Lieger O, Zix J, Stauffer-Brauch EJ, Iizuka T Synovial chondromatosis of the temporomandibular joint with cranial extension: a case report and literature review. J Oral Maxillofac Surg. 2007; 65:2073-2080
Guarda-Nardini L, Piccotti F, Ferronato G Synovial chondromatosis of the temporomandibular joint: a case description with systematic literature review. Int J Oral Maxillofac Surg. 2010; 39:745-755
Shah S, Ramanojam S, Gadre P Synovial chondromatosis of temporomandibular joint: journey through 25 decades and a case report. J Oral Maxillofac Surg. 2011; 69:2795-2814
Moses JJ, Hosaka H Arthroscopic punch for definitive diagnosis of synovial chondromatosis of the temporomandibular joint: case report and pathology review. Oral Surg Oral Med Oral Pathol. 1993; 75:12-17
te Veldhuis AH, Lobbezoo F, te Veldhuis EC, Naeije M, van Selms MK Synoviale chondromatose van het temporomandibulaire gewricht. Een systematisch literatuuronderzoek naar de kenmerken [Synovial chondromatosis of the temporomandibular joint. A systematic review of the literature on its characteristics]. Ned Tijdschr Tandheelkd. 2011; 118:421-426
Martín-Granizo R, Sánchez JJ, Jorquera M Synovial chondromatosis of the temporomandibular joint: a clinical, radiological and histological study. Med Oral Patol Oral Cir Bucal. 2005; 10:272-276
Wang P, Tian Z, Yang J Synovial chondromatosis of the temporomandibular joint: MRI findings with pathological comparison. Dentomaxillofac Radiol. 2012; 41:110-116
D’Souza B, Dimitroulis G A case of recurrence of synovial chondromatosis of the temporomandibular joint. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 104:59-61
Lucas JH, Quinn P, Foote J Recurrent synovial chondromatosis treated with meniscectomy and synovectomy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 84:253-258
Martín-Granizo R, Sánchez JJ, Jorquera M Synovial chondromatosis of the temporomandibular joint: a clinical, radiological and histological study. Med Oral Patol Oral Cir Bucal. 2005; 10:272-276
Synovial chondromatosis is a condition in which loose fragments of cartilage develop in the synovial membrane of joints due to metaplasia of the subsynovial connective tissue. The resulting symptoms are similar to those of temporomandibular joint (TMJ) dysfunction. Clinical diagnosis can therefore be challenging. Synovial chondromatosis rarely occurs in the TMJ as its predilection is towards larger joints. A systematic review up until June 2010 reported a total 241 cases of TMJ synovial chondromatosis. We present two cases of TMJ synovial chondromatosis seen and treated in our department.
CPD/Clinical Relevance: Awareness of TMJ synovial chondromatosis can enable patients to receive appropriate management before progression of the condition.
Article
Synovial chondromatosis (SC) is a condition in which loose fragments of cartilage develop in the synovial membrane of joints due to metaplasia of the subsynovial connective tissue. The synovial membrane is a soft tissue lining joints. It has a protective characteristic, containing the lubricating agent, synovial fluid.
Background
SC usually presents in large joints, most commonly reported in the knee joint.1 SC of the temporomandibular joint (TMJ) is rare,1,2 but not uncommon. A systematic literature review of 246 years, up to June 2010, reported a total of 241 cases of SC of the TMJ.3 SC is a benign condition; however, if left untreated, it can cause extensive destruction that can extend from the TMJ to the skull base in severe cases.
A patient with SC of the TMJ will complain of pain within the affected joint and subsequent dysfunction. Patients may also report any of the following symptoms:2,4
Swelling;
Dysfunction;
Crepitus;
Malocclusion;
Vertigo;
Tinnitus.
Clinical diagnosis is difficult owing to its presentation being similar to that of TMJ dysfunction. Definitive diagnosis is therefore achieved with arthroscopy alone or or in conjunction with cross-sectional imaging, such as magnetic resonance (MR) or computed tomography (CT).3,5 Histopathological analysis of the fragments obtained from arthroscopy is then required to confirm the diagnosis.5,6,7
Case 1
A 67-year-old woman was referred to the maxillofacial surgery department complaining of a 6-week history of initially shooting pain in the right side of her mandible, followed by trismus and difficulty with eating. She was generally fit and well, worked in school administration, and was a non-smoker and drank alcohol in moderation.
On clinical examination, she had acute tenderness over the head of the right TMJ and 30-mm mouth opening. Radiographic examination, in the form of an orthopantomogram (Figure 1), showed good bone stock in the right condylar head and no evidence of pathology.
Figure 1. Orthopantomogram showing good bone stock and no pathology in the right TMJ.
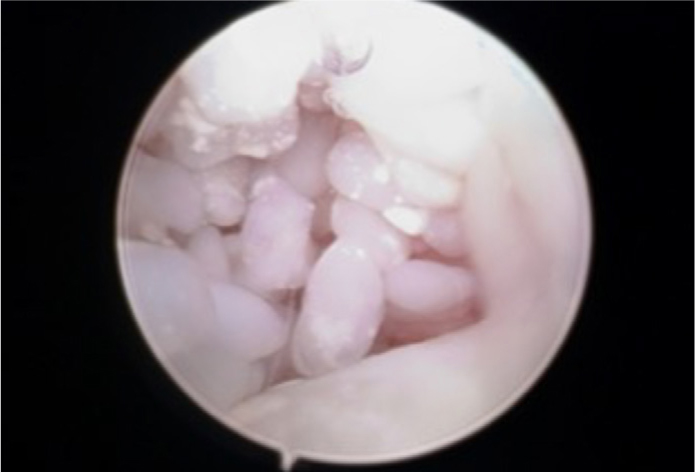
Conservative management with ibuprofen gel massages over the right TMJ area was initially advised, as would be the case with any patient suspected with TMJ dysfunction. The symptoms, however, did not resolve after 6 weeks and as it was unclear why she was experiencing them. A therapeutic arthroscopy with a steroid injection was offered. On performing arthroscopy, we were surprised to find hundreds of small nail-like fragments (Figure 2).
Figure 2. Arthroscopy of the temporomandibular joint showing hundreds of small fragments.
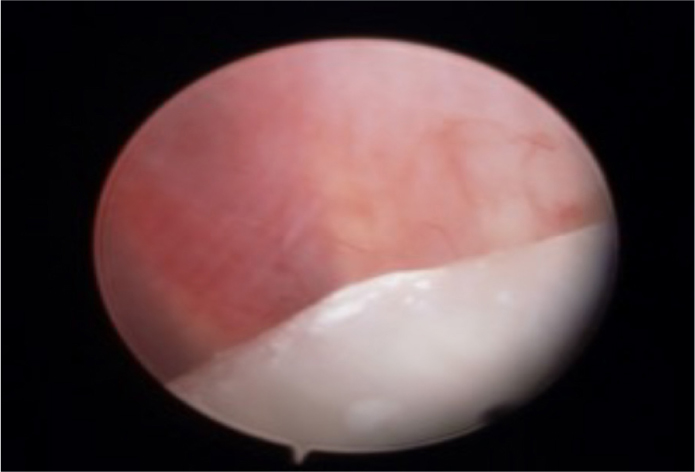
The joint space was cleared of all fragments (Figure 3) through washing out (Figure 4) and the fragments were sent for histopathological examination. Histopathology reported fragments of cartilage composed of mildly pleomorphic chondrocytes, confirming TMJ SC. The patient was reviewed 1 week post-operatively when she had increased mouth opening to 40 mm, no deviation, no crepitus and no functional impairment. One year following, she was still asymptomatic.
Figure 3. The TMJ cleared of all fragments.Figure 4. The fragments seen during arthroscopy were washed out of the temporomandibular joint space.
Case 2
A 29-year-old man was referred to the maxillofacial surgery department with crepitus on mouth opening, general throbbing pain in the mandible, daily locking, but with no trismus. His diet was not restricted and he did not need to take regular analgesia. Medically, he was generally fit and well; however, he did have a history of having had a fall while playing squash 5 years before, but he had not injured himself. He worked in telecommunications, was an occasional smoker and drank, on average, 10 units of alcohol per week.
On clinical examination he had crepitus, but no deviation of the mandible on mouth opening. MRI of his head was carried out, which showed SC of the right TMJ and erosion of the base of the skull. As a result of this finding, he underwent excision of the SC from the right TMJ and exploration of the right skull base and right temporal lobe. Loose bodies were seen herniating out of the right TMJ capsule and 20 loose bodies were removed. The synovium was also removed to prevent recurrence.8,9 Histopathological examination of the fragments confirmed the MR findings of TMJ SC.
On review after 6 months, he was asymptomatic and his crepitus had resolved. He had optimal mouth opening. An MRI 14 months later, showed no evidence of synovial pathology and he was still asymptomatic.
Conclusion
SC of the TMJ is rare, but it must not be excluded if a patient presents to general dental practice complaining of TMJ pain. The patient must be monitored and referred to secondary care should any pathology be supected. As seen from these cases, plain film alone is not enough to obtain a diagnosis. A definitive diagnosis is confirmed by adequate diagnostic work-up, including imaging and finally histopathological analysis10 of the specimens. Treatment of SC is dependent on the stage of the disease. In the early stages, arthroscopy removal of all of the loose bodies and affected synovium is sufficient; however if the SC has extended beyond TMJ synovium, then condylectomy or even discectomy may be necessary.