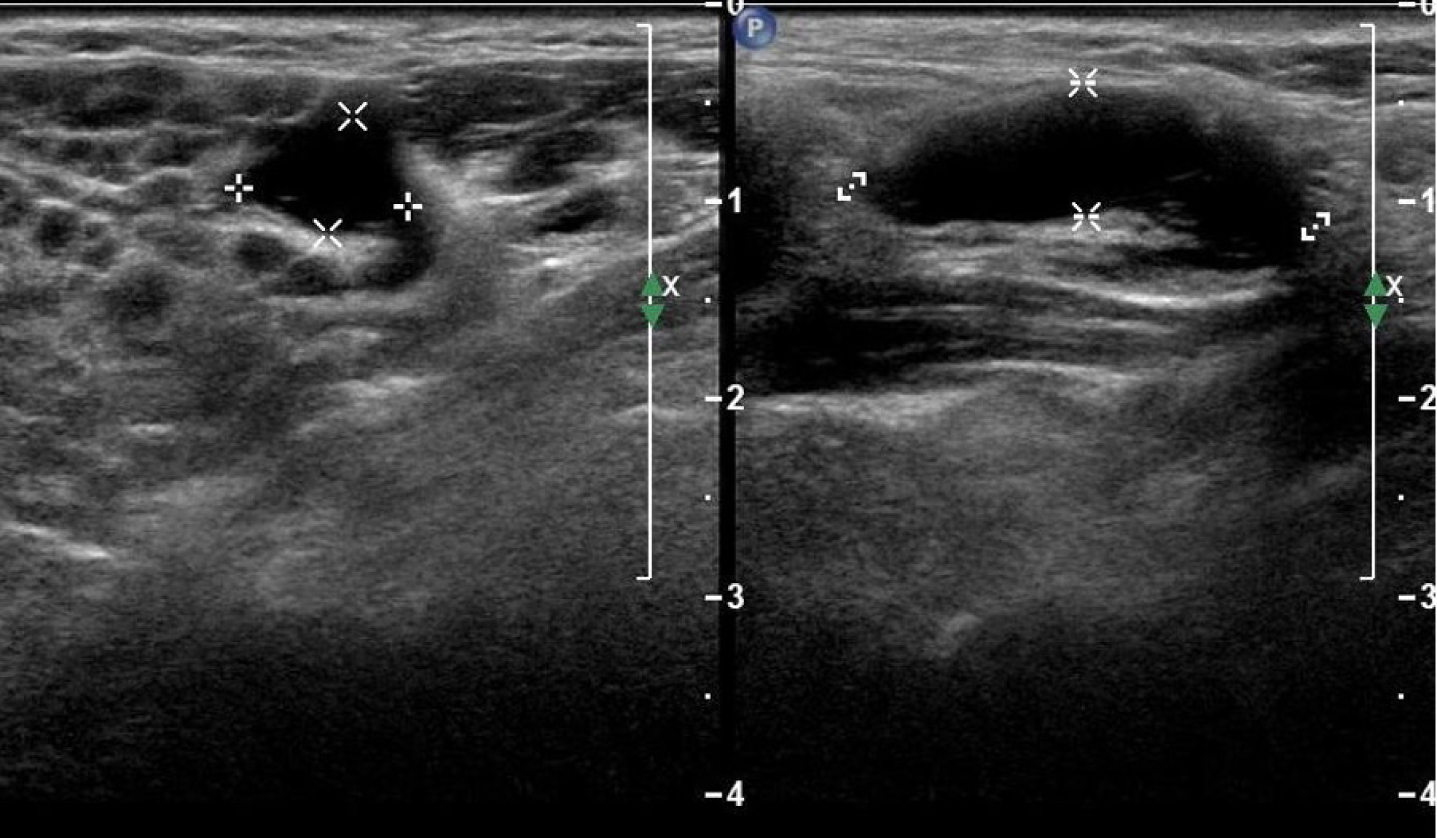
Ultrasound imaging of the salivary glands in Sjögren's syndrome (Figure 6) characteristically reveals focal and diffuse hypoechoic areas with non-homogeneous changes throughout the major salivary glands.16 Over time, the glands can become atrophic, but the majority of ultrasound screening in patients Sjögren's syndrome is for the detection of MALT lymphomas.
Figure 6. Ultrasound image of the parotid gland showing cystic areas consistent with Sjögren's syndrome.
Management
Dental prevention and patient education
Patients with xerostomia should be informed of their increased risk of dental disease, such as caries and periodontal disease. They should be supported to achieve a diet with low cariogenic potential, including avoidance of frequent ‘grazing’ throughout the day, and consumption of sugary foods prior to sleep. Patients who use mints and lozenges to alleviate dry mouth symptoms should be encouraged to use sugar-free preparations. The British Society for Rheumatology also recommends use of a xylitol-based sugar-free chewing gum for symptomatic relief in Sjögren's syndrome.10 Patients should also be encouraged to attend for regular examinations and receive comprehensive oral hygiene instruction.
The Delivering Better Oral Health (DBOH) toolkit (Public Health England and Department of Health) should be used to guide use of fluoridated products in primary dental care.17 In brief, adult patients with clinical features of dry mouth, or at high risk of dry mouth (eg Sjögren's syndrome), should be advised to use a daily fluoride mouthrinse (0.05% NaF) at a different time to brushing. Fluoride varnish (2.2% NaF) should be applied to the teeth twice yearly, and prescription of a high fluoride toothpaste (2800ppm or 5000ppm) should be considered for patients with active caries.
Symptomatic relief
A number of options are available for symptomatic relief of xerostomia. Success of these symptomatic treatments is highly variable. Topical replacement therapy in the form of salivary replacement gel and salivary replacement sprays can be beneficial for lubrication of the oral mucosa. Unfortunately, the duration of action of these replacements is limited, and patients often report dryness shortly after use. Gel-based salivary replacements tend to be more viscous and are, therefore, more beneficial during sleep. Lower viscosity salivary sprays can be more beneficial during periods of mastication and prolonged periods of speech. Salivary sprays with an acidic base should be avoided in the dentate to minimize iatrogenic tooth destruction
Pilocarpine
Pilocarpine, a muscarinic agonist, can assist with increasing volumes of saliva where some residual salivary gland function is still present. It is taken in tablet form (initially 5 mg) up to three times daily before being up-titrated to effect. A balance between the benefit versus the side-effects must be considered while commencing pilocarpine. Notable side-effects of pilocarpine include excessive sweating, increased respiratory mucous secretions, slowed heart rate, hypotension and gastrointestinal upset, therefore, giving it a challenging ‘excluded from use’ profile.
Systemic management of Sjögren's syndrome
Patients with Sjögren's syndrome should be under the care of a multidisciplinary team, including a rheumatologist, for overall coordination and management of this multi-system disease. Hydroxychloroquine, an antimalarial drug with anti-inflammatory properties is commonly used in the management of Sjögren's syndrome and associated conditions such as SLE, with some benefit reported for oral and ocular symptoms, in addition to fatigue, for some, but not all patients.10,12 Other immunomodulatory drugs, such as methotrexate, mycophenolate and rituximab are used for specific indications (Table 4).
Drug
Indication in Sjögren's syndrome
Dental relevance
Prednisolone
Flares of extra-glandular disease. Not recommended for long-term maintenance therapy
Increased susceptibility to infectionAdrenal suppression with long-term usePatients may require bisphosphonates for bone protection
Hydroxychloroquine
Commonly used for primary Sjögren's syndrome (particularly if concurrent joint involvement, fatigue or skin involvement)
N/A
Methotrexate
Concurrent inflammatory arthritis(Methotrexate is taken once per week, with folate supplementation on the other 6 days)
Oral ulceration (can be secondary to folate deficiency)Interaction with aspirin and NSAIDs (check British National Formulary)
Azathioprine
Not routinely usedMay be prescribed for management of lung involvement or cytopenias
Leukopenia (increased susceptibility to infection)Thrombocytopenia (increased bleeding tendency)
Mycophenolate mofetil
May be prescribed for management of lung involvement or cytopenias
LeukopeniaThrombocytopenia
Rituximab
Severe systemic involvement refractory to other systemic therapiesAlso used for management of lymphoma
B cell depletion leading to increased susceptibility to infection (liaise with patient's physician regarding timing of dental procedures)
Conclusion
Dry mouth can have a profound impact on a patient's oral health and quality of life. Dental practitioners should be aware of the common local and systemic causes of dry mouth, the indications for specialist referral and the importance of regular dental care to maintain oral health. This is particularly important in the current context, with disruptions to routine dentistry across the UK owing to COVID-19, and patient flow reduced due to infection control requirements. These changes have resulted in patients accessing dental care less readily or having urgent dental treatment needs that supersede concerns regarding dry mouth symptoms. Coupled with potential delays with secondary care referrals, the early recognition of dry mouth and implementation of preventive regimens in primary care is more important than ever.