Papaspyridakos P, Chen CJ, Gallucci GO Accuracy of implant impressions for partially and completely edentulous patients: a systematic review. Int J Oral Maxillofac Implants. 2014; 29:836-845 https://doi.org/10.11607/jomi.3625
Various methods exist for taking implant impressions. The open-tray or pick-up impression technique is one of the conventional methods for transferring the impression coping from the implant to the impression. In this method, a window directly above the implant is made in a stock or custom tray to allow access to the impression coping. Traditionally, the window is either left open, or closed with melted wax or foil. This technique tip describes a modification to create a stable and secure seal over the opening using rayon-based adhesive tapes. The benefits of this modification over the conventional open-tray technique are due to the enhanced adhesive quality of the materials to metal or plastic. Because there is less chance of impression material leaking from the tray window into the mouth, it is more comfortable for patients and less messy for clinicians. The benefit of this method over the closed-tray technique is the ability to feel for the head of the impression coping at the same time as making sure the impression material is in good contact with the underlying structures. It is easy to use, and efficient in terms of time and cost.
Article
The techniques for transferring information from the clinical scenario to the laboratory are based on commonly used conventional impressions and digital impression techniques. These can be grouped as follows:
Open closed tray;
Stock custom tray;
Digital scanning;
The open-tray technique uses an impression coping that is picked up with the impression, whereas the closed-tray technique relies on the clinician or technician to re-insert the impression coping back into the impression after it has been removed from the patient's mouth.1 The re-insertion of the coping, including any angulation factors on pick up, can produce errors in either the pick-up stage or during reseating. The open-tray impression technique has been shown in a systematic review to be more accurate than the closed-tray in all except partially edentulous patients (where there was no difference).2
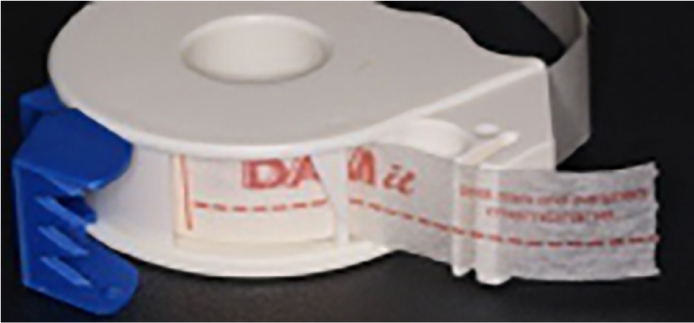
The standard open-tray impression technique involves sealing the tray opening with wax or using sticky wax to seal foil over the opening. As wax does not always adhere very well to tray material, a common problem is the wax coming away, causing extrusion of the impression material into the mouth. This new technique (Figures 1–9), however, uses a novel, yet simple, process of using a 100% non-woven rayon with a layer of acrylic adhesive tape DAM-it (Danville, California USA; Figure 10) or 3M medical tapes (3M, Minnesota, USA; Figure 11), which are latex free and hypoallergenic, to create a stable and secure seal over the opening. In the authors' opinion, owing to its adhesive quality on metal or plastic, it is simple to place. The adhesion is improved the firmer it is pressed against the tray material.
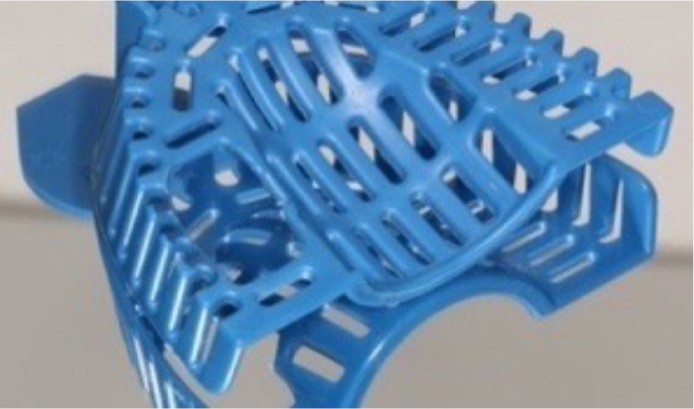
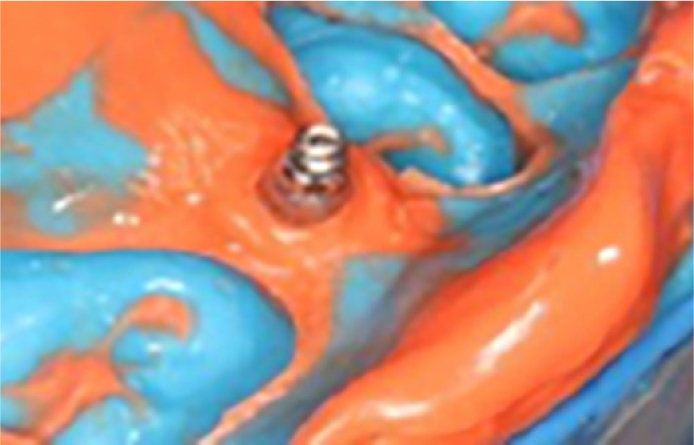
Figure 1. Implant healing abutment.Figure 2. Implant impression coping.Figure 3. Medium stock tray market, ready for adjustment.Figure 4. Custom open tray created using acrylic cutting bur.Figure 5. DAM-it adhesive tape placement.Figure 6. Putty and light-bodied silicone wash impression. Finger to push down material and locate head of impression coping.Figure 7. Locating the head of impression coping with a dental probe and removing set impression material.Figure 8. Final impression showing good occlusal and soft tissue detail.Figure 9. Final open-tray impression using stock plastic tray and pick up impression coping.Figure 10. DAM-it tape dispenser.Figure 11. 3M Micropore with dispenser.
Creating an effectively sealed opening prevents impression material being pushed out through the open access into the patient's mouth, especially on the upper impressions, making it much more comfortable for them. It also maintains a positive downward pressure against the soft tissue, teeth and impression coping, so creating a better impression. It reduces the cost because less material is needed and there are fewer glove changes. It keeps the working environment clean and tidy.
DAM-it is an adhesive tape that was marketed for use in the post-dam area to stop impression material flowing beyond the posterior aspect of the impression tray (Figure 10). 3M medical tapes produce comparable results.
The tapes have very good adhesive qualities to metal, stock and custom acrylic trays. The advantages are that the tape rarely comes away during impression taking; and if it does displace or distort, due to pressure from putty or heavy body impression material, it can be easily repositioned onto the impression coping, teeth and soft tissue (Figure 6). In addition, the head of the impression coping can be easily felt for, and by pushing firmly, the impression coping can be pushed through the tape with a good seal around it. Alternatively, a probe can be used to make a tiny hole in the tape and remove the set impression material that would get lodged in the screw access hole. Wax can be used to cover over the screw access to the impression coping, although the benefit is questionable, and it is generally not needed.
Conclusion
This modified open-tray technique has been used for several years in my practice, where it has proven to be simple and efficient in terms of both time and cost. Importantly, patients find the technique more comfortable than the conventional open-tray technique, and clinicians find it helpful to be able to feel the impression coping through the closed window.