Waste plastics in clinical environments: a multi-disciplinary challenge. https://tinyurl.com/kzzj6hsu (accessed July 2021)
Duane B, Stancliffe R, Miller FA Sustainability in dentistry: a multifaceted approach needed. J Dent Res. 2020; 99:998-1003 https://doi.org/10.1177/0022034520919391
Our Common Future.Oxford: Oxford University Press; 1987
NICE. Dental checks: intervals between oral health reviews. Clinical guideline CG19. 2004. http://www.nice.org.uk/guidance/cg19 (accessed July 2021)
Bauer N, Megyesi B, Halbac-Cotoara-Zamfir R, Halbac-Cotoara-Zamfir C. Attitudes and environmental citizenship. In: Hadjichambis AC, Reis P, Paraskeva-Hadjichambi D : Springer International Publishing; 2020
International Organization for Standardization. ISO 14040 – Environmental management – life cycle assessment – principles and framework. http://www.iso.org/standard/38498.html (accessed July 2021)
Hellweg S, Milà i Canals L. Emerging approaches, challenges and opportunities in life cycle assessment. Science. 2014; 344:1109-1113 https://doi.org/10.1126/science.1248361
Duane B, Ashley P, Saget S Incorporating sustainability into assessment of oral health interventions. Br Dent J. 2020; 229:310-314 https://doi.org/10.1038/s41415-020-1993-9
Duane B, Croasdale K, Ramasubbu D Environmental sustainability: measuring and embedding sustainable practice into the dental practice. Br Dent J. 2019; 226:891-896 https://doi.org/10.1038/s41415-019-0355-y
Fricton J, Chen H. Using teledentistry to improve access to dental care for the underserved. Dent Clin North Am. 2009; 53:537-548 https://doi.org/10.1016/j.cden.2009.03.005
Romano DM, Longson TD, Martin N. Minimal data set for remote clinical consultations in restorative dentistry - an exploratory case study. Eur J Prosthodont Restor Dent. 2020; 28:142-150 https://doi.org/10.1922/EJPRD_1972Romano09
Martin N, Shahrbaf S, Towers A Remote clinical consultations in restorative dentistry: a clinical service evaluation study. Br Dent J. 2020; 228:441-447 https://doi.org/10.1038/s41415-020-1328-x
Kraai IH, Luttik ML, de Jong RM Heart failure patients monitored with telemedicine: patient satisfaction, a review of the literature. J Card Fail. 2011; 17:684-690 https://doi.org/10.1016/j.cardfail.2011.03.009
Rizan C, Mortimer F, Stancliffe R, Bhutta MF. Plastics in healthcare: time for a re-evaluation. J R Soc Med. 2020; 113:49-53 https://doi.org/10.1177/0141076819890554
Duane B, Dixon J, Ambibola G, Aldana C, Couglan J, Henao D, Daniela T, Veiga N, Martin N, Darragh JH, Ramasubbu D, Perez F, Schwendicke F, Correia M, Quinteros M, Van Harten M, Paganelli C, Vos P, Moreno Lopez R, Field J. Embedding environmental sustainability within the modern dental curriculum – exploring current practice and developing a shared understanding. Eur J Dent Educ. 2020; https://doi.org/10.1111/eje.12631
Duane B, Steinbach I, Ramasubbu D Environmental sustainability and travel within the dental practice. Br Dent J. 2019; 226:525-530 https://doi.org/10.1038/s41415-019-0115-z
Sustainable oral healthcare and the environment: mitigation strategies Nicolas Martin Lucy Smith Steven Mulligan Dental Update 2024 48:7, 707-709.
Authors
NicolasMartin
BDS, PhD, PgCertEd, MFDSRCS, FDSRCS
Professor and Consultant in Restorative Dentistry, Academic Unit of Restorative Dentistry, School of Clinical Dentistry, Claremont Crescent, The University of Sheffield, S10 2TA, UK
Carbon emissions and single-use plastics (SUPs) are the main forms of environmental pollution relating to waste arising from oral healthcare. Ownership of this problem is shared with the whole supply chain, from manufacturing to distribution, procurement, clinical use and finally, waste management. Mitigation strategies focus on the individual stakeholders in the supply chain, including the provision of clinical care. Key to this is establishing a baseline analysis of the nature and the size of the problem through life cycle assessments (LCAs). Reduction of CO2 emissions, other associated environmental impacts and plastic waste is considered through remote clinical consultations, recycling, patient education and the provision of high-quality care to achieve high impact environmentally sustainable outcomes.
CPD/Clinical Relevance: Environmentally sustainable oral healthcare requires the combined efforts of all stakeholders across the supply chain. The provision of good oral healthcare can deliver environmentally sustainable outcomes from a reduced need for interventions.
Article
Oral healthcare, in the form of prevention, therapeutic interventions and long-term maintenance, has an effect on the environment in the form of pollution, an increased carbon footprint, and an increase in other environmental impacts. In both domestic and clinical settings, much of the waste will end up as landfill or incineration, with some energy recovery in limited instances.1,2 Part one of this two-part series explored the sources of pollution arising from our professional activities in the provision of oral healthcare and how these activities appear to conflict with environmentally sustainable practice. Environmental impacts, plastic usage in the form of single-use plastics (SUPs, including packaging) and the use of dental materials and sundries are the largest contributors to pollution. Broader concepts were identified that influence these issues, such as the impact of supply chains, environmental citizenship and the effect of the COVID-19 pandemic.
Oral health professionals are required to carry out their duties to promote oral health in an ethical manner, to the highest quality standards, doing so in a safe manner with appropriate use of healthcare resources.3 In our dual capacity as citizens and oral healthcare providers, we have a moral and ethical responsibility to manage the impact of our activities in the environment and ensure that we do this sustainably.4,5 The first step to achieving this is to translate our behaviour of sustainable citizenship from the domestic environment to that of the work place to create a pervasive team attitude that will provide high-quality oral healthcare in an environmentally sustainable manner.6
The complex and mostly contaminated nature of the waste produced in the delivery of oral healthcare means that it is challenging to implement the established waste management strategies of reuse, reduce and recycle in the clinical healthcare setting.
Of these three strategies, the logical and immediately achievable approach to reducing waste in oral healthcare is through a reduction for the demand of materials and associated products. This reduction of need can be achieved through a promotion of better health focused on disease prevention coupled with the provision of high-quality interventions that do not require revising. This should be coupled with effective and pragmatic patient-centred maintenance plans.
This second article identifies the need to assess and establish a reliable baseline of scientific knowledge that will inform different approaches to mitigate these environmental impacts, including remote clinical consultations and recycling.
Assessment of environmental impacts
As with all major problems in life, understanding the scale of the issue is a prerequisite.2 Accordingly, the first step for planning sustainable dentistry requires a baseline assessment of the nature and the size of the problem. This will include an analysis of data on current practices, including dental materials and SUP use. Dentistry is truly unique in its use of a wide range of very specific materials and operates in a highly regulated healthcare environment. It provides an opportunity to study and understand the impacts of these materials through sophisticated mathematical modelling referred to as life cycle assessments (LCA). LCAs are techniques for assessing the potential environmental impacts and aspects associated with a product or service.
Establishing a system boundary and functional unit;
Compiling an inventory of relevant inputs and outputs;
Evaluating the potential environmental impacts associated with those inputs and outputs;
Interpreting the results of the inventory and impact phases in relation to the objectives of the study.
To use the term ‘life cycle’ with respect to the use of dental materials and SUPs could be regarded as a misnomer, as a life cycle implies that usage is circular, that is, where part or all of the material is reused. Instead, as we have identified, the use of dental materials and indeed the multiplicity of SUPs in dentistry can be described as being predominately linear, because the materials are made, used and disposed of in landfill or via incineration. With this in mind, LCAs for dental materials can be complex and all-encompassing, or they can be used to determine the environmental impact of a specific component within the life cycle of these materials. This is especially useful for dental restorative materials because they are not simple entities and their environmental fate must be considered to be: part of a complex manufacturing and distribution network; part of a complex system with different constituents and packaging; often part of a complex restorative process with other sundries (eg impressions require trays and crowns require cements); and part of a restored dentition that is attached to an additional complexity, a human. There is a danger of naively considering dental materials in isolation and not considering these complexities, which a well-designed LCA can accomplish. The overarching goals of LCAs make them an invaluable tool to enable evidence-based decision making.8,9,10 A robust LCA could determine which restorative dental materials, waste management strategies, dental waste products (such as empty composite compules and associated packaging) result in the lowest environmental impacts.
LCAs can be performed from ‘cradle to gate’, which describes analysis of impacts caused by the material manufactured by the company until it reaches the gate of the factory. A wide range of environmental impacts can be assessed including (but not limited to) the global warming potential (GWP, a quantification of climate change that measures the change in the Earth's temperature cause by greenhouse gas emissions from anthropogenic activities), human toxicity (which measures the toxicity of a compound, and its potential dose, to determine the harm caused on its release into the environment), eco-toxicity (a measurement of the tolerable concentration of harmful substances in water to different ecosystems), eutrophication (caused by nutrient accumulation in ecosystems) and ozone depletion (degradation of the ozone layer caused by the release of ozone depleting substances).11
Analysis of the fate of the dental materials, associated packaging, the GWP and other environmental impacts after this point are difficult to ascertain due to a dearth of available data. A more complete ‘cradle to grave’ analysis, which follows the journey of the material from manufacturing, to use, to disposal would be the only way to fully understand the complete environmental impact of dental materials. This is where collaboration between stakeholders, including manufacturers, distributors, policy makers, regulators, public administration, purchasers, academics, experts, clinicians, consumers and patients, is essential to fully analyse the impact of dental material use. By working together, and analysing dental material life cycles (including the opinions of patients who receive these restorations) better, more sustainable and well-accepted treatments can be provided.
Reducing CO2 emissions through remote clinical consultations
The risks associated with in-person appointments throughout the COVID-19 pandemic can be mitigated through the use and wider adoption of teledentistry for the provision of advice and remote clinical consultations (RCCs) (Figure 1). This is part of the NHS strategy that is actively being considered to reach its NHS Net Zero carbon emissions target by 2040.12
Figure 1. Remote clinical consultation between a dental practice with the patient and own GDP (left) and a remote specialist/consultant (right). Transmission of live data through multiple two-way audio-visual channels (multiple cameras, including intra-oral) and radiographs, using secure super-fast broadband connectivity.
Remote clinical consultations reduce the need for patient travel with an associated reduction of CO2 emissions. Teledentistry has been previously used to eliminate disparities between rural and urban communities and improve community access to oral healthcare.13,14 Today, RCCs facilitate expert or consultant-led treatment planning with the patient involved in the process.15 RCCs using technology that currently exists in the form of secure, live, superfast internet connectivity and high-resolution, multi-channel audio-visual streaming can provide patient-centred, cost-effective, safe and efficient care that is well accepted by patients.16 Teledentistry and RCCs are now actively promoted for their additional beneficial impact of reduction in air pollution caused by road travel, high patient satisfaction and patients not having to take time off work and/or travel with associated costs.17
After travel, the second largest contributor to carbon emissions from primary care dentistry is through procurement, or the acquisition of goods and stock required for dental service provision, which includes dental materials. It is noteworthy, that most dental materials originate from a small cluster of manufacturers that are mainly located in the European continent, Japan and the USA, with a significant carbon footprint associated with the required long-distance transport.
What about recycling?
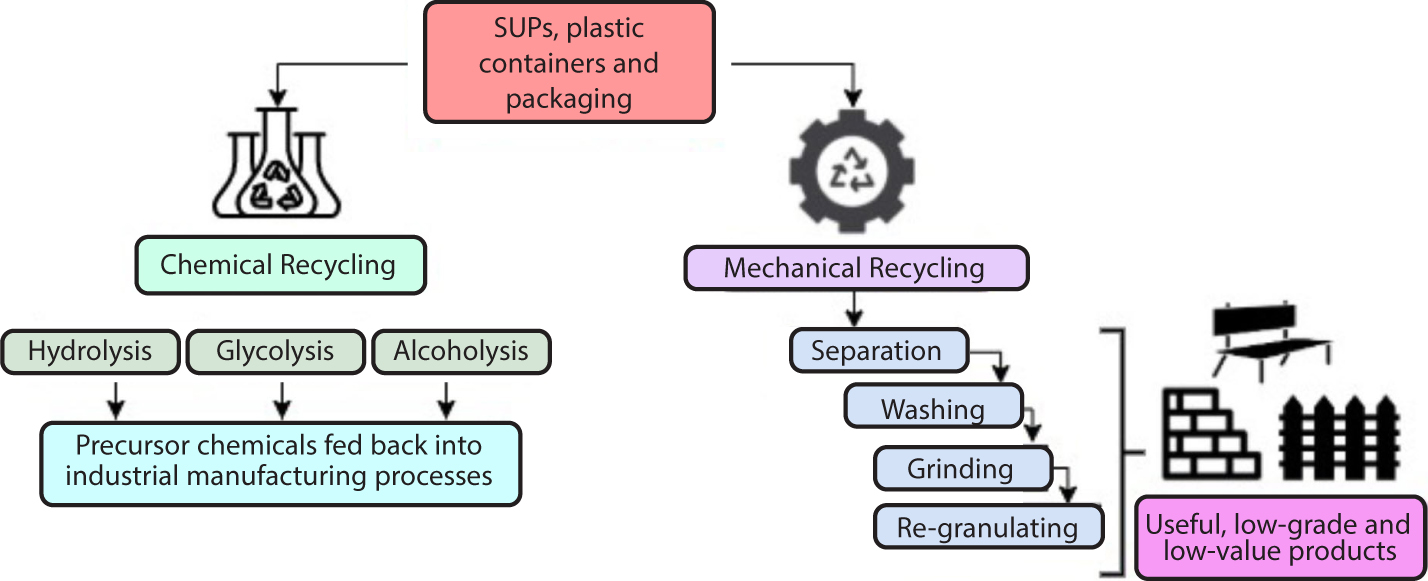
Plastic waste can be recycled through mechanical and chemical routes (Figure 2).18 Essentially, mechanical recycling is a physical process of separating, washing, grinding and re-granulating plastics; a process that results in useful a low-grade and low-value product that is mainly used to make items such as construction building blocks, park benches, fence posts and waste bins. Chemical recycling breaks down chemical bonds to depolymerize condensation polymers such as polyamides (eg nylon tooth brush bristles) and polyesters (eg trays, containers, film) through processes such as hydrolysis, alcoholysis and glycolysis. Chemical recycling results in precursor chemical products that can be readily recycled and used as valuable feedstock for industrial plastic manufacturing processes.
Figure 2. Chemical and mechanical recycling has the potential to develop a circular economy that is less dependent on raw materials and waste management through landfill and incineration.
Frustratingly, not all polymers can be depolymerized. Addition polymers, such as polyolefins (eg polyethylene (PE), polypropylene (PP), polystyrene (PS), cannot easily be depolymerized to monomers, making them inefficient and expensive to recycle. Others, such as polyvinyl chloride (PVC), present significant challenges as they release HCl and organic Cl-containing by-products through thermal processing. The single largest contributor to plastics in the dental surgery comes from packaging because the product travels from the manufacturer downstream to the dental surgery after which the majority (>90%) ends as waste for incineration or landfill (Figure 3).19 The packaging sector in the EU accounts for 65% of the main plastics used in healthcare divided as follows: low density PE (17.5%), PP (19.3%), PS (6.4%), PVC (10%), high- and medium-density PE (12.2%).20 It is encouraging, however, that managing this plastic packaging waste stream is a major research priority for the UK and other nations, with significant target-driven research initiatives underway. The UK Plastics Pact has set a series of ambitious targets for 2025, with the headline of 100% of plastic packaging to be reused, recycled or compostable.21
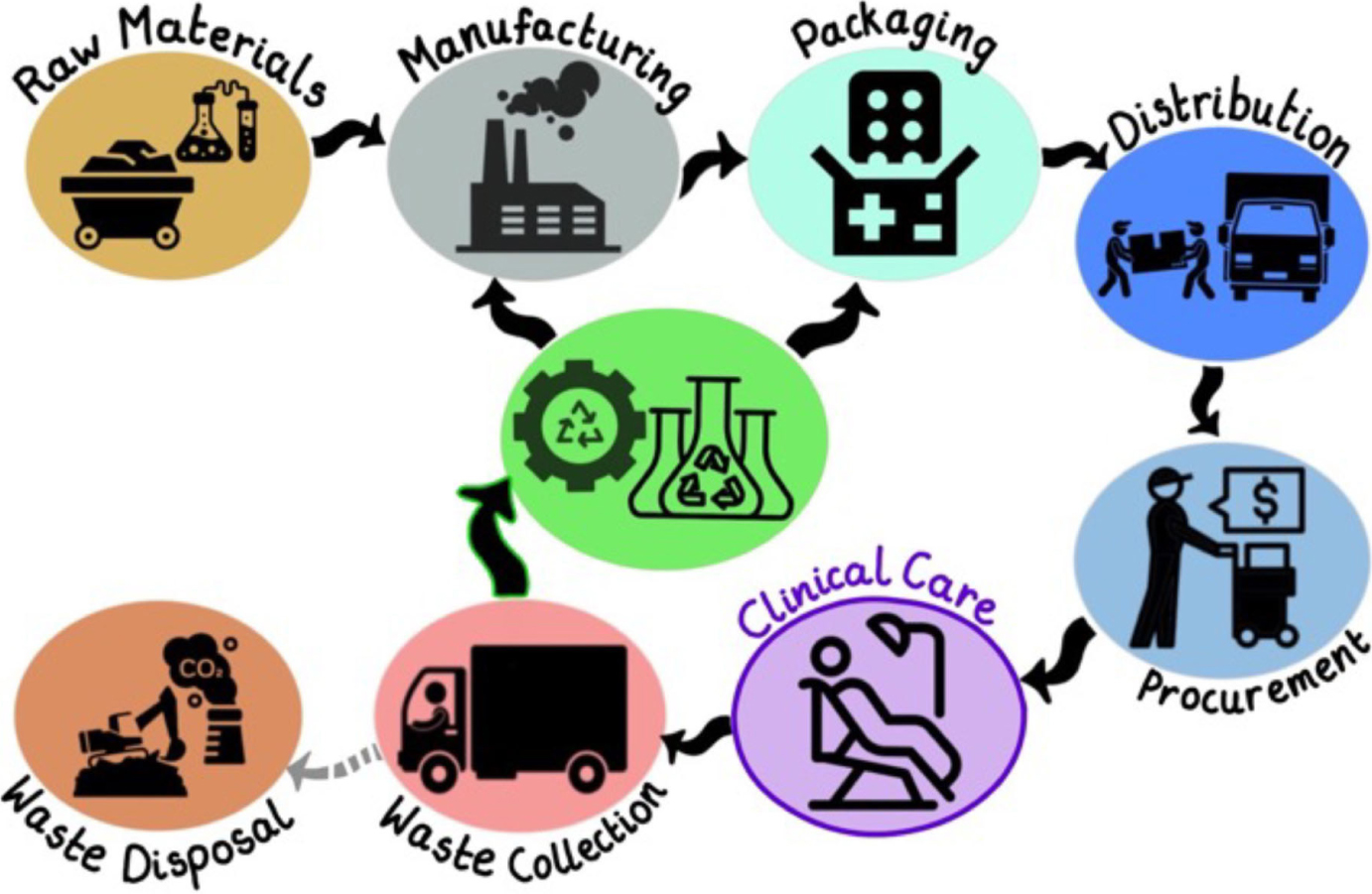
Figure 3. A circular economy supply chain, with a reduced reliance on the extraction and synthesis of raw materials and end-of life disposal in landfill or incineration. Waste from materials and packaging can be diverted back into the supply chain through mechanical and chemical recycling.
With regards to the actual plastic items used in the dental surgery, the greatest challenge is that they are contaminated and, therefore, considered potentially dangerous. As such, current EU and UK legislation requires very strict disposal routes.22 The largest contributors to SUPs in oral healthcare are nitrile examination gloves. In the UK, based on the number of dental care professionals registered with the General Dental Council in 2019, it is possible to extrapolate the national usage of nitrile gloves.23 The calculation assumes a figure of 110,000 dentists and DCP registrants (including nurses) that is rounded down from the official figure 113,439 (that acknowledges some elements of double counting); a 40-week working year, with an allowance for part-time working (mean 4 days/week); an average of 10 procedures/day (any clinical event requiring the donning of gloves); and working as a dentist/DCP and nurse team (two pairs of gloves/procedure, accounted for in the total number of 110,000 registrants). Multiplying these variables suggests that a conservative estimate for the number of disposable nitrile examination gloves used for the provision of oral healthcare in the UK is 176 million pairs of gloves per year (Table 1).
A
Approximate number of dental healthcare professionals (UK GDC Report 2019)
≈110,000
B
Working days per year
≈40 weeks x 4 days = 160
C
Number of clinical procedures per day
≈10
D
Approximate number of pairs of gloves per procedure
≈1
Total number of pairs of gloves per year
A x B x C x D
=176,000,000 pairs
Some programmes (eg Terracycle) are available for the collection and mechanical recycling of non-clinically contaminated gloves.24 This route is not available for clinical gloves used in dentistry or healthcare because they are classed as clinical waste and must be disposed of through regular clinical waste processes. Plastic sundries make up the remainder of the plastics in the dental surgery; where a further recycling challenge lies in the design of plastic products for functionality in healthcare. These have specific characteristics for a given application and often combine both condensation and addition polymers to obtain needed barrier properties and flexibility.
It is clear that the key to improve recyclability and a more circular economy, is to design simpler devices with plastics that can be disassembled or that lend themselves to cost-effective chemical recycling. Chemical recycling is the focus of intensive research, such as that pioneered by Garforth et al that employs a hydrocracking catalytic process that is tolerant of a mixed polyolefin (PE, PP and PS) with small amounts of PET (polyethylene terephthalate) and PVC, reducing rigorous collection and sorting regimes.25
In healthcare and dentistry, for truly sustainable plastic use, innovative recycling strategies are required to avoid complex, bespoke, expensive, multi-stage chemical separation and thermal treatments. The adoption of effective recycling technologies has the potential to impact our supply chain and divert much waste into a successful circular economy, with a reduced reliance on the extraction and synthesis of raw materials and end-of life disposal in landfill or incineration (Figure 3).
Education
Education is the prerequisite that will facilitate incorporating sustainability within the profession. This starts from undergraduate training by incorporating sustainability within the curricula of dental trainees; a process that is currently underway that considers how sustainability can be included in the undergraduate dental curriculum.26 Continued professional development (CPD) must include elements of sustainable practice and auditing and accreditation, such as the programme run by the Green Impact initiative, which should be encouraged within primary care.27 Educating patients regarding sustainability would follow naturally from this and be accepted and well received by not just the environmentally conscious cohort. This can be as simple as promoting ‘green’ travel and helping to accommodate it, such as highlighting public transport routes or providing an area to allow patients to secure their bicycles outside dental practices.
Good quality dentistry is sustainable dentistry
This article has previously identified the potential for a reduction in pollution, carbon emissions, and other environmental impacts by promoting and delivering high-quality care for the management of oral health, principally with a focus on preventable diseases. The provision of high-quality preventive care brings about notable and durable oral health benefits for the individual and the population at large, while reducing inequalities. Effective prevention regimes result in a reduced need to treat (preventable) oral diseases, which in turn results in less patient travel, with a net reduction in CO2 emissions and resources needed.2,28,29,30 The recent publication by PHE highlighting the inequalities in oral health in England recommends community interventions, such as targeted supervised tooth brushing in childhood settings and water fluoridation.31 These actions would reduce inequalities for those in more deprived areas while also improving sustainability through prevention. Prevention reduces costs to healthcare systems and has wider economic benefits. An example would be the cost of dental extractions (majorly caused by caries) required for 0–19 year olds in secondary care sites, which cost £50.5 million in 2015.32 To this we should now also add the financial burden associated with the environmental impact from the treatment of preventable diseases (eg caries and periodontal disease).
The provision of good dentistry translates into a reduced need for restorative dentistry, less material used, fewer prostheses and fewer visits. This reduction in treatment need translates to a reduced amount of carbon emissions, other environmental impacts and pollution; both a welcome, but unintended consequence of providing good-quality oral healthcare.
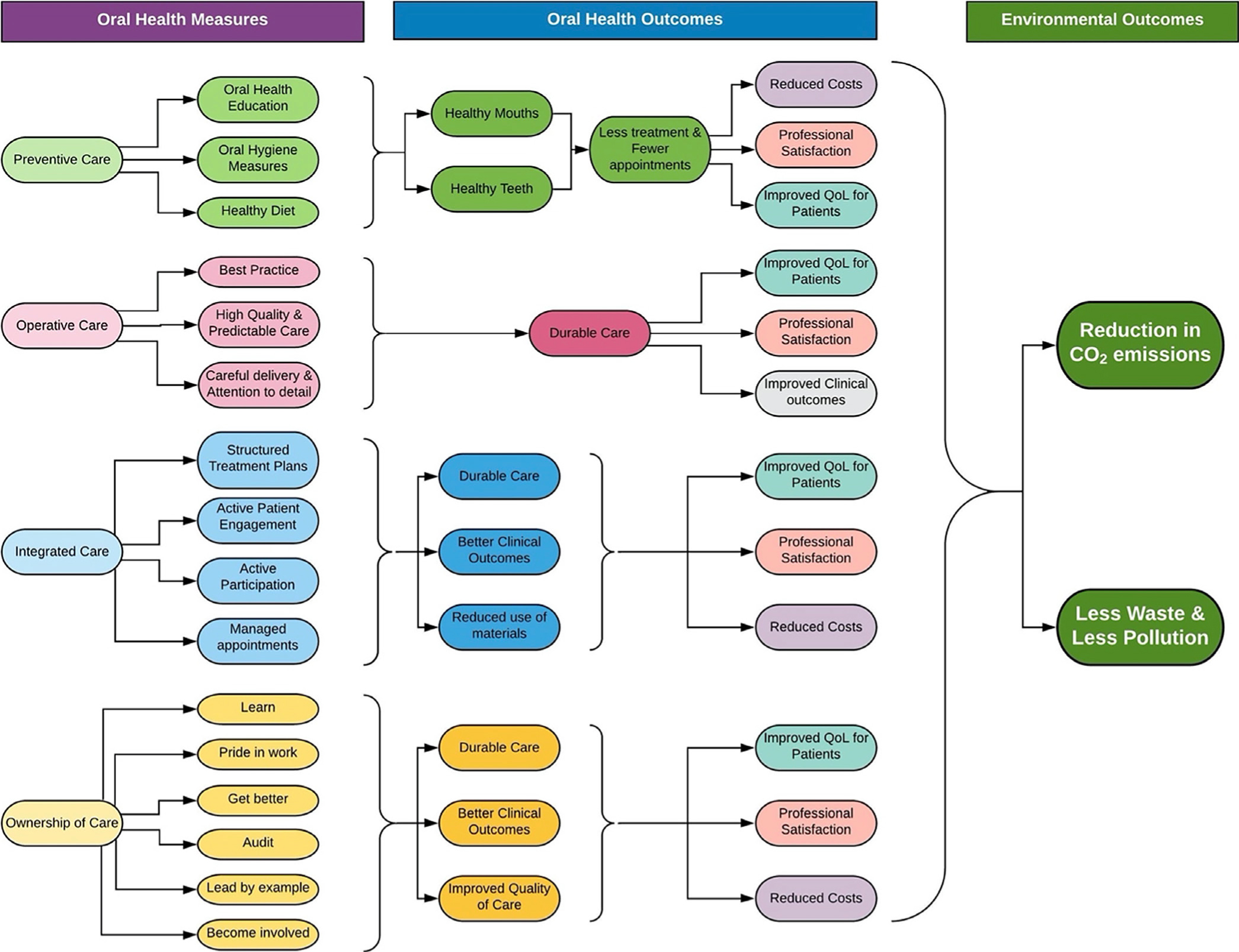
The authors suggest that effective and durable patient-centred oral healthcare can be achieved by considering the domains: preventive care, operative care, integrated care and ownership of care (Figure 4).3
Figure 4. The relationship between oral health measures (first column), their impact on good oral health outcomes (second and third columns) and, as an unintended consequence, in environmentally sustainable outcomes (fourth column).
In this way, the dental team, working in partnership with their patients, can deliver environmentally sustainable oral health simply by jointly striving to achieve high standards of care. The aim of this strategy is threefold:
The provision and promotion of good oral healthcare is core to what we do as professionals, and as such we should strive to do this as well as possible.
We can provide and promote good oral health by pursuing excellence in each of the domains that make up our everyday practice.
If we provide and promote good oral health, we will need to do fewer interventions, which will result in higher oral health outputs. This in turn, will result in environmental gains brought about by:
A reduced use of materials that will consequently reduce the overall amount of waste produced at the point of manufacturing, packaging and clinical care.
Reduced number of patient visits for routine dental care that will equate to reduced travel and thus, a reduced patient-based carbon footprint.
This message is very simply encapsulated in the statement: good oral healthcare is good for the patient and good for the profession and (as an unintended consequence) it is also good for the environment’ (Figure 5).
Figure 5. Good quality oral health provision results in good oral health outcomes and environmentally sustainable dental care outcomes.
Sustainability and the supply chain
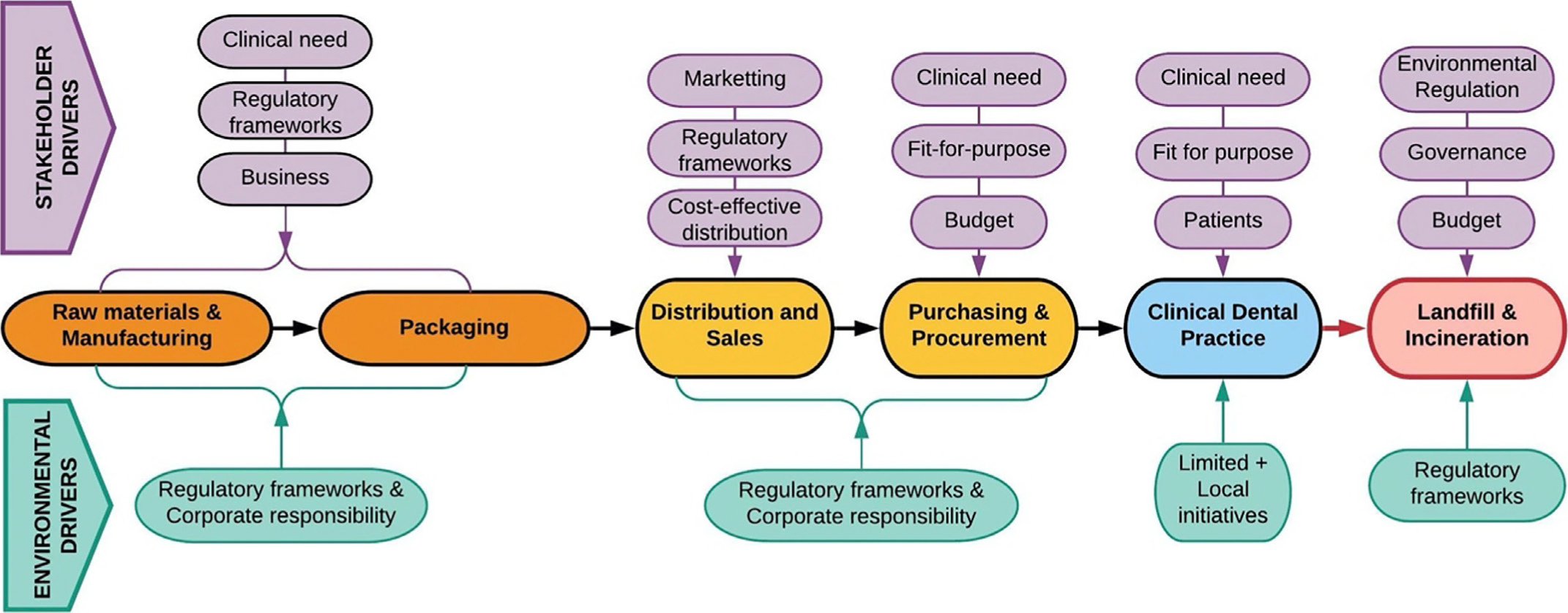
COVID-19 has had a profound effect on dentistry and will probably continue to do so indefinitely. Prior to the pandemic, environmental concerns regarding SUPs, carbon emissions and other environmental impacts from the provision of oral healthcare and the use of dental materials in particular, was a source of concern for the profession. It is clear that, although our professional focus remains on the provision of oral healthcare, the issue of environmental sustainability has not gone away and has been hugely magnified with the extensive use of PPE during the COVID-19 pandemic. The impact of dental materials, sundries and equipment on the environment is not restricted to daily dental practice, but starts a long way upstream of the supply chain when the raw materials are synthesized, prior to manufacturing or assembly into restorative materials, devices or packaging. Our activities as healthcare professionals are a long way down the supply chain, just before the final stage of waste management (Figure 3). In the supply chain, goods travel from the raw materials and manufacturing (at the head of the chain), via distribution and procurement, to the end user in clinical practice, and eventually to an end point for end-of-life waste management. Each stakeholder along the chain is principally driven by commercial pressures and their own individual business models. Limited attention is given to sustainability outside the need to comply with regulatory bodies and some environmental action as part of their own corporate responsibility, included within the framework of the company's environment, social and corporate governance frameworks (ESG). Historically, stakeholders have not readily taken any responsibility for the impact of their products or processes downstream of the supply chain. For example, dental manufacturers create restorative materials according to best practice, in compliance with regulatory bodies. In doing so, some sustainable goals are achieved; however, there is less preoccupation with regards to the environmental impact of the carbon footprint of distribution, the use of the materials, packaging or waste disposal. Essentially, there is a lack of whole supply chain ‘joined up’ environmental responsibility for products as they travel downstream and are conveyed from stakeholder to stakeholder (Figure 6).
Figure 6. Linear supply chain that is principally driven by the individual stakeholder drivers (top) that are core to the commercial business model. The environmental drivers (bottom) are largely focused on compliance with regulatory frameworks and corporate responsibility.
As healthcare providers we need to realize that we hold the ace card and have the capability to influence manufacturers, distributors and waste management companies to support our sustainable practice endeavours. In this way, our sustainable actions will have significantly greater impact than being simply limited to local small-scale initiatives, useful as they may be. In this context, it is important that we understand that our actions or inactions as providers of sustainable practice will have significant impacts in the way that other stakeholders react up and down the supply chain.
Conclusion
In order to reduce carbon emissions and other environmental impacts, we need to establish a robust knowledge base for current activities. This is vital to enable the profession and the supply-chain stakeholders to set effective targets. Life-cycle assessments are very useful in this respect, but the results obtained are only as good as the quality of the data that informs the analysis. There is also a need for all stakeholders in manufacturing, distribution, end users and waste management to engage effectively to create this database of core knowledge.
Strategies to manage the impact of our activities on the environment:
The smart use of IT to develop effective care pathways with remote clinical consultations as an example, can help mitigate the impact of commuting traffic.
The impact of dental materials should be considered, even as we phase out the use of dental amalgam, which is considered a significant pollutant. Other materials, such as RBCs also have an environmental impact, and this should be considered further.
Single-use plastics present a big environmental challenge in healthcare. There is a clear need to first acknowledge their invaluable and indispensable contribution to healthcare in general and to oral healthcare in particular. SUPs are essential to the operation and delivery of safe and effective clinical outcomes. We need to identify ways of reducing their use and increasing their recovery and recycling rates.
The COVID-19 pandemic has highlighted the need for increased use of SUPs in personal protective equipment, guards and equipment sheaths, as a key part of our strategies to reduce the risk of contagion. History tells us that this is unlikely to be a one-off event and that once a pattern has been set and established, it is likely to mould our future practice and our reliance on this extra PPE in our future professional activities.
Recycling technologies are evolving rapidly, but improved technology will not solve the problem if it is not matched with a strong individual and team attitude to recycling that creates effective and practical collection and processing strategies.
We can all play a role in the delivery of oral healthcare in a sustainable manner, and education is at the heart of this. Sustainability is now being embedded in undergraduate curricula and continuous education programmes at all levels of professional activity. Oral health professionals need to engage with this educational process and give it the same level of importance as any other professional CPD programme.
A key message is that ‘Good oral healthcare is good for the patient and good for the profession and it is also good for the environment’ (Figure 5). Thus, by doing our job well, with effective professional and patient engagement, we can make a direct and real contribution to the reduction of the waste, CO2 emissions and other environmental impacts that arise from our practice.
While we can focus on the problem of sustainability as being the responsibility of oral healthcare providers, it is important to note that in reality this is a problem shared with all other stakeholders up and down the oral healthcare supply chain.
Net zero and carbon-negative emissions and a reduction of plastic waste going to landfill is achievable, by taking individual responsibility for our actions at a professional level and through conscious and deliberate decisions at every step of the healthcare supply chain.