Al-Ghatam R, Jones TEM, Ireland AJ Structural outcomes in the cleft care UK study – dentofacial outcomes. Orthod Craniofac Res. 2015; 18:14-24
Smallridge J, Hall AJ, Chorbachi R 2015. Functional outcomes in the Cleft Care UK study – part 3: oral health and audiology. Orthod Craniofac Res. 2015; 18:25-35 https://doi.org/10.1111/ocr.12110
Grosen D, Chevrier C, Skytthe A A cohort study of recurrence patterns among more than 54,000 relatives of oral cleft cases in Denmark: support for the multifactorial threshold model of inheritance. J Med Genet. 2010; 47:162-168 https://doi.org/10.1136/jmg.2009.069385
Beaty TH, Ruczinski I, Murray JC Evidence for gene-environment interaction in a genome wide study of nonsyndromic cleft palate. Genet Epidemiol. 2011; 35:469-478 https://doi.org/10.1002/gepi.20595
Seelan RS, Mukhopadhyay P, Pisano MM, Greene RM. Developmental epigenetics of the murine secondary palate. ILAR J. 2012; 53:240-252 https://doi.org/10.1093/ilar.53.3-4.240
Davis JS, Ritchie HP. Classification of congenital clefts of the lip and palate: with a suggestion for recording these cases. JAMA. 1922; 79:1323-1327
McBride WA, McIntyre GT, Carroll K, Mossey PA. Subphenotyping and classification of orofacial clefts: Need for orofacial cleft subphenotyping calls for revised classification. Cleft Palate Craniofac J. 2016; 53:539-549 https://doi.org/10.1597/15-029
McBride WA, Mossey PA, McIntyre GT. Reliability, completeness and accuracy of cleft subphenotyping as recorded on the CLEFTSiS (Cleft Service in Scotland) electronic patient record. Surgeon. 2013; 11:313-318 https://doi.org/10.1016/j.surge.2013.05.003
Sandy J, Williams A, Mildinhall S The Clinical Standards Advisory Group (CSAG) Cleft Lip and Palate Study. Br J Orthod. 1998; 25:21-30 https://doi.org/10.1093/ortho/25.1.21
Shaw WC, Dahl E, Asher-McDade C A six-center international study of treatment outcome in patients with clefts of the lip and palate: part 5. General discussion and conclusions. Cleft Palate Craniofac J. 1992; 29:413-418 https://doi.org/10.1597/1545-1569_1992_029_0413_asciso_2.3.co_2
Ness AR, Wills AK, Mahmoud O Centre-level variation in treatment and outcomes and predictors of outcomes in 5-year-old children with non-syndromic unilateral cleft lip treated within a centralized service: the Cleft Care UK study. Part 6: summary and implications. Orthod Craniofac Res. 2017; 20:48-51 https://doi.org/10.1111/ocr.12188
Madahar A, Murray A, Orr R, Sandler PJ. The long and winding road – the journey of a cleft lip and palate patient part 1. Dent Update. 2013; 40:791–794-796–798 https://doi.org/10.12968/denu.2013.40.10.791
Worth V, Perry R, Ireland T Are people with an orofacial cleft at a higher risk of dental caries? A systematic review and meta-analysis. Br Dent J. 2017; 223:37-47 https://doi.org/10.1038/sj.bdj.2017.581
Veiga KA, Porto AN, Matos FZ Caries experience and periodontal status in children and adolescents with cleft lip and palate. Pediatr Dent. 2017; 39:139-144
Durhan MA, Topcuoglu N, Kulekci G Microbial profile and dental caries in cleft lip and palate babies between 0 and 3 years old. Cleft Palate Craniofac J. 2019; 56:349-356 https://doi.org/10.1177/1055665618776428
Perdikogianni H, Papaioannou W, Nakou M Periodontal and microbiological parameters in children and adolescents with cleft lip and/or palate. Int J Paediatr Dent. 2009; 19:455-67 https://doi.org/10.1111/j.1365-263X.2009.01020.x
Sundell AL, Marcusson A. A comparison of orofacial profiles in 5- and 10-year-old Swedish children with and without cleft lip and/or palate. Clin Oral Investig. 2019; 23:1341-1347 https://doi.org/10.1007/s00784-018-2562-3
Lehtonen V, Sándor GK, Ylikontiola LP Dental treatment need and dental general anesthetics among preschool-age children with cleft lip and palate in northern Finland. Eur J Oral Sci. 2015; 123:254-259 https://doi.org/10.1111/eos.12195
Cook AK, Kerins CA, Heppner CE. Dental impacts on health-related quality of life of children with orofacial clefts. Pediatr Dent. 2016; 38:218-223
Boloor V, Thomas B. Comparison of periodontal status among patients with cleft lip, cleft palate, and cleft lip along with a cleft in palate and alveolus. J Indian Soc Periodontol. 2010; 14:168-172 https://doi.org/10.4103/0972-124X.75911
Rodrigues R, Fernandes MH, Monteiro AB Oral hygiene of children with cleft lip and palate: efficacy of the cleft toothbrush. A designed add-on to regular toothbrushes. Int J Paediatr Dent. 2018; 29:213-220 https://doi.org/10.1111/ipd.12447
Pegelow M, Alqadi N, Karsten AL. The prevalence of various dental characteristics in the primary and mixed dentition in patients born with non-syndromic unilateral cleft lip with or without cleft palate. Eur J Orthod. 2012; 34:561-570 https://doi.org/10.1093/ejo/cjr074
Menezes C, de Arruda JA, Silva LV Nonsyndromic cleft lip and/or palate: a multicenter study of the dental anomalies involved. J Clin Exp Dent. 2018; 10:e746-e750 https://doi.org/10.4317/jced.54926
Germec Cakan D, Nur Yilmaz RB, Bulut FN, Aksoy A. Dental anomalies in different types of cleft lip and palate: Is there any relation?. J Craniofac Surg. 2018; 29:1316-1321 https://doi.org/10.1097/SCS.0000000000004359
Hunt O, Burden D, Hepper P, Johnston C. The psychosocial effects of cleft lip and palate: a systematic review. Eur J Orthod. 2005; 27:274-285 https://doi.org/10.1093/ejo/cji004
Hunt O, Burden D, Hepper P Parent reports of the psychosocial functioning of children with cleft lip and/or palate. Cleft Palate Craniofac J. 2007; 44:304-311 https://doi.org/10.1597/05-205
Lorot-Marchand A, Guerreschi P, Pellerin P Frequency and socio-psychological impact of taunting in school-age patients with cleft lip-palate surgical repair. Int J Pediatr Otorhinolaryngol. 2015; 79:1041-1048 https://doi.org/10.1016/j.ijporl.2015.04.024
Kramer FJ, Baethge C, Sinikovic B, Schliephake H. An analysis of quality of life in 130 families having small children with cleft lip/palate using the impact on family scale. Int J Oral Maxillofac Surg. 2007; 36:1146-1152 https://doi.org/10.1016/j.ijom.2007.06.009
Hunt O, Burden D, Hepper P, Johnston C. The psychosocial effects of cleft lip and palate: a systematic review. Eur J Orthod. 2005; 27:274-285 https://doi.org/10.1093/ejo/cji004
Antonarakis GS, Palaska PK, Herzog G. Caries prevalence in non-syndromic patients with cleft lip and/or palate: a meta-analysis. Caries Res. 2013; 47:406-413 https://doi.org/10.1159/000349911
Queiroz Herkrath AP, Herkrath FJ, Rebelo MA, Vettore MV. Measurement of health-related and oral health-related quality of life among individuals with nonsyndromic orofacial clefts: a systematic review and meta-analysis. Cleft Palate Craniofac J. 2015; 52:157-172 https://doi.org/10.1597/13-104
Silva MARD, Balderrama IF, Wobeto AP The impact of nonsyndromic cleft lip with or without cleft palate on oral health-related quality of life. J Appl Oral Sci. 2018; 26 https://doi.org/10.1590/1678-7757-2017-0145
Naros A, Brocks A, Kluba S Health-related quality of life in cleft lip and/or palate patients – a cross-sectional study from preschool age until adolescence. J Craniomaxillofac Surg. 2018; 46:1758-1763 https://doi.org/10.1016/j.jcms.2018.07.004
Stock NM, Sharratt ND, Heath J Falling through the gap: Dental treatment experiences of patients affected by cleft lip and/or palate. Br Dent J. 2018; 225:218-222 https://doi.org/10.1038/sj.bdj.2018.542
Cleft lip and palate in general dental practice: filling in the gaps Sharan Reddy Catherine Liu Mina Vaidyanathan Nabina Bhujel Dental Update 2024 48:7, 707-709.
Authors
SharanReddy
BDS, BSc (Hons), PgCert, MFDS (RCPS Glas)
Specialty Dentist in Paediatric Dentistry, Guy's and St Thomas' Hospital, London
Cleft lip and palate (CLP) is the most common of craniofacial anomalies in humans. CLP results from disruption of embryonic processes during orofacial development; while syndromic clefts may have clearer aetiology, non-syndromic clefts are heterogeneous in aetiology. It is important for GDPs to understand the classification of CLP and the structure of centralized cleft centres in order to communicate with cleft teams. This article aims to clarify the role of GDPs within cleft management and discusses challenges in maintaining oral health in this group of patients, including increased risk of dental caries and periodontal disease, dental anomalies and psychosocial considerations.
CPD/Clinical Relevance: The GDP should be responsible for maintaining good oral health for the patient with cleft lip and palate, focusing on prevention from a young age and restorative work if needed.
Article
Cleft lip and palate (CLP) is a common congenital anomaly with a wide spectrum of severity, from a simple soft tissue cleft to a bilateral complete cleft involving multiple structures. CLP can occur in isolation, or in association with other developmental anomalies or as part of a syndrome (syndromic CLP). The management of CLP requires integrated care from an extensive multidisciplinary team, which co-ordinates timely treatment for the patient from birth.1 CLP can have a significant Impact on the patient and their family, and it is important to ensure that all healthcare professionals involved can provide streamlined care to maximize efficiency, effectiveness and patient experience.
General dental practitioners (GDPs) play an important role in the management of CLP in primary care. While the specialized cleft teams in tertiary care plan and perform complex treatment in hospital, GDPs are heavily relied on to review the patients on a regular basis to optimize their oral health and communicate with the cleft teams. Since the centralization of UK cleft services, outcomes such as facial growth and speech have improved by up to 70%,2 yet oral health outcomes have not changed.3 This highlights the need for better integration of the GDP in care of patients with CLP.
This article aims to give an overview of the background of CLP, its management in tertiary care, and the role of the GDP.
Epidemiology
CLP is reported to occur in 1 in 600–700 live births in the UK,1 with cleft lip (CL) comprising 23.5%, cleft palate (CP) 44.9% and CLP 31.6% of these live births.4 However, the incidence of CP has significant geographical variation, between 1.3 and 25.3 per 10,000 live births worldwide,5 with the highest rates in British Columbia and the lowest in Nigeria. Incidence of CLP also varies by ethnicity as shown in Table 1.6
The majority of clefts are isolated (76.8%), and approximately 7.3% are associated with recognized syndromes while 15.9% occur with malformations in other systems, most commonly with congenital heart defects, deformations, hydrocephaly, urinary tract defects and polydactyly. Isolated CP is more frequent in females, with a female to male ratio of 2:1, but CLP is more frequent in males than in females, at the same ratio.5
Incidence of CLP
Ethnicity
1 in 500 live births
Asians and Native American groups
1 in 1000 live births
European-derived populations
1 in 2500 live births
African populations
Aetiology
CLP has a multifactorial aetiology with interplay of genetic and environmental risk factors.6 While some syndromic clefts often have a clear inheritance pattern, non-syndromic clefts show a complex heterogeneous aetiology. Orofacial clefting occurs as a result of atypical embryonic development between the fourth and tenth week in utero. Any disruption to these processes may result in CLP.
Genetic factors
There is strong evidence to show that a family history of CLP substantially increases the risk of a child being affected by CLP.5 Genetic counselling is often recommended when a family member or child is affected by CLP, to advise parents about whether the cleft is isolated or syndromic, and the risk of having another child with an orofacial cleft.
There are many syndromes and conditions that may present with a CLP as a feature, some of which are listed with their aetiological genetic factors in Table 2.
Syndrome
Associated gene(s)
Pierre Robin sequence
SOX9
22q11.2 deletion
Chromosome 22
Van der Woude
IRF6 (also implicated in CLP)
Treacher–Collins
TCOF1, POLR1C, POLR1D
Stickler
COL2A1, COL11A1, COL11A2, COL9A1, COL9A2, COL9A3
Environmental factors
More recently, environmental factors have been considered to play a significant role in the aetiology of CLP, although these mechanisms are not fully understood. Epigenetic processes, heritable phenotypic changes that occur due to the influence of external factors on gene expression, have been increasingly implicated in this.7
Certain environmental factors are recognized as having an adverse effect on orofacial development, and increase the risk of CLP, primarily through changes in maternal health (Table 3).
Genetic
Environmental
Family history of CLPAsian and Native American ethnicitySingle gene mutations (syndromic)
Maternal smokingMaternal alcohol abuseMaternal diabetesMaternal sodium valproate useMaternal folic acid deficiencyMaternal fever in first 8 weeks
Classification
The complexity and variation in CLP presentations has made universal acceptance of a single classification system difficult. The first attempt to develop a classification for clefts was by Davies and Ritchie in 1922.8 Subsequently, many other different classifications of CLP have been proposed and used historically, based on embryological principles, morphological features, or a combination of both.
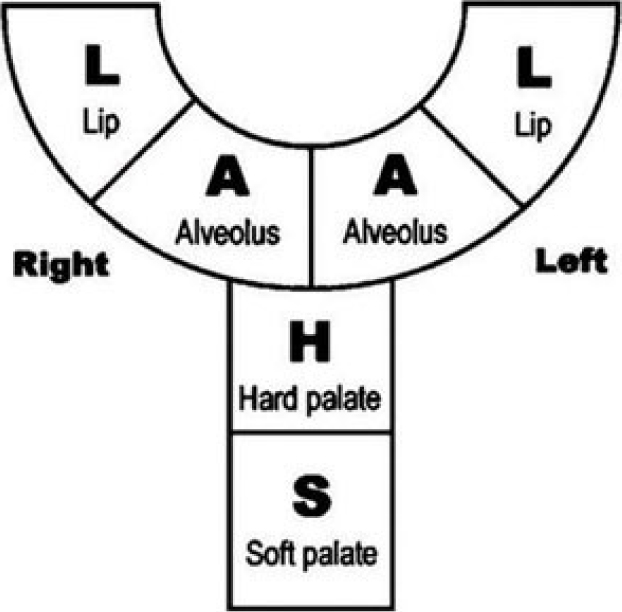
In the UK, the LAHSAL descriptive system of CLP classification is currently the most widely used, primarily for its simplicity and transferability to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD 10)9 and the Craniofacial Anomalies Register. LAHSAL has been shown to have a high degree of inter- and intra-observer reliability.10 The system was modified by the Royal College of Surgeons from Kriens' original ‘LAHSHAL’11 by omitting one ‘H’ from the acronym to give ‘LAHSAL’. The classification is divided into six parts:
Lip (right);
Alveolus (right);
Hard palate;
Soft palate;
Alveolus (left);
Lip (left).
In addition, an asterisk (*) is used to represent a microform lip, submucous cleft palate or a Simonart's band.
A capital letter in the LAHSAL classification indicates a complete cleft, whereas a small letter indicates an incomplete cleft. Any anatomical area that does not have a cleft is indicated with a full stop or a dash, for example: incomplete hard palate, complete soft palate defect and right incomplete cleft lip would be classified thus: ‘l . hS ..’ Figure 1 shows a diagrammatic representation of this classification.
Figure 1. Diagram of the LAHSAL classification.
Structure of the CLP team
The Clinical Standards Advisory Group (CSAG) report on cleft lip and palate, published in 1998, audited outcomes of non-syndromic unilateral cleft lip and palate (UCLP) patients aged 5 and 12 years old over a 15-month period. Of children aged 5 and 12 years old, 40% and 20%, respectively, had active caries requiring dental treatment, while 42% of 12-year-olds had seriously deficient or failed bone grafts. Dental arch relationships were ‘poor’ or ‘very poor’ in 37% of 5-year-olds and 39% of 12-year-olds and were likely to require further surgery to correct the skeletal discrepancy. A series of recommendations was made (Table 4).12 In 1992, prior to CSAG, a six-centre international study of treatment outcomes for UCLP patients concluded that key indicators for good patient outcomes involved standardization, centralization and high volume operators.13
A reduction of CLP teams from 57 to 8–15
Clarity on expertise and quality standards of each CLP team
Trust should review cleft care with a view to ensure a full range of clinical skills available
Agreement on a common database for all cleft patients
Training programmes for surgical training only in high-volume, high-quality CLP centres
Improved record keeping of cleft births in the UK
Following these recommendations, moves were made to centralize CLP care, which now has 11 managed clinical networks comprising 16 surgical sites that follow a multidisciplinary approach (Table 5). The investigations performed by the CSAG were repeated some 15 years later in a study known as Cleft Care UK. Reassuringly, it was found that there were marked improvements in some outcomes, such as dento-alveolar relationships and speech. However, and of great concern, was the finding that the percentage of children with caries experience (dmft > zero) had only reduced to 52% from 55%,14 highlighting an area in which the role of the primary care service holds significant importance.
Cleft surgeon
Paediatric anaesthetist
Specialist in paediatric dentistry
Consultant orthodontist
Specialist speech and language therapist
Consultant paediatrician
Consultant ENT (ear, nose and throat) surgeon and/or audiological physician/paediatric audiologist
Consultant/clinical nurse specialist (sometimes called a ‘cleft nurse’)
Clinical psychologist
Consultant restorative dentist
Consultant clinical geneticist
Dental reviews and interventions that involve the dentition are centred around orthodontics and paediatric dentistry in the CLP hub team; however, a significant component of care is delivered in primary care (Table 6). This highlights the need for shared care and the importance of clear communication between the various healthcare providers. Considering that the two main dental issues (dental caries and periodontal diseases) are wholly preventable, this should be a cause for a concerted and targeted effort to create and deliver interventions for this priority group.
Birth–8 weeks
9 weeks–2 years
3–7 years
8–4 years
15–20 years
>21 years returning
Orthodontics at hub
Assessment between 7 years and before 9 years by cleft team orthodontist, paediatric dentist and surgeon
Definitive orthodontic careAssessment for orthognathic surgery, if indicated
Orthodontic treatmentOrthognathic surgery
Paedodontics at hub
Paediatric dentist for dental health education/advice by 6 months and liaison with general dental care
Paediatric dentistry advice and/or intervention, if necessary
Paediatric dentistry and orthodontic treatment
Paediatric to restorative dentistry as indicated
With restorative dentistry
Primary care
Dental health education in liaison with main centre
Dental health education in liaison with main centre
Routine preventive dental advice and treatment
Routine preventive dental advice and treatment
Regular dental care
Regular dental care
Role of the GDP
The journey of a child born with a cleft is long and complex,15 yet the role of the GDP is critical because these patients have a higher risk of caries, periodontal disease and an increased incidence of dental anomalies. Children born with a cleft have a higher susceptibility to caries in both their deciduous and permanent dentition, so early detection and treatment is required.16 In the UK, advice from Public Health England and the British Society of Paediatric Dentistry's ‘Dental Check by One’ campaign is for all children to be seen by a dentist by 1 year of age, and ideally as soon as primary teeth erupt. Good communication and joint care between the GDP and CLP team gives the GDP the ability to more confidently deal with the complexities of care.
All CLP patients are encouraged to register with a GDP as soon as possible to start shared care early in the child's journey and to acclimatize the child to the dental setting. This, and preventive interventions, are key to dental care for those children born with a cleft. The majority of complex dental care is usually carried out by the CLP team; however, there may be a number of years in between dental assessments at the centre, and GDPs, along with orthodontic colleagues and MDT co-ordinators, are instrumental in maintaining the oral health of the child with CLP.
Advice for GDPs:
Encourage early registration of CLP patients by the age of 1 year;
Record details of CLP team, in particular the specialist(s) looking after their care;
Be alert to the holistic needs of the patient, and ensure appropriate referral to a range of dental specialists for orthodontics, complex restorative, implantology, periodontology, obturators and surgery (eg for fistula), as required;
Ensure good communication with CLP team to facilitate shared care;
Enhanced preventive advice, instruction and interventions.
Challenges of CLP management
High caries risk
There is good evidence that children born with clefting have a higher risk of caries.17,18 Some work suggests that the oral microbial profile of those born with a cleft may have an impact between the ages of 0 and 3 years;18 however, this may not be a factor in older children.19,20 The impact of high caries risk could increase the chances of these children requiring a general anaesthetic.21 Their dental treatment plans are often complicated by orthodontic needs along with further surgical treatments around the cleft site, such as alveolar bone grafting (Figure 2). This high caries risk is also more likely to be associated with a lower health-related quality of life (Figure 3).22
Figure 2. Localized caries around a cleft site.Figure 3. Gross caries in the primary dentition.
Advice for GDPs:
Management of all children born with clefts as higher caries risk;16
Check ups every 3–4 months with topical fluoride varnish (2.2% NaF);
Ensuring to follow radiography guidelines, all children with CLP should have radiographs as part of the cleft audit at the ages of 18 months, 5 years, 15 years and 20 years.
Periodontal diseases
Children born with a cleft often have poor oral hygiene19 and a corresponding high risk of gingivitis.17 The severity of periodontal disease may relate to the extent of the cleft and the involvement of the lip, alveolus and palate.23 It is important to note that periodontal diseases can also be localized, or more severe in teeth adjacent to the cleft area (Figure 4).19 Individualized oral hygiene instruction and equipment can be central to improving oral hygiene in CLP patients.24
Figure 4. Periodontal disease around a cleft site.
Advice for GDPs:
Oral hygiene instruction around CLP site;
Modified BPE scoring;
Ensuring reinforcement of oral hygiene during orthodontic treatment.
Malocclusion and dental anomalies
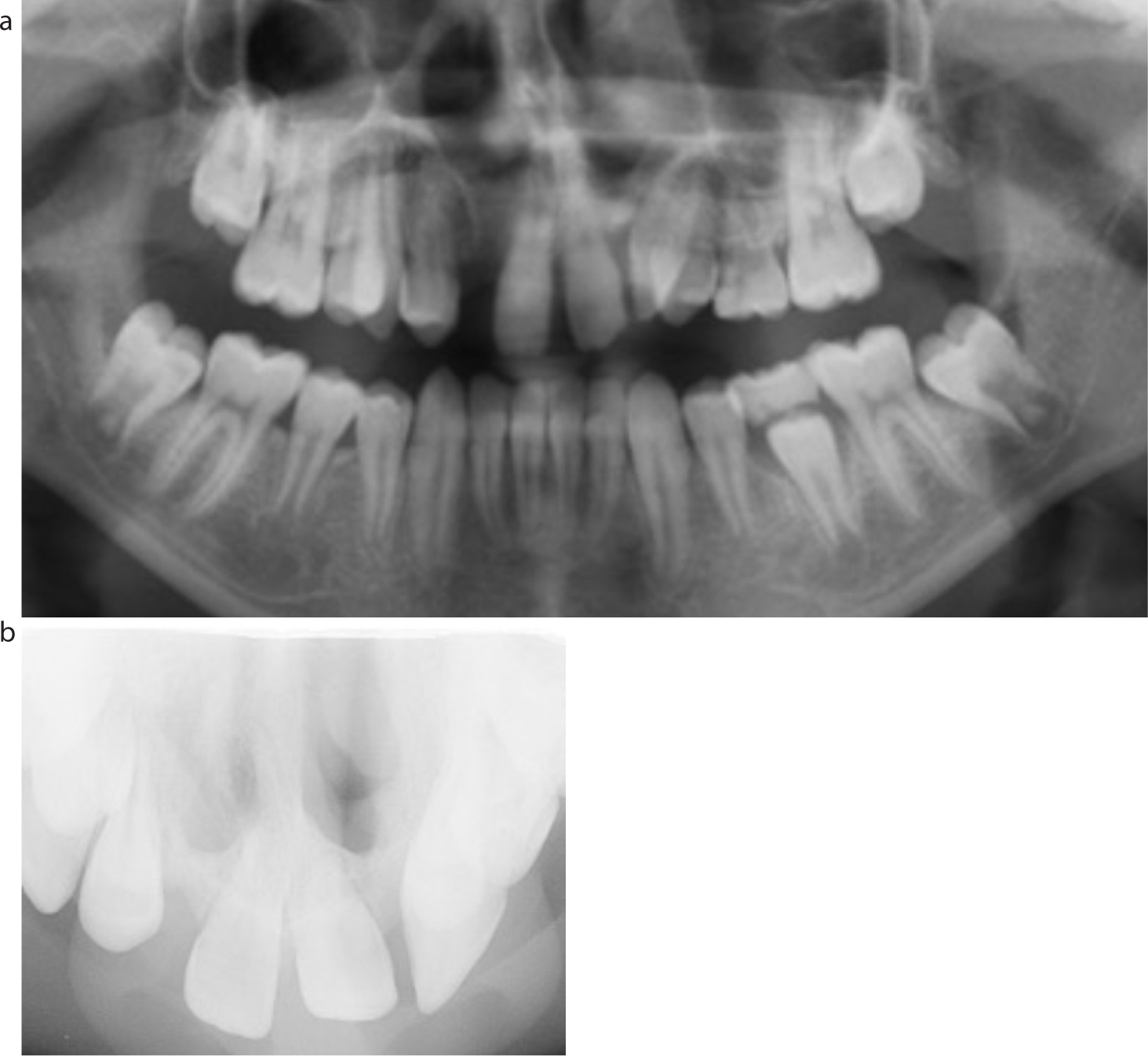
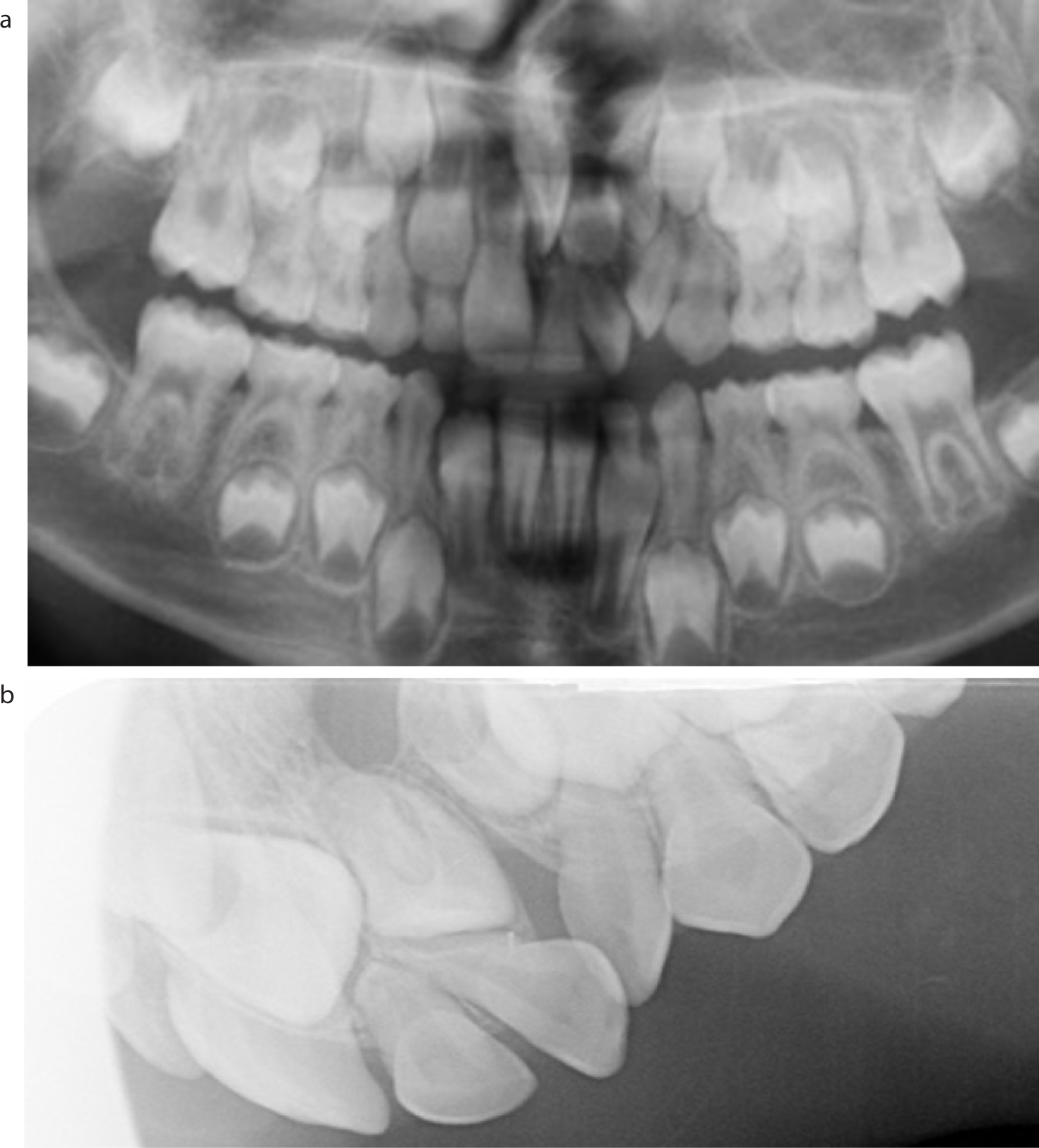
Many studies show that there is a high prevalence of dental anomalies, mostly surrounding the cleft site, affecting approximately 20–80% of those with CLP25,26,27 and there are significant differences from those in the non-cleft population.27 The most common dental anomalies seen in both syndromic and non-syndromic clefting include:
Figure 5. (a, b) Hypodontia caused by tooth agenesis of the UR2, UL2 and UL5.Figure 6. Double teeth caused by tooth gemination.Figure 7. (a, b) Ectopic eruption of UL1 adjacent to the cleft site, and multiple supernumeraries in the cleft site.Figure 8. Dens in dente in a cleft patient.Figure 9. Natal tooth associated with a cleft.
Due to these dental anomalies, close involvement with orthodontic and paediatric dentists is often essential in the care pathway.
Advice for GDPs:
Good medical history;
Consult with paediatric dentist or paediatrician if any specific concerns;
Closely monitor eruption of the developing dentition, and if concerned, discuss with paediatric dentist;
Be aware of any correspondence regarding the GDP's role in monitoring and managing conditions;
Encourage children born with a cleft to prioritize oral health and appreciate its benefits.
Diet
The type of cleft may often have an impact on a patient's diet. This is seen at an early age, with mothers given advice from birth to maintain good nutritional intake for the baby. Although CLP can create feeding difficulties, breastfeeding is often still possible, so parents should be advised against feeding on demand and through the night after the age of 1 year. Often specialist bottles and equipment are needed to ensure good intake, and with such challenges it is normal for parents to be focused on increasing calories and nutritional content, which may place the child at a higher caries risk.
Advice for GDPs:
Detailed diet history is important;
Early advice regarding diet, eg milk and water, avoid added sugars, warn regarding fruit juices;
Keep sugary foods to mealtimes;
Be aware of the textures of food and diet issues surrounding each patient.
Psychosocial impact
The impact of CLP undoubtedly extends more widely than oral health-related disease, and the effects on psychosocial functioning of these children is a field of research in its own right.
Although the majority of children and adults with CLP may not experience major psychosocial problems, specific issues can occur.28 Being teased about facial appearance is a significant predictor of psychosocial problems, such as anxiety, behavioural issues and negative self-perception.29,30 The impact of clefting can also influence family life, with increased social and personal demands.31
Several key issues arise from the literature:28,32
Behavioural problems;
Depression;
Anxiety
Dissatisfaction with facial appearance
Lower self-esteem
This reinforces the need for a multidisciplinary approach and emphasizes the importance of the psychologist in the CLP team.
Oral ill-health has been shown to be detrimental to overall quality of life.33 With regards to oral health-related quality of life (OHRQoL), children and adults with a cleft tend to score more poorly when compared to non-cleft populations,34,35 although patient and parent perceptions of OHRQoL differ significantly.29 Promisingly, the OHRQoL of some patients with a cleft improves due to the positive effect of CLP teams on self-esteem, communication skills and family interactions.36 However, only a small number of patients with CLP are accessing primary dental care services, in part due to a perceived lack of knowledge about CLP by GDPs, and also a lack of awareness of the services to which they are entitled.37
Advice for GDPs:
Draw on your regular interactions with the patient to build relationships with them and their family, understand their motivations and domestic circumstances;
CLP patients and families have frequent medical appointments, therefore discuss with parents convenient days/times for them to attend;
As the GDP, understand and relay patients' concerns to the CLP team;
Be aware of potential psychosocial consequences of having a cleft and the need for referral for psychological support, both through the cleft team and locally;
Enhanced prevention and 3-monthly recalls using motivational interviewing (or health coaching) techniques to encourage internal motivation for the self-management of their oral health;
Seek help from psychologists if there are more complex systemic factors preventing good oral health.
Conclusion
Children born with a cleft require multidisciplinary care from a multidisciplinary team, within which the GDP plays an important role. Considering the significant number of people affected by orofacial clefting, it is useful to understand the wide range of severities that may present, and the syndromes and other features that may be associated.
The GDP should be comfortable communicating with the centralized CLP team ‘hub’ to optimally co-ordinate the patient's care. While the specialized hubs perform complex treatments and surgical procedures to manage the clefting and its sequelae in the hospital setting, GDPs are pivotal in reviewing these patients regularly, and maintaining their oral health. As patients with clefts are at an increased risk of caries and periodontal pathology, especially around the cleft site, they require enhanced prevention and 3-monthly recalls. They may also present with challenging behaviour resulting from the psychosocial impact of CLP, which should be managed considerately.