Darveau RP. Periodontitis: a polymicrobial disruption of host homeostasis. Nat Rev Microbiol. 2010; 8:481-490 https://doi.org/10.1038/nrmicro2337
Hajishengallis G, Liang S, Payne MA Low-abundance biofilm species orchestrates inflammatory periodontal disease through the commensal microbiota and complement. Cell Host Microbe. 2011; 10:497-506 https://doi.org/10.1016/j.chom.2011.10.006
Needleman I, Suvan J, Moles DR, Pimlott J. A systematic review of professional mechanical plaque removal for prevention of periodontal diseases. J Clin Periodontol. 2005; 32:229-282 https://doi.org/10.1111/j.1600-051X.2005.00804.x
Tonetti MS, Jepsen S, Jin L, Otomo-Corgel J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: a call for global action. J Clin Periodontol. 2017; 44:456-462 https://doi.org/10.1111/jcpe.12732
Ismail AI, Lewis DW, Dingle JL. Prevention of periodontal disease. Canadian Task Force on the Periodic Health Examination. 1994; 420-431
Glossary of periodontal terms, 3rd ed. Chicago, Ill: American Academy of Periodontology; 1992
Frame PS, Sawai R, Bowen WH, Meyerowitz C. Preventive dentistry: practitioners' recommendations for low-risk patients compared with scientific evidence and practice guidelines. Am J Prev Med. 2000; 18:159-162 https://doi.org/10.1016/s0749-3797(99)00138-5
Tugnait A, Clerehugh V, Hirschmann PN. Use of the basic periodontal examination and radiographs in the assessment of periodontal diseases in general dental practice. J Dent. 2004; 32:17-25 https://doi.org/10.1016/S0300-5712(03)00126-X
Lovdal A, Arno A, Schei O, Waerhaug J. Combined effect of subgingival scaling and controlled oral hygiene on the incidence of gingivitis. Acta Odontol Scand. 1961; 19:537-555 https://doi.org/10.3109/00016356109043406
Suomi JD, Greene JC, Vermillion JR The effect of controlled oral hygiene procedures on the progression of periddontal disease in adults: results after third and final year. J Periodontol. 1971; 42:152-160 https://doi.org/10.1902/jop.1971.42.3.152
Worthington HV, Clarkson JE, Bryan G, Beirne PV. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2013; https://doi.org/10.1002/14651858.CD004625.pub4
Jones CL, Milsom KM, Ratcliffe P Clinical outcomes of single-visit oral prophylaxis: a practice-based randomised controlled trial. BMC Oral Health. 2011; 11 https://doi.org/10.1186/1472-6831-11-35
Hefti AF, Preshaw PM. Examiner alignment and assessment in clinical periodontal research. Periodontology 2000. 2012; 59:41-60
Ramsay CR, Clarkson JE, Duncan A Improving the Quality of Dentistry (IQuaD): a cluster factorial randomised controlled trial comparing the effectiveness and cost-benefit of oral hygiene advice and/or periodontal instrumentation with routine care for the prevention and management of periodontal disease in dentate adults attending dental primary care. Health Technol Assess. 2018; 22:1-144 https://doi.org/10.3310/hta22380
Lembariti BS, van der Weijden GA, van Palenstein Helderman WH. The effect of a single scaling with or without oral hygiene instruction on gingival bleeding and calculus formation. J Clin Periodontol. 1998; 25:30-33 https://doi.org/10.1111/j.1600-051x.1998.tb02360.x
Lamont T, Worthington HV, Clarkson JE, Beirne PV. Routine scale and polish for periodontal health in adults. Cochrane Database Syst Rev. 2018; 12 https://doi.org/10.1002/14651858.CD004625.pub5
Needleman I, Nibali L, Di Iorio A. Professional mechanical plaque removal for prevention of periodontal diseases in adults – systematic review update. J Clin Periodontol. 2015; 42:S12-S35 https://doi.org/10.1111/jcpe.12341
A Review of the Evidence for the Provision of the Routine Scale and Polish for the Prevention of Periodontal Disease Rachel Birt Claire M Healy Denise MacCarthy Lewis Winning Dental Update 2024 48:3, 707-709.
The routine scale and polish is the most commonly performed treatment procedure in general dental practice. With a large proportion of state dental health expenditure in the UK and Ireland being used to provide ‘routine scale and polish’ treatments, it is necessary to establish the true value of this treatment for patients. In this narrative review, we discuss the available evidence regarding provision of the routine scale and polish. Based on the available studies, there is little evidence to support the use of the routine scale and polish alone for the prevention of periodontal disease.
CPD/Clinical Relevance: This paper evaluates the evidence surrounding the routine provision of scaling and polishing for the prevention of gingivitis and periodontitis.
Article
Dental plaque has been shown to play a central role in the development of periodontal diseases (PDs) including gingivitis and periodontitis.1,2,3 Oral hygiene instruction (OHI) should play a primary role in the prevention and management of periodontal disease.4 Scaling and polishing (S&P) by dental professionals is a treatment intended to complement the patient's own plaque control and is not intended to act as a replacement.5 Studies suggest that calculus deposits are not significant in the development of periodontal diseases; however, it has been suggested that calculus does serve as a reservoir for bacteria and potentially minimizes the effectiveness of personal oral hygiene measures (Figure 1).6
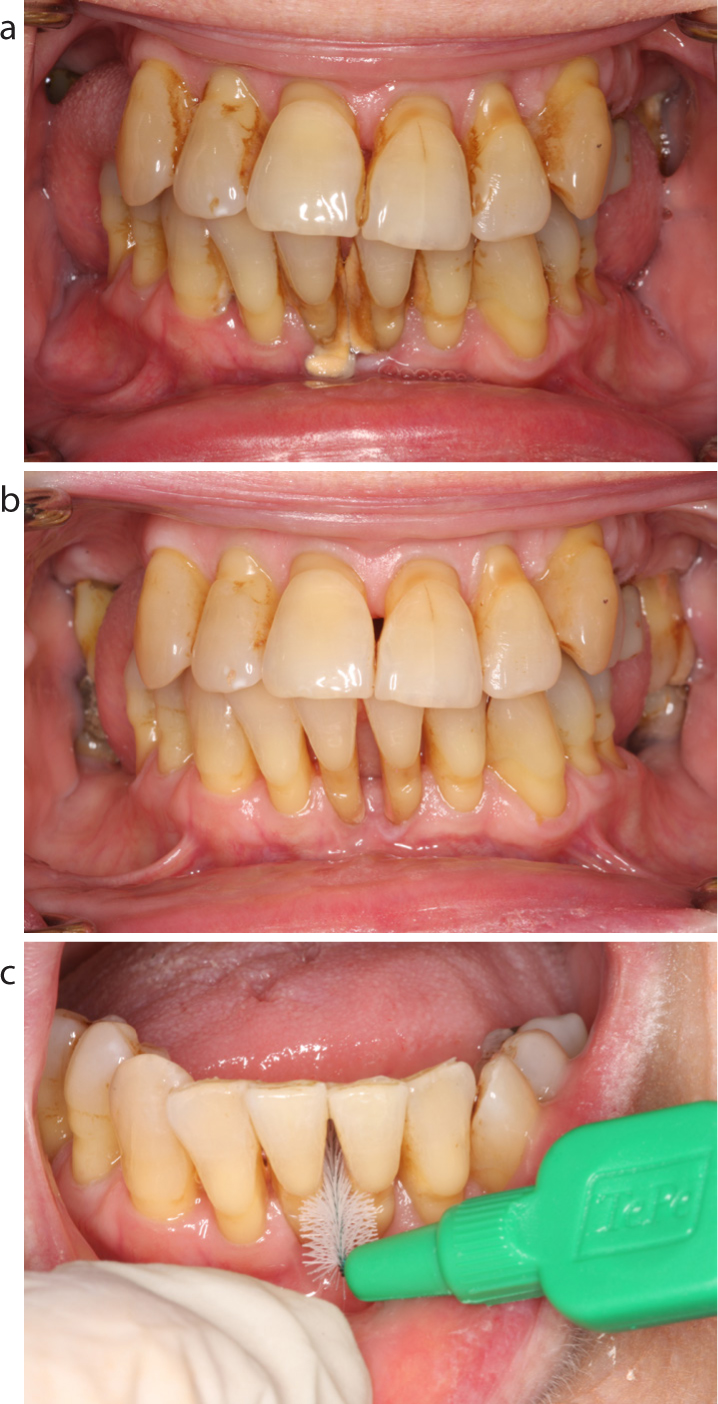
Figure 1.
(a) A 72-year-old female patient (with evidence of previous but now stable periodontitis) presents with gross calculus deposits in the lower incisor area. (b) Removal of calculus via a routine scale and polish, (c) permits better access for personal oral hygiene measures.
Presently there is no standard definition for the term ‘scale and polish’, which is also referred to as oral prophylaxis, professional mechanical plaque removal or periodontal instrumentation. The American Academy of Periodontology defines scaling as the ‘instrumentation of the crown and root surfaces of the teeth to remove plaque, calculus and stains from these surfaces’.7
Routine S&P is commonly recommended by general dental practitioners as a preventive or prophylactic treatment for all patients, regardless of their risk for developing PD (Figure 2). A survey of general dentists in New York revealed that 86% of respondents recommended 6-monthly S&P for all patients as a preventative measure, even if these patients were considered to be low risk for developing PD.8
Figure 2. A 39 year old female patient attends having not previously attended a dentist in the last 5 years. The patient has no significant risk factors for the development of periodontal disease. There are some minor calculus deposits in the lingual area of the lower incisor region, however actual plaque deposits are minimal and essentially the patient has a healthy periodontium. In such a case it is unclear whether the recommendation of a routine scale and polish actually offers a benefit in the prevention of future periodontal disease.
In the UK, the majority of practitioners use the Basic Periodontal Examination (BPE) to screen for PD.9 The BPE was first developed by the British Society of Periodontology in 1986 and has recently been updated.10 Although its use is primarily intended as a screening tool, it does provide basic guidance on treatment need. The presence of supra-or sub-gingival calculus/overhangs with periodontal pocketing <3.5 mm indicates a score of ‘2’ in the BPE. This doesn't necessarily indicate a diagnosis of gingivitis, but carries a treatment recommendation of ‘oral hygiene instruction and removal of plaque retentive factors including all supra- and sub-gingival calculus’, most commonly delivered as a S&P (Figure 3). The Periodontal Screening Record11 (PSR) is a variation on the BPE, originally developed in 1992 by the American Academy of Periodontology and American Dental Association. The same clinical presentation as that described derives a score of ‘2’ in the PSR, and also carries the same treatment recommendation as described in relation to a BPE score of ‘2’.
Figure 3. A 64-year-old patient who, at routine annual examination, presented with a BPE/PSR score of 2 in the lower anterior sextant. Routine scaling and polishing is indicated to remove all plaque, calculus, and staining deposits: (a) before; (b) after.
In 2009/2010 44.1% of adult courses of dental treatments in the National Health Service (NHS) in England included a scale and polish, equating to 12 million courses of treatment.12 This has remained consistent, with 2017/2018 figures showing that 45.7% of adult clinical treatments provided by the NHS in England were S&P treatments.13 In 2016/2017 the NHS in Scotland provided 2.3 million S&P treatments, costing the NHS £33.2 million.14 In Ireland the Treatment Benefit scheme allows individuals who are making PRSI (Pay Related Social Insurance) contributions to avail of a free oral examination and a subsidised S&P treatment once per calendar year, regardless of risk of periodontal disease.15 Approximately 2.5 million people are eligible for treatment under this scheme in Ireland. In 2018, a total of 804,735 claims were made under this scheme for exam S&P treatments, amounting to a cost of €46.9 million to the state.16
This aim of this narrative review was to investigate the validity of the current routine practice of S&P treatments for PD prevention.
Historical perspective
A randomized controlled trial (RCT), conducted in the US Air Force Academy, investigated the effectiveness of preventative periodontal treatments in 713 participants over a 4-year period.17,18 Three standardized techniques involving S&P were investigated: a 50-minute preventive periodontal treatment; a preventive treatment given in two 30-minute appointments; and a preventive periodontal treatment given in a single 30-minute appointment. Controls groups involving no OHI were also investigated. The study found that the periodontal status of all patients improved in the first 2 years. The mean gingival and plaque index scores for all groups improved from commencement to completion of the trial. All participants reached a plateau with regard to improvement in periodontal status after the 2-year mark with minimal or no improvement recorded thereafter. Groups who received OHI showed the greatest improvement in plaque control. Groups who received S&P at 3- or 6-monthly intervals exhibited fewer participants with loss of attachment. The 12-monthly group who received no OHI had a significantly reduced improvement in periodontal status than participants in the other groups. Calculus prevalence decreased for all groups over the 46-month period.
Classic studies such as this,19,20 may have perpetuated the notion that preventive periodontal procedures (including routine S&P) were essential in order to maintain periodontal health. A Cochrane review in 201321 found this particular trial to have a high risk of bias as the method of randomization was unclear, which may have resulted in selection bias. Also, insufficient information was provided in relation to allocation concealment and attrition bias with 33% of subjects not followed-up for the duration of the trial. Baseline imbalances were present with calculus scores noted to be lower in the control groups. Due to the above shortcomings and the young population examined, which is not representative of the general population, the level of evidence reported to support routine S&P to control gingivitis and periodontitis is now considered low quality.
More recent trials conducted in general dental practice
An RCT in 2011 investigated the effectiveness of routine S&P conducted in general dental practices in England, for the prevention and control of gingivitis over a 2-year period.22 In total, 307 adults with BPE codes <3 were randomly assigned to three groups (6-month, 12-month, or 24-month interval between S&P). The primary outcome measure was gingival bleeding with the hypothesis that 6-monthly S&P would result in lower prevalence than 12-month or 24-month frequency. This trial found bleeding scores increased in all groups from baseline to follow-up, with no significant association noted between frequency of S&P and bleeding prevalence. No significant differences were noted in the prevalence of plaque or calculus for patients in the different treatment groups. The amount of calculus present on the mandibular anterior teeth was noted to increase with an increase in the time interval between S&P visits. This increase in the amount of calculus was found to be statistically significant. However, it was not deemed to be a clinically significant increase as it was so minimal that it would not be possible to measure these changes with standard dental instruments. This trial does not provide evidence to support the provision of routine S&P to control gingivitis. The study also examined patient perceptions of the benefits of S&P treatment and OHI concluding that the 71% of patients believed S&P treatment should be provided at least every 6 months. A ‘high level of oral cleanliness’ was more frequently reported by patients in the 6-monthly treatment group compared to the other treatment groups. There are several limitations to this study. It is generally accepted that methods of assessing gingival inflammation that provoke gingival bleeding do not allow for repeated assessment.23 Periodontal status is best assessed long term by measuring probing pocket depths and clinical attachment levels, rather than presence or absence of bleeding. The use of clinical measurements, however, would need a longer period of observation to detect meaningful change than the 24-month duration in this study. Changes in pocket depth or attachment level of <2 mm could be due to measurement error, so would also require a larger sample size to detect changes. A further limitation relates to the fact that patients with BPE scores of ≥3 were excluded and those who developed BPE scores ≥3 were removed from the trial, so no conclusion on the effectiveness of S&P for the control of periodontitis can be made. The 2013 Cochrane review deemed this RCT to have an unclear risk of bias due to these withdrawals.21
A large RCT comparing the effectiveness and cost–benefit of oral hygiene advice and/or periodontal instrumentation (S&P) for the prevention and management of PD was reported in 2018.24 The trial was conducted in 63 dental practices across Scotland and England. There were 1877 participants and follow up was for 3 years. Patients were randomly assigned to groups who either received no periodontal instrumentation, periodontal instrumentation at 6-monthly intervals (current practice) or periodontal instrumentation at 12-monthly intervals. Patients included in this trial had healthy periodontium, gingivitis or mild periodontitis (BPE 0,1,2,3). The trial found no evidence of a difference in gingival inflammation/bleeding between patients in the no periodontal instrumentation group and patients in the 6-monthly PI group. Similarly, there was no difference between the 6-monthly and 12-monthly periodontal instrumentation groups. There was also no evidence of a difference between personalized and routine oral hygiene advice. This study concluded that there was no benefit in providing 6- or 12-monthly routine periodontal instrumentation over not providing this treatment. However, the results of patient-centred outcomes and willingness-to-pay analysis showed that participants did value the interventions and were willing to pay for both periodontal instrumentations and oral hygiene advice. Again, there are limitations to this trial. The primary outcome of the trial was gingival inflammation measured as bleeding on probing, and therefore the same limitations as previously discussed apply. The observation period was longer than the previous trial, at 3 years, but this may still be an insufficient observation period to detect the protective benefit of routine S&P. As the trial was conducted across Scotland and England, there are some limitations with regard to the health economic analysis because both countries have different contracts for delivery of care. A further limitation is that S&P was also provided to patients on request, regardless of which treatment group they were assigned to. No record was kept as to why additional S&P was provided.
Additional considerations: the importance of repeat oral hygiene instruction
A split-mouth RCT in Tanzania in 1998 investigated the effect of single scaling, with or without OHI, on gingival bleeding and calculus formation.25 Participants were chosen from a preliminary study conducted by the same author that identified 50 students from three schools with the highest calculus scores, but who did not have periodontal pockets greater than 4 mm. Baseline examinations revealed no differences between the calculus or bleeding scores between the groups. The OHI given in this trial did not result in significant reductions in bleeding or calculus scores, indicating that OHI without reinforcement did not improve the gingival condition. Scaled sites had significantly lower calculus scores than non-scaled sites throughout the 22 months. Scaled sites had 20% lower bleeding scores than non-scaled sites 6 months after scaling and this difference remained for the duration of the study. The authors of this study concluded that the observed reduction in gingival bleeding was due to the scaling because there was no improvement in OH. It can be concluded that the effect of single scaling alone on the gingival condition was minimal and the effect of a single OHI session negligible.
An RCT in Denmark (1977) investigated the effect of professional cleaning, applied at 4-weekly intervals, on the periodontium of patients who were in periodontal maintenance therapy.26 At the beginning of the trial phase no statistically significant differences were present between control and experimental quadrants in relation to plaque and gingival indices and average loss of attachment. The 1-year examination revealed no statistical difference for clinical attachment loss between test and control teeth. Calculus deposits were recorded on 0.028% of tooth surfaces in the test units and 0.04% in the control units. At the final examination, 1% of the experimental and 3% of the control units had a gingival index score of 2, indicating gingival bleeding. Additionally, 71% of the experimental and 69% of the control units had a gingival index score of 0. At the final examination 11% of the experimental and 12% of the control units displayed plaque index19 scores of 2, indicating visible plaque. Plaque index scores of 0 were found in 68% of both the control and experimental unit. This study suggests that it was not the professional cleaning per se that was responsible for the improved periodontal condition and high level of oral hygiene displayed in the control and test units throughout this trial. Frequent recall intervals appeared to motivate patients to develop and maintain a high level of oral hygiene, which improved the periodontal status for the control and test units.
Current consensus on the routine provision of scale and polish treatments
A Cochrane review on the effectiveness of routine S&P was published in December 2018.27 This review studied RCTs conducted in general dental practices that investigated the effectiveness of routine S&P for the prevention and control of PDs and is based on the two studies previously disucussed.22,24 The review investigated effects of S&P treatments provided at regular intervals of 6 or 12 months and compared this to no S&P treatment. The review confirmed the findings of the individual studies in that there was a high certainty of evidence to suggest that there was little or no difference in gingivitis or probing depths between groups of patients who were routinely provided with S&P treatments compared to those who received no treatment. It was concluded that participants who were receiving scheduled S&P treatments reported higher levels of oral cleanliness than those who do not; however, there is currently no evidence of a difference in oral health-related quality of life.
Needleman and colleagues28 conducted a systematic review as part of the XI European Workshop of Periodontology ‘Effective Prevention of Periodontal and Peri-implant diseases’.29 The aim of the systematic review was to determine the effect of professional mechanical plaque removal (including S&P/oral prophylaxis) on clinical and patient-reported outcomes related to the primary prevention of PDs. The review found that there was a moderate strength of evidence to suggest no additional benefit to plaque and gingival bleeding outcomes from professional mechanical plaque removal over that achieved by repeated and thorough OHI. In fact, the review suggested, repeated, thorough OHI can achieve a similar benefit to repeated professional mechanical plaque removal. There was a lack of data to make a conclusive statement regarding the prevention of periodontitis.
Conclusion
In general, there is a lack of evidence to support the provision of the routine S&P to prevent gingivitis and periodontitis, at least in the short term. Moreover, the available evidence tends to suggest that provision of the routine S&P offers no additional benefits in terms of plaque and bleeding indices than those which are achieved by repeated and thorough OHI alone. Longer-term studies may be required to fully establish the benefit of routine S&P. Indeed, beneficial effects of routine S&P may not occur directly through the S&P itself, but may occur indirectly through encouraging better dental attendance, improved relationship with dental professionals, and as a tool to encourage and motivate patients to develop and maintain a high level of oral hygiene. A longitudinal study investigating benefits of routine dental visits, found routine attenders had better-than-average oral health, fewer had teeth missing due to caries, and they had lower mean decayed teeth and DMFS scores.30 The longer routine attendance was maintained in this study, the stronger the effect.
The S&P is a procedure regularly provided by dental professionals. The large proportion of dental health budgets spent on the routine S&P in both the UK and Ireland, highlights the importance of establishing its true value both from a health perspective to the individual patient and also fiscally to the wider public. At a population level, it may be more effective to target the use of future dental health budgets to the ‘at risk’ population rather than the population as a whole. The lack of evidence regarding such models of care highlights the need for further studies. These studies should be in the form of well-conducted randomized controlled trials, carried out in general dental practice with an adequate follow-up period. Trials should include participants with both a healthy periodontium as well as more established PD. A greater emphasis on risk assessment at a subject level, as well as at a site level, may be a more effective way of determining who may benefit from preventive periodontal procedures.