The term double tooth has often replaced the clinical diagnosis of gemination or fusion. If teeth have been extracted or exfoliated, the use of the neutral term ‘double tooth’ avoids the need to arbitrarily decide if it was gemination or fusion in origin. This case reports on a 16-year-old male who presented with an UL2 ‘double tooth’ and his combined restorative, surgical and orthodontic intervention to achieve his ideal result.
CPD/Clinical Relevance: A multidisciplinary approach should be adopted when treating patients with a double tooth and an appropriate protocol as cited can be used.
Article
Dental anomalies can be considered by the developmental stage at which they arise. Double teeth (geminated or fused teeth) arise during the dental lamina formation stage. However, the exact aetiology of gemination and fusion remains unclear. There are numerous hypotheses, some of which mention its association with local metabolic interferences, which occur in the morphodifferentiation stage of the tooth germ.1 Without further research being undertaken to investigate the embryological events during odontogenesis that lead to the development of this anomaly, it is difficult to determine the exact aetiological factors and pathogenesis underlying ‘double teeth’.2 The double tooth is a relatively common dental anomaly with a prevalence of 0.5% in the deciduous dentition and 0.1% in the permanent dentition, with no known variation between genders.3 The double tooth can be linked to syndromes such as achondroplasia and chondroectodermal dysplasia, although this anomaly can still found in non-syndromic patients.4
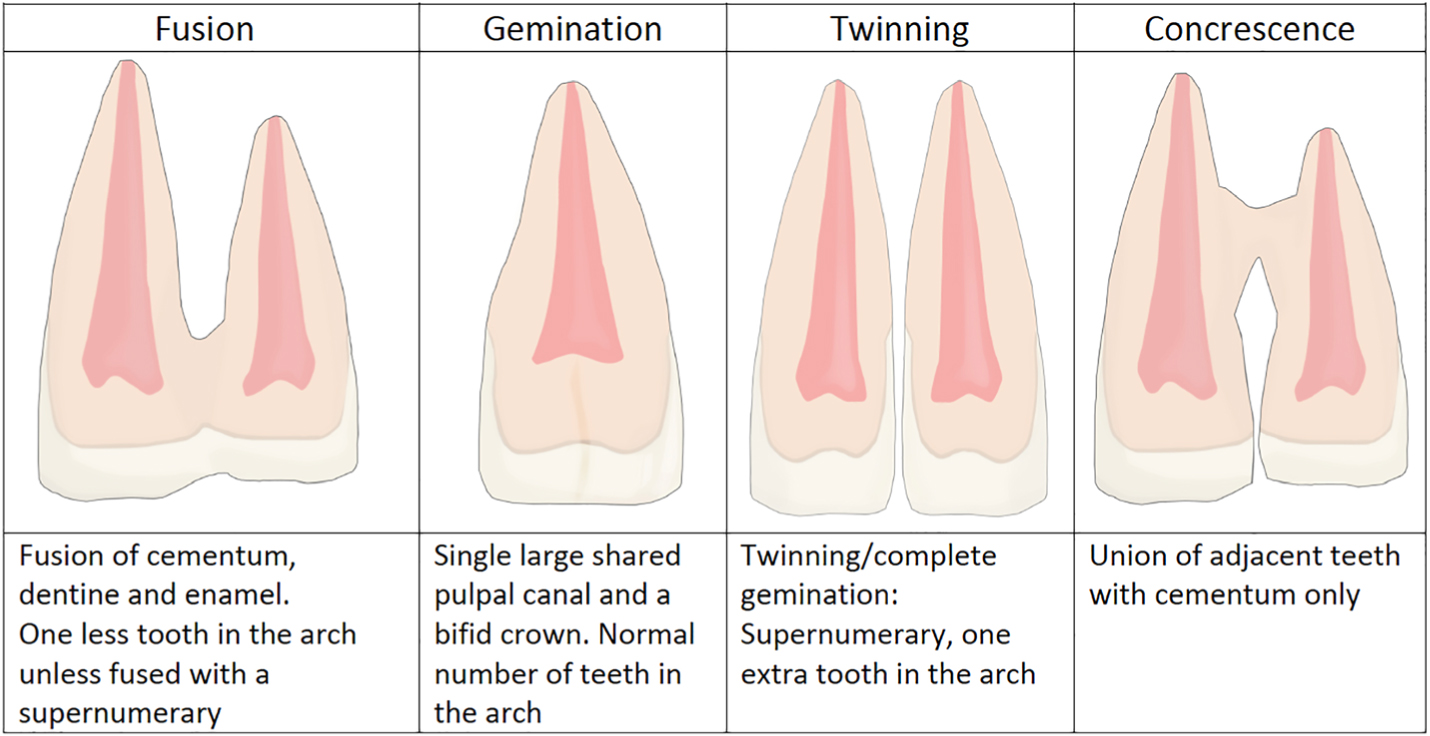
Fusion is defined as the joining of two developing tooth germs, resulting in a single enlarged tooth structure.5 When the fusion process takes place, the entire length of the teeth may be involved, in which case cementum, dentine and enamel are shared, resulting in one less tooth in the arch.5 Gemination is classed as the budding of a second tooth from a single tooth germ and usually one root canal is present, resulting in a single tooth with a bifid crown and a normal number of teeth in the arch.6
Concrescence is where the fusion process occurs after the developmental stages. This is a twinning anomaly characterized by the union of two or more teeth by cementum only. This is thought to arise as a result of injury to the teeth, crowding and resorption of the interdental bone so that the root faces are in approximate contact. Considering that this occurs after root development, concrescence is technically not a developmental anomaly.7Figure 1 illustrates the difference in relation to the enamel, dentine, pulp and cementum for each dental anomaly.
Figure 1. Dental anomalies: fusion; gemination;, twinning; and concrescence.
Double teeth pose a number of management issues for the clinician and a multidisciplinary approach should be sought. Commonly, the double tooth is seen in the anterior region and presents an aesthetic problem due to asymmetry associated with the incisal notch, central groove and possible crowding. Clinically, the extension of the fissure or union line extends subgingivally, increasing the risk of caries and local periodontal problems.
A clinical protocol for double teeth takes into account various presentations of the double tooth.8 The flowchart covers the management of double teeth with single and separate roots, including a treatment option of autotransplantation of a supplemental tooth to replace a double tooth. Taking into account the patient's aesthetic desires and functional needs would dictate the level of intervention required on a case-specific basis.
It is essential to diagnose whether a single canal or separate canals are present, which is not always visible on plain radiographs due to superimposition. Cone beam computed tomography (CBCT) can help determine the true internal anatomy of the root canal and assist with any surgical intervention.9 It is important to limit radiation exposure and, therefore, a small volume scan is usually sufficient.
Multidisciplinary management of a ‘double tooth’
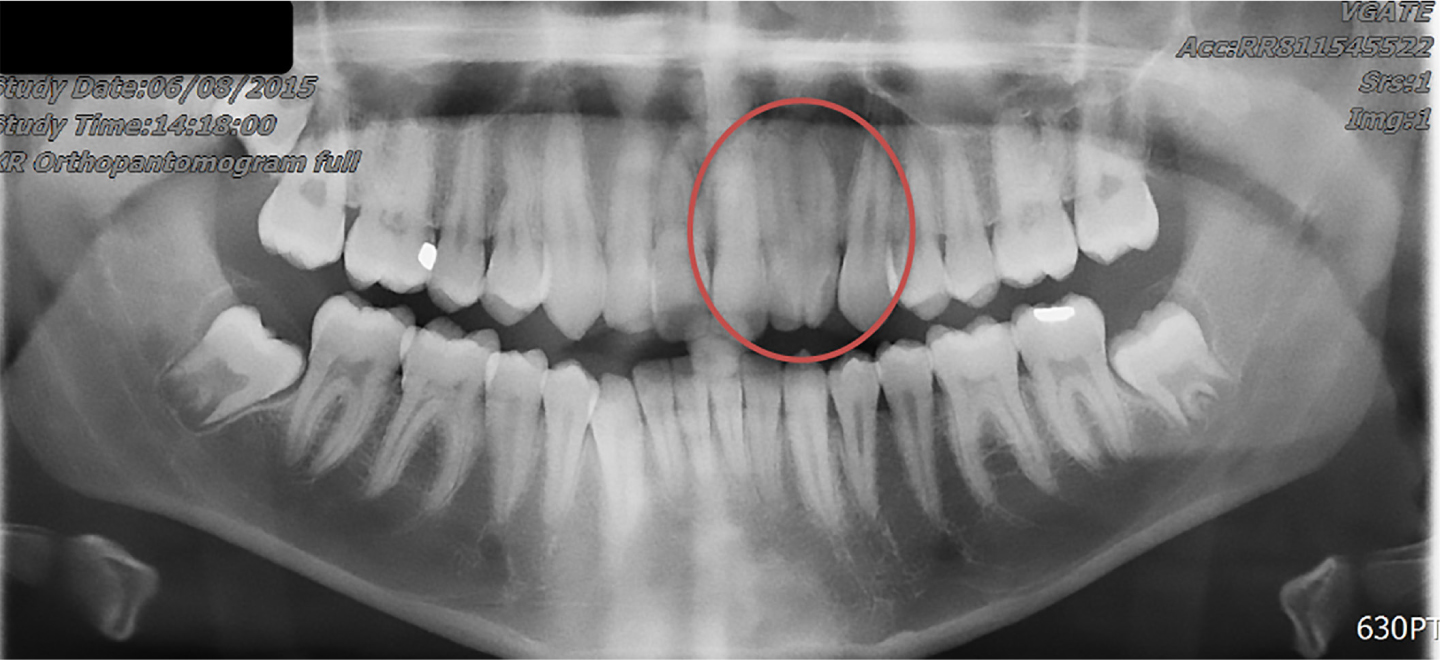
This case reports a 16-year-old male patient referred by his general dental practitioner to the orthodontic department at Leeds Dental Institute with a simple request of ‘I would like a nicer looking tooth.’ The patient presented with the UL2 as a ‘double tooth’. Based on the patient having the normal number of teeth in the arch and clinically noticeable developmental anomaly of the UL2, a provisional diagnosis of the UL2 fused with a supernumerary was made (Figure 2) A multidisciplinary team, including orthodontic and restorative specialists initially assessed the patient. It was important to develop a definitive diagnosis, therefore further investigations were carried out, including an orthopantomograph (Figure 2) and a small volume CBCT (Figure 3).
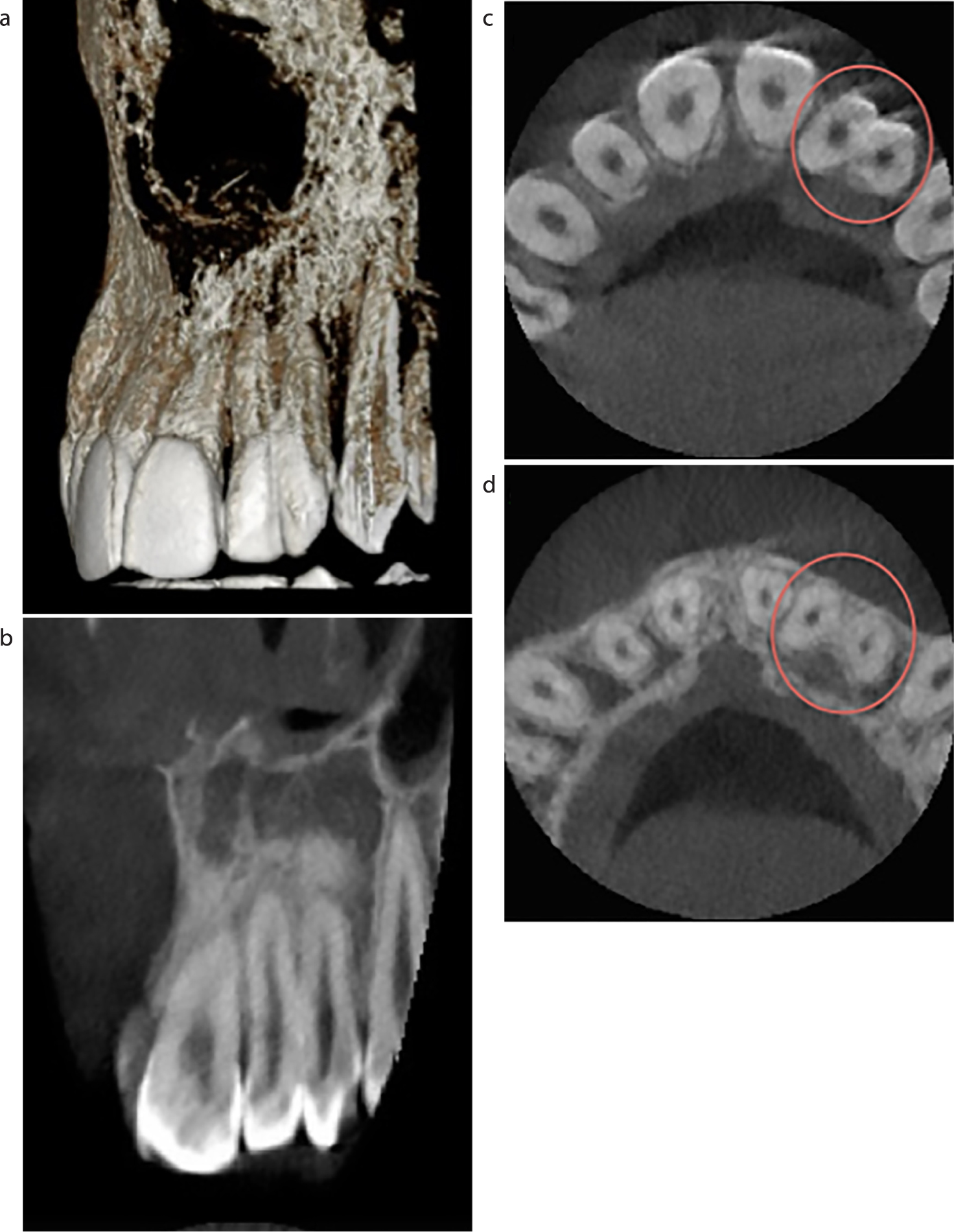
Figure 2. Orthopantomogram of tooth at presentation.Figure 3.
(a–d) CBCT of the tooth at presentation.
The CBCT confirmed the original diagnosis as a case of fusion (fused cementum, dentine and enamel) of the UL2 with a supernumerary. The patient was provided with treatment options along with the limitations of each:
Camouflage using resin composite;
Surgical division of the UL2 and extraction of the distal portion followed by orthodontic space alignment and composite camouflage;
Extraction of UL2, orthodontic space alignment and replacement with resin-retained bridge or implant.
Option 1 would not achieve the correct symmetry and tooth dimensions required to adequately mask this anomaly. Option 2 was chosen as the less invasive option to achieve the patient's desired outcome while knowing that option 3 could be explored if option 2 were to fail.
The definitive treatment plan involved sectioning the UL2 and removal of the distal portion of crown and root, followed by composite augmentation of UL2. Fixed upper and lower orthodontic appliances were required during the final stage to align his arches.
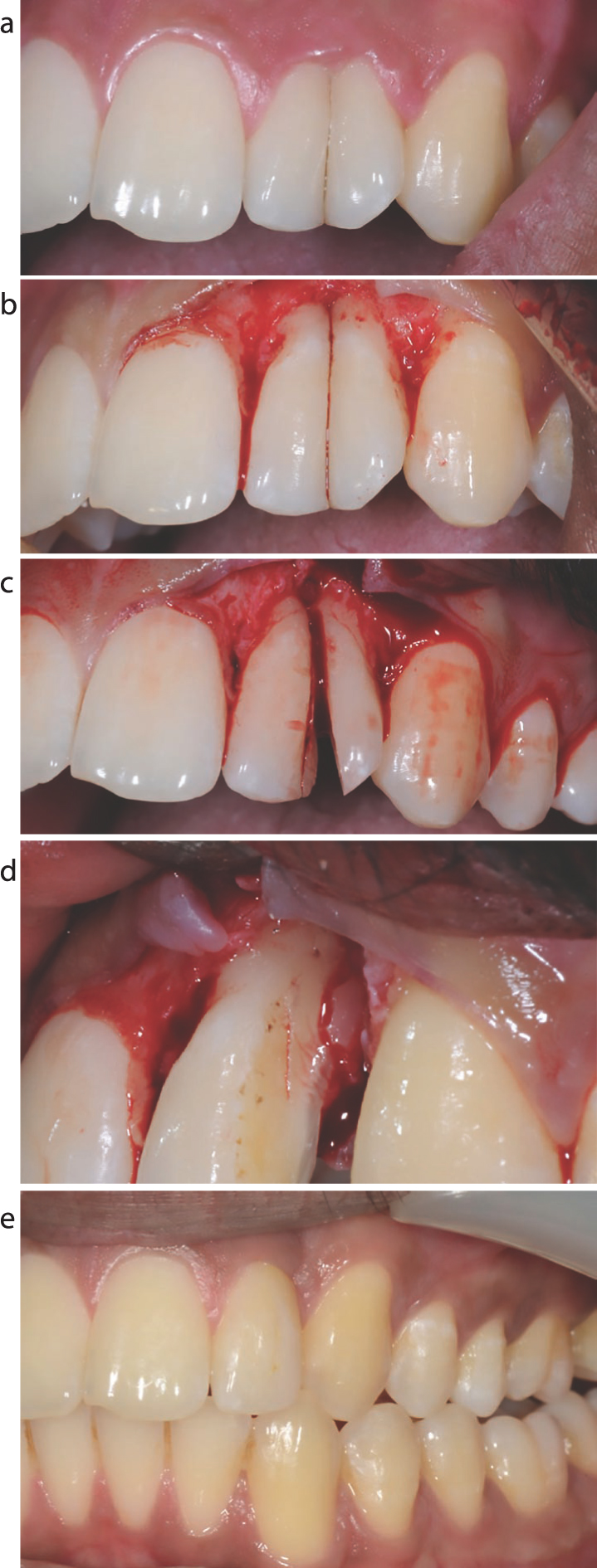
The surgical intervention was carried out under local anaesthetic with full aseptic precautions. A full-thickness mucoperiosteal envelope flap was raised to expose the extent of the fissure line (Figure 4b). Taking into account the removal of the distal portion of the UL2, the surgical fissure bur was kept distal to the fissure line (Figure 4c). This allowed the clinician to smooth up to the fusion line with a diamond bur, producing a smooth contour for future composite augmentation (Figure 4d). Following surgical intervention, the site was left to heal with 5-0 monofilament, absorbable sutures (Serafast, Serag-Wiessner, Germany). On review of the site, the UL2 was built up using composite resin aided by a wax-up and palatal memosil guide. The restorative phase of treatment was now complete. The orthodontic team continued with upper and lower fixed orthodontic appliances 12 weeks after the surgical intervention, with the result shown in Figure 4e.
Figure 4.
(a) Pre-operative view showing the UL2 fusion with supernumerary. (b) Raised full thickness mucoperiosteal envelope flap. (c) Sectioned distal portion of crown and root at fusion line. (d) Remaining mesial portion of UL2 with no pulpal exposure. (e) Final result. UL2 composite augmentation and orthodontic alignment.
On reflection, the patient's desires were met in a timely manner. In this case, we benefited from the small volume CBCT, which displayed pulpal anatomy and root thickness, providing the operator with information to produce a successful outcome. Surgical intervention coupled with orthodontic movement of a tooth can increase the risk of the UL2 losing vitality, developing root resorption or becoming ankylosed. It would be important to monitor this tooth using sensibility tests and radiographs to assess for loss of vitality, apical pathology and resorption, which may require endodontic intervention in the future.
Discussion
The aetiology of the double tooth is unclear due to the inability to witness embryological changes at the time of tooth development. Tooth development commences with thickening of the dental epithelium to form the dental lamina, followed by the bud, cap and bell stages of tooth morphogenesis. Abnormalities caused by mutations have been shown to affect tooth formation in transgenic mice.10 The genes identified give rise to a number of dental anomalies of size, shape, quality and quantity defects of enamel and dentine, and the number of teeth. However, gene mutations have not been identified for the ‘double tooth’. This case does not fall into the precise category of gemination or fusion owing to the patient having a normal number of teeth present, and separate root canals. However, considering the extension of the buccal groove, separation of roots and pulp systems, it could be appropriately classified as an atypical case of dental fusion of the UL2 with a supernumerary.
Summary
The initial presentation of a double tooth can range from an aesthetic concern, as with this case, to a symptomatic situation where caries, periodontal disease or apical infection are involved. The patient's concerns, expectations and level of acceptable treatment intervention should help to guide the clinician into the appropriate treatment plan. Managing the double tooth can have a hierarchy of treatment interventions, from composite masking to surgical, restorative and orthodontic intervention, as with this case. It would be wise to investigate patients' desires to customize this plan, ensuring they understand the limitations of each option.