Hassan O, Shoukry T, Raouf AA, Wahba H Combined palatal and buccal flaps in oroantral fistula repair. Egypt J Ear Nose Throat Allied Sci. 2012; 13:77-81
Khandelwal P, Hajira N Management of oro-antral communication and fistula: various surgical options. World J Plast Surg. 2017; 6:3-8
Eberhardt JA, Torabinejad M, Christiansen EL A computed tomographic study of the distances between the maxillary sinus floor and the apices of the maxillary posterior teeth. Oral Surg Oral Med Oral Pathol. 1992; 73:345-346 https://doi.org/10.1016/0030-4220(92)90133-b
Kiran Kumar Krishanappa S, Prashanti E, Sumanth K Interventions for treating oro-antral communications and fistulae due to dental procedures. Cochrane Database Syst Rev. 2016; 5 https://doi.org/10.1002/14651858.CD011784.pub2
Voss PJ, Vargas Soto G Sinusitis and oroantral fistula in patients with bisphosphonate-associated necrosis of the maxilla. Head Face Med. 2016; 12 https://doi.org/10.1186/s13005-015-0099-0
Martines F, Salvago P, Ferrara S Parietal subdural empyema as complication of acute odontogenic sinusitis: a case report. J Med Case Rep. 2014; 8 https://doi.org/10.1186/1752-1947-8-282
Lizé F, Verillaud B, Vironneau P Septic cavernous sinus thrombosis secondary to acute bacterial sinusitis: a retrospective study of seven cases. Am J Rhinol Allergy. 2015; 29:e7-12 https://doi.org/10.2500/ajra.2015.29.4127
El Mograbi A, Ritter A, Najjar E, Soudry E Orbital complications of rhinosinusitis in the adult population: analysis of cases presenting to a tertiary medical center over a 13-year period. Ann Otol Rhinol Laryngol. 2019; 128:563-568 https://doi.org/10.1177/0003489419832624
Levine MH, Spivakovsky S Low quality evidence for treatment approaches for oro-antral communications. Evid Based Dent. 2017; 18:90-91 https://doi.org/10.1038/sj.ebd.6401260
Scattarella A, Ballini A, Grassi FR Treatment of oroantral fistula with autologous bone graft and application of a non-reabsorbable membrane. Int J Med Sci. 2010; 7:267-271 https://doi.org/10.7150/ijms.7.267
Shetty L, Kulkarni D, Pradhan R Oroantral fistula resulting from chronic periodontitis: a rare case report. Clin Adv Periodont. 2016; 6:(1)
Huang CH, Brunsvold MA Maxillary sinusitis and periapical abscess following periodontal therapy: a case report using three-dimensional evaluation. J Periodontol. 2006; 77:129-34 https://doi.org/10.1902/jop.2006.77.1.129
Mora C Penetration to maxillary sinus during periodontal therapy. J Periodontol. 1962; 33:200-201
Moskow BS A histomorphologic study of the effects of periodontal inflammation on the maxillary sinus mucosa. J Periodontol. 1992; 63:674-681 https://doi.org/10.1902/jop.1992.63.8.674
Naito T, Hosokawa R, Yokota M Three-dimensional alveolar bone morphology analysis using computed tomography. J Periodontol. 1998; 69:584-589 https://doi.org/10.1902/jop.1998.69.5.584
Waldrop TC, Semba SE Closure of oroantral communication using guided tissue regeneration and an absorbable gelatin membrane. J Periodontol. 1993; 64:1061-1066 https://doi.org/10.1902/jop.1993.64.11.1061
Ogunsalu C A new surgical management for oro-antral communication: the resorbable guided tissue regeneration membrane – bone substitute sandwich technique. West Indian Med J. 2005; 54:261-263 https://doi.org/10.1590/s0043-31442005000400011
Lee BK One-stage operation of large oroantral fistula closure, sinus lifting, and autogenous bone grafting for dental implant installation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:707-713 https://doi.org/10.1016/j.tripleo.2007.09.020
A case of grafted repair of an oro-antral fistula following non-surgical periodontal therapy Claudia Heggie Kelly Smorthit Banoo Sood Tom Thayer Dental Update 2024 48:6, 707-709.
Authors
ClaudiaHeggie
BDS, MFDS (Ed)
Dental Core Trainee, Liverpool University Dental Hospital
Oro-antral communication is a well-recognized complication of dental extractions in the maxilla, but is rarely reported to occur from periodontal causes. This article describes the formation of an oro-antral communication following non-surgical periodontal therapy, and its subsequent management.
CPD/Clinical Relevance: This article presents a previously unreported formation of an oro-antral communication following non-surgical periodontal therapy, in a patient with localized periodontitis and presence of a root cementum defect. It is of relevance to all dentists managing periodontal disease.
Article
In this article, we report a case of oro-antral communication following non-surgical periodontal therapy. Oro-antral communication most commonly occurs during extraction of upper molar and premolar teeth due to the proximity of the roots of these teeth to the antral floor.1,2 The average distance of apices of maxillary molars from the sinus floor has been reported as 1.97 mm.3 Other well-accepted causes of an oro-antral communication include: tuberosity fracture; peri-apical infection; trauma; displacement of an implant or apex of a root into the antrum; maxillary cysts or tumours; osteoradionecrosis; and medicine-related osteonecrosis.4,5
Oro-antral communication may lead to significant complications and may have a considerable impact on quality of life. Consequent acute maxillary sinusitis with pain and discharge, that may potentially lead to serious complications, is common.6,7,8,9 When a communication persists, maxillary sinusitis may become intractable. However, symptoms may be less severe over time, reflecting a change to a chronic state. There is debate in the literature between conservative and surgical management of oro-antral communication, and evidence for definitive approaches is lacking.10 In many cases, small communications (<5 mm), in the presence of a healthy sinus may heal spontaneously and may occur more commonly than recognized. Larger communications typically require repair.11,12 Surgical splints can be used to keep the site clean and reduce symptoms during conservative management.13 Approaches for repair of an oro-antral communication all involve placing a material to fill the defect, and range from classical soft tissue with buccal or palatal advancement flaps, through fat pad grafts, to the use of autologous, allogeneous grafting materials, or xenografts.4,11,14
A literature review revealed a report of formation of an oro-antral communication believed to be a consequence of untreated chronic periodontitis, and a case of maxillary sinusitis and oro-antral communication following surgical periodontal therapy.15,16 However, to the authors' knowledge, there are no reports in the literature of an oro-antral communication following non-surgical periodontal management.
Case report
Restorative management
The patient, a 34-year-old male, was initially referred to the restorative department for management of localized periodontitis associated with the upper left first molar (UL6). The patient reported a history of root surface debridement at his dental practice every 3 months in this area. His oral hygiene regimen consisted of brushing his teeth twice daily, with supplementary use of interdental brushes. Medically, the patient reported an allergy to penicillin, hay fever, and asthma controlled by salbutamol inhaler as required. On examination, his oral hygiene was found to be good with minimal bleeding on probing and a BPE score of:
1
1
4
1
0
1
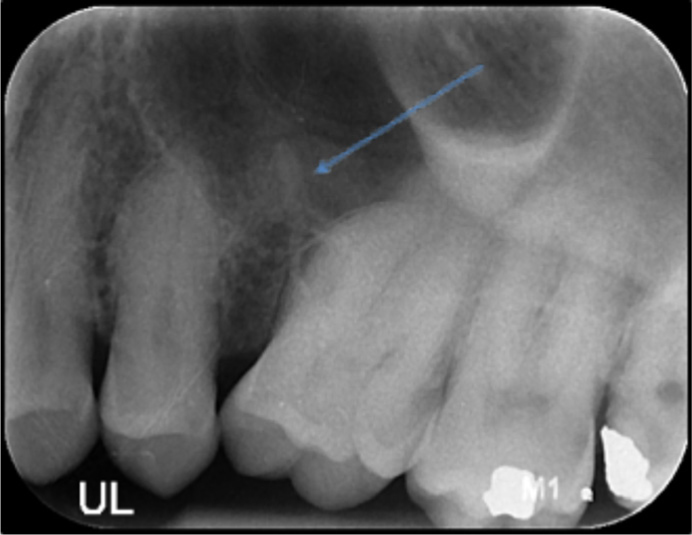
The UL6 had a deep mesio-palatal pocket with subgingival calculus detected and absence of bleeding on probing. The tooth was mesially inclined and mild spacing noted in the sextant. Radiographic examination showed a wide infrabony defect with a 60% vertical component and the appearance of diffuse bone loss (Figure 1). No peri-apical pathology was noted.
Figure 1. Appearance of defect on periapical radiograph taken at initial periodontal examination. Arrow indicating cemental spur, later found on pre-surgical CBCT (Figure 3).
A diagnosis of localized aggressive periodontitis associated with the UL6 was made. The treatment plan consisted of oral hygiene instruction for interdental brush resizing, baseline periodontal indices and root surface debridement (RSD) of the UL6 under local anaesthetic. Review for subsequent use of adjunctive systemic antimicrobials was arranged on the specialty training clinic.
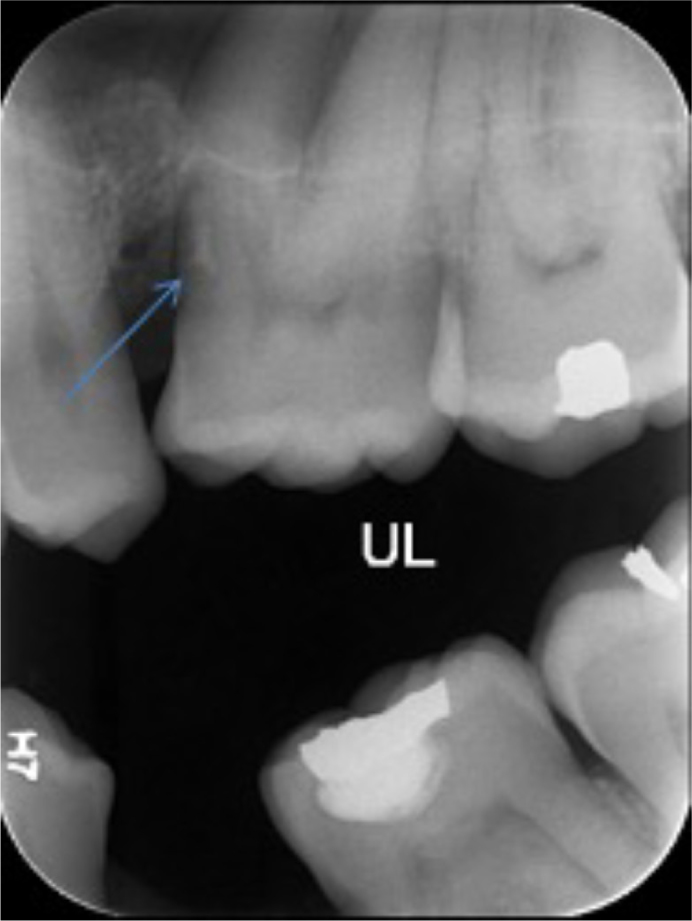
The first course of RSD proceeded uneventfully. At the 3-month periodontal reassessment, the bitewing radiograph obtained suggested a reduction in the bony defect, but without resolution (Figure 2). Further RSD and insertion of a Periochip (Dexcel Pharma, UK) in the mesio-palatal pocket of the UL6 was arranged. At this appointment, following subgingival calculus removal, probing depth of 13 mm and grade II mesio-palatal furcation involvement of UL6 was recorded, and a Periochip was placed. Additionally, a sharp ridge was noted on the palatal aspect of the mesio-buccal root.
Figure 2. Vertical bony defect and aberrant root morphology UL6 mesial observed on bitewing radiograph. Arrow indicates cemental spur, later found on pre-surgical CBCT (Figure 3).
The patient contacted the department later in the day to report that he was finding liquids to be passing from his mouth to his nose. He was reviewed urgently with additional input from an oral surgeon. The patient later mentioned that he had experienced a sensation of ‘drowning’ during the most recent ultrasonic debridement. There was an absence of swelling or discharge associated with the UL6, but the symptoms clearly suggested a diagnosis of oro-antral communication and conservative management in the interim was advised.
Surgical management
Arrangements were made by the oral surgery department for cone beam computed tomography (CBCT) of the UL6 region to assess the local anatomy and to aid treatment planning.
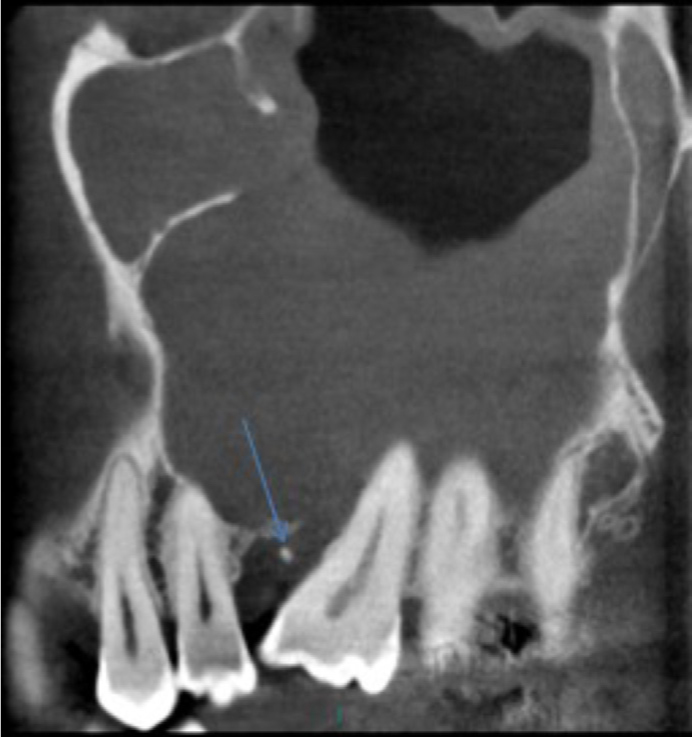
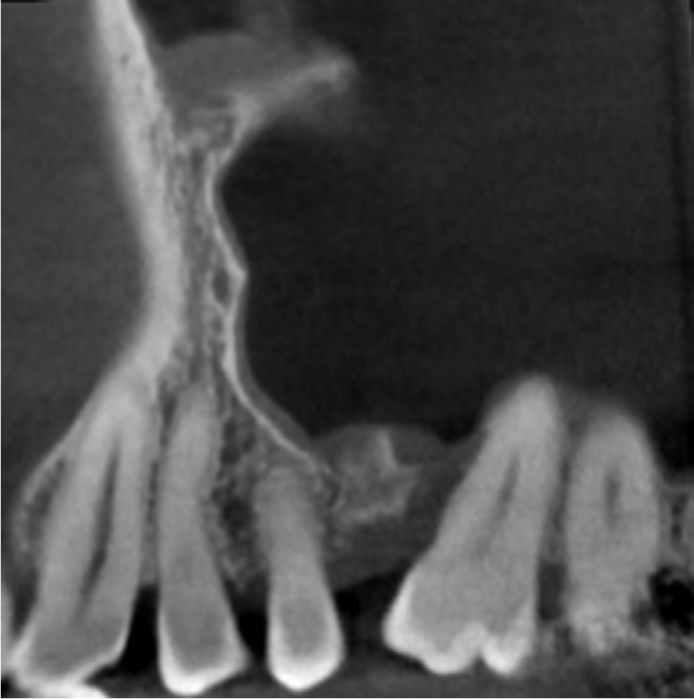
The imaging showed mild crestal periodontal bone loss with a mesial angular bony defect associated with the UL6. The left maxillary sinus was well pneumatized, invading the alveolus to expose the roots of the molar teeth. Mesial to the UL6 roots, the sinus floor was particularly thin, with a 3x3 mm focal break at the palatal aspect of the mesio-buccal root and mesial to the palatal root. There was evidence of an extensive inflammatory response within the antrum, and a radio-opacity lying horizontally between the UL5 and UL6 was noted (Figure 3).
Figure 3. Pre-surgical CBCT imaging of oro-antral communication shows focal defect in floor of sinus, extensive inflammation of the antral cavity lining and cemental spur in cross section. Arrow indicates cemental spur.
The patient reported that he had experienced recurrent chronic sinusitis in the interim, which had been managed by his medical practitioner with multiple courses of clarithromycin and doxycycline. His last episode had resulted in trismus, swelling and discharge from the area. He reported, however, that he was no longer experiencing fluid exchange from his mouth to his nose and was now able to drink through a straw. Clinically, a deep periodontal pocket could be probed at the mesio-palatal surface of the UL6 (Figure 4).
Figure 4. Pre-surgical assessment of UL6.
The symptoms experienced by the patient were severe and repetitive, and a strong indicator for intervention with a surgical approach. Treatment options broadly discussed were surgical repair of the defect or extraction of the tooth with subsequent alveolar repair. However, extraction would produce a large defect in the floor of the antrum that would be difficult to repair. Consequently, exploration of the defect with localized repair by grafting was planned.
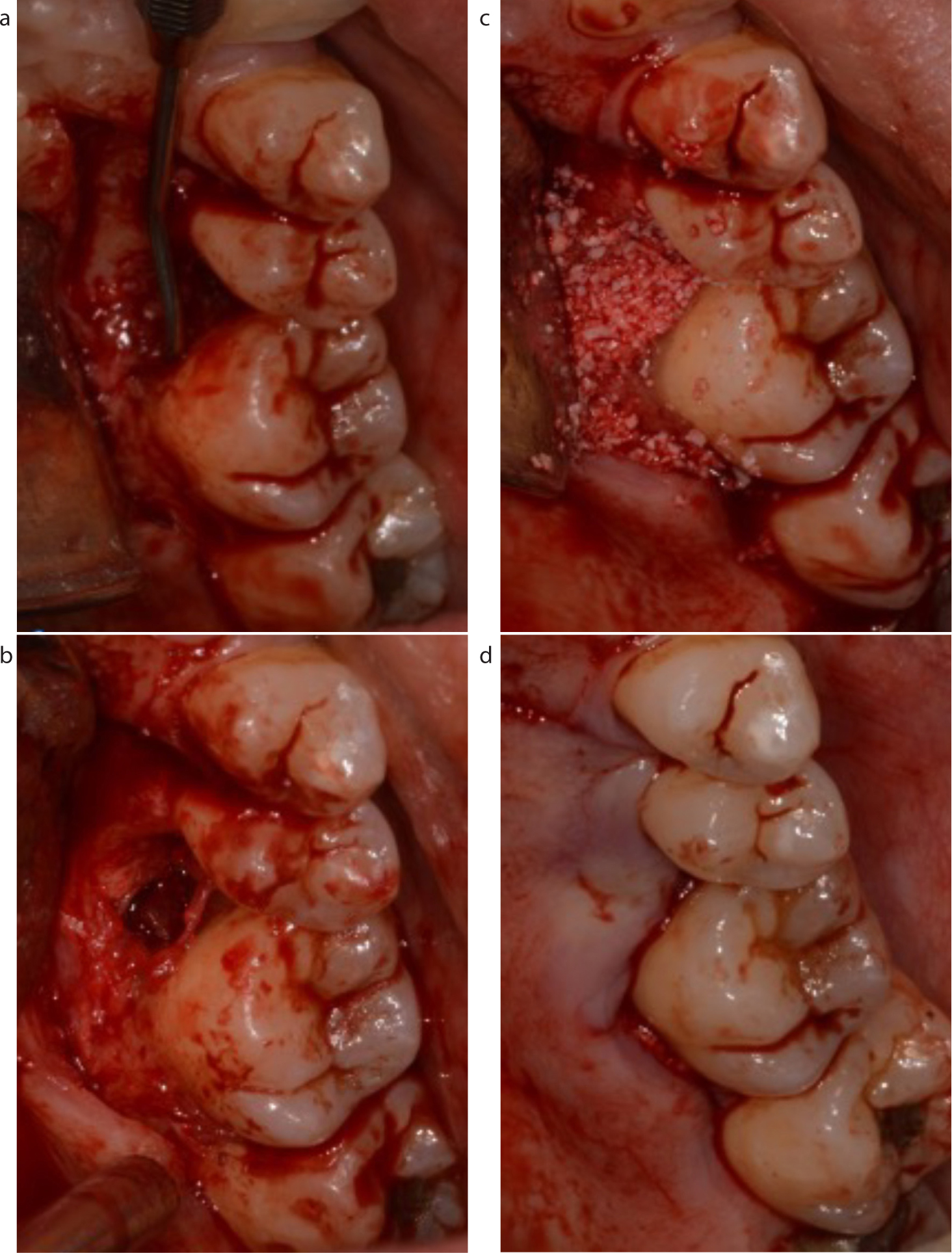
Under local anaesthetic, a two-sided, full thickness mucoperiosteal flap was raised with excision of the fistulous epithelial tract. Curettage of the surrounding bone was completed as well as root surface debridement. Clinically, there was a distinct communication from the oral cavity into the sinus from the mesio-palatal aspect of the UL6, with no exudate or fluid excretion.
The radiopaque body observed on imaging was retrieved from the site, and sent to histopathology for examination, revealing the tissue fragment to have an appearance more in line with cementum than bone. This cementum fragment may have inhibited healing and contributed to the chronic infection in the area, as well as being a local aggravating factor for the occurrence of localized periodontitis.
A bovine-derived xenograft, Bio-Oss (Geistlich, UK), was placed into the defect to facilitate bone regeneration, and the soft tissue repair was achieved with primary closure of the site using simple interrupted sutures (Figure 5). A membrane was not placed at this time. Conventional post-operative instructions and antibiotics were given.
Figure 5. Surgical repair UL6. (a) True extent of defect with probe extending into sinus following raising of mucoperiosteal flap. (b) Bony defect following removal of granulation tissue (c) Xenograft placed into defect. (d) Flap replaced for closure of surgical site.
At the 4-week follow-up, the patient's symptoms of sinusitis had resolved, and there was an absence of fluid passage between oral and nasal cavities. The 4-month follow-up and repeat CBCT showed closure of the communication with partial bony infill, and a soft tissue seal (Figure 6). The inflammatory changes in the antrum had largely resolved, with minor thickening only at the site of the communication. Review of the pre- and post-repair CBCTs obtained by the oral surgery team, highlighted the presence of the root cementum defect in the form of a spur.
Figure 6. UL6 4-month post-surgical CBCT shows closure of communication with soft tissue seal, partial bony infill and resolution of sinus inflammation.
Discussion
An odontogenic origin for maxillary sinusitis is well known, although this is commonly related to peri-apical pathology.17,18 Sinusitis as an extension of periodontal disease into the maxilla has been previously suggested, with pervasive extension of inflammatory infiltrates found on histopathology in the antral lining in those with moderate to severe periodontal disease.19,20 CBCT imaging has been shown to be accurate in assessing bone defects in periodontal disease, and a useful resource in guiding periodontal therapy in areas in close proximity to the maxillary sinus.16,21 However, given the limited additional diagnostic yield compared to clinical assessment and conventional intra-oral radiographs, the routine use of CBCT cannot be justified, given that sinus complications following periodontal disease and therapy are exceptionally rare.
In this case, in the first instance, repair of the defect with a xenogenous bone graft was the treatment of choice. This technique has been previously documented for successful repair of oro-antral communications following exodontia.22,23 Although successful outcomes of bone grafting without the use of a membrane for tissue regeneration have been reported, in retrospect, the use of a membrane may have enhanced bony regeneration at the site.24 The benefit of this technique compared to conventional buccal advancement flap closure in this case is primarily the opportunity to maintain the UL6 in the dentition. Extraction of the tooth and subsequent creation of a vast defect would make repair of an oro-antral communication extremely difficult, with a high likelihood of subsequent repeated breakdown and chronic infection. In reality, design of a suitable flap for a conventional non-graft approach would be impossible in this particular set of circumstances.
This case highlights that extraction, although the most common aetiology of oro-antral communication is not a prerequisite of the condition. Diagnosis of oro-antral communication should be made based on clinical signs and reported symptoms, and the chosen surgical intervention should aim to resolve these signs and symptoms. This may require a surgical graft approach given that in these situations, the associated tooth remains in the dentition.
For this patient, the resolution of sinus symptoms was a priority, after having had significant and repeated symptoms. The absence of sinus infection over a 4-month period post-operatively indicates a positive outcome in this case. However, although the tooth is asymptomatic, deep periodontal probing depths remain and so the prognosis is guarded. Long term, should sinus symptoms recur, extraction of UL6 and conventional repair of the defect will remain as a management option.
Conclusion
This article reports on the formation of an oro-antral communication following non-surgical periodontal therapy in a patient with localized periodontitis and aberrant root morphology, later confirmed to be a root cementum spur. There are no other recorded cases in the literature.
Oro-antral communication formation should be considered a rare, but significant, risk of non-surgical periodontal therapy in deep vertical bony defects of maxillary posterior teeth, where the floor of the maxillary antrum is in close approximation to the base of the periodontal defect. Xenografting in this case allowed maintenance of the tooth in the arch and the elimination of recurrent maxillary sinusitis.