Kahler B, Hu JY, Marriot-Smith CS, Heithersay GS Splinting of teeth following trauma: a review and a new splinting recommendation. Aust Dent J. 2016; 61:(Suppl 1)59-73
DiAngelis AJ, Andreasen JO Figure 4. Cone-beam CT images with (a) sagittal and (b) axial, views of UR1 and UL1, and (c) peri-apical radiograph 4 years after the dental trauma. January 2021 Dental Update 45 Paediatric Dentistry Ebeleseder KA et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012; 28:2-12
Andreasen JO, Andreasen FM, Mejare I, Cvek M Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation. Dent Traumatol. 2004; 20:192-202
Andreasen JO, Andreasen FM, Mejare I, Cvek M Healing of 400 intra-alveolar root fractures. 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and antibiotics. Dent Traumatol. 2004; 20:203-211
Hinckfuss SE, Messer LB Splinting duration and periodontal outcomes for replanted avulsed teeth: a systematic review. Dent Traumatol. 2009; 25:150-157
Borrie F, Bearn D Early correction of anterior crossbites: a systematic review. J Orthodont. 2011; 38:175-184
Wiedel AP, Norlund A, Petren S, Bondemark L A cost minimization analysis of early correction of anterior crossbite-a randomized controlled trial. Eur J Orthodont. 2016; 38:140-145
Miaoto CB, Marques LS, Abreu LG, Paiva SM Comparison of two early treatment protocols for anterior dental crossbite in the mixed dentition: a randomized trial. Angle Orthod. 2018; 88:144-150
Kindelan SA, Day PF, Kindelan JD Dental trauma: an overview of its influence on the management of orthodontic treatment. Part 1. J Orthodont. 2008; 35:68-78
Amat P A myofunctional approach to treatment of anterior cross bites. J Dentofacial Anom Orthodont. 2009; 12:182-191
Tzatzakis V, Gidarakou I Correction of anterior crossbite using occlusal build-ups. J Clin Orthodont. 2007; 41:393-397
Management of Anterior Crossbite due to Splinting for Dental Trauma: A Case Report with 4-year Follow-up Camila Corral Nuñez Andrea Veliz Ramirez Sigrid Schade Cristian Navarrete Hans von Mühlenbrock Braulio Catalan Gamonal Aws Alani Dental Update 2024 48:1, 707-709.
Authors
Camila CorralNuñez
BDS, MClinDent, PhD, Child and Adult Dental Traumatology Clinic, Department of Restorative Dentistry, Faculty of Dentistry, Universidad de Chile, Santiago, Chile.
DS, Paediatric Dentistry Specialist, Child and Adult Dental Traumatology Clinic, Department of Paediatric Dentistry and Orthodontics, Faculty of Dentistry, Universidad de Chile, Santiago, Chile.
BDS, Paediatric Dentistry Specialist, Child and Adult Dental Traumatology Clinic, Department of Paediatric Dentistry and Orthodontics, Faculty of Dentistry, Universidad de Chile, Santiago, Chile.
BDS, Child and Adult Dental Traumatology Clinic, Department of Paediatric Dentistry and Orthodontics, Faculty of Dentistry, Universidad de Chile, Santiago, Chile.
This report describes the sequelae and subsequent management of a 7-year-old boy who failed to attend follow-up visits after a dental trauma and was initially managed with an active splint. The splint was maintained for 9 months, resulting in an anterior cross-bite, caused by retroclination of the upper incisors. The splint was removed and occlusal build-ups were placed on the molars. Nine months later, the form and shape of the upper dental arch were re-established and the cross-bite was corrected. Four years after the dental trauma, the injured teeth were asymptomatic and had continued root development.
CPD/Clinical Relevance: Splints for dental trauma management should be passive and removed at the requisite time, to avoid the risk of the splint generating a malocclusion.
Article
Splint management for luxated, avulsed, or fractured teeth is a cornerstone of dental trauma management.1,2 Periodontal healing, once a tooth has been repositioned, provides the clinician with a predictable and efficient way to maintain the teeth, thus avoiding the need for complicated and invasive tooth replacement options. In the growing patient, this becomes even more crucial as the patient has yet to fully develop and timely management reduces the burden of treatment throughout the patient's life. Hence, splint therapy is needed, but requires adherence to guidelines and protocols to prevent complications as a result of the splint provision.
In the developing dentition, a concerted effort should be made to maintain pulp vitality and ensure continued root development. This is key as the immature tooth has an immense capacity to heal and continue root development.2 In situations where the pulp loses vitality, the repercussions are severe as the tooth's prognosis diminishes with thin dentine walls and is further compounded and compromised in situations where the root is fractured. In situations where roots are fractured, the remaining tissues have the capacity to heal. The modes through which healing can occur depend on a variety of factors.3,4 Indeed, fractures may present concurrently with other injuries, such as concussion, subluxation, or, in more severe cases, extrusion or lateral luxation of the coronal fragment. Once stabilized, healing can take the form of two broad categories: healing with hard tissue union; or healing with the ingrowth of connective tissue or bone. The former is obviously the more favourable category.5 Something that has changed significantly in the past 20 years is the length of splinting time.1,6 This is relevant as prolonged splinting, which may potentially be caused by failure to follow up, may compromise dentoalveolar development and require further treatment down the line.
In essence, during the growth period, the splint can act as an orthodontic appliance if it is not removed as and when required. The following report presents the case of a child who failed to attend follow-up visits after a dental trauma emergency was managed with an active splint due to a root fracture. The anterior cross-bite that resulted was treated by the use of occlusal build-ups of the posterior teeth. No other appliances were used.
Clinical report
A 7-year-old boy was referred to the Paediatric and Adult Dental Traumatology Clinic Faculty of Dentistry, Universidad de Chile, with a history of paediatric dental trauma caused by an accident on a bicycle. The history revealed that the patient received emergency treatment at a public hospital where UR1 and UL1 were repositioned after a lateral luxation and a composite wire splint was placed. In addition, a diagnosis of horizontal root fracture of the UR1 was made upon radiographic examination. He was advised on gentle tooth brushing, rinsing with chlorhexidine mouthwash and a soft diet. According to the patient's mother, after 1 week, they returned to the same hospital because the splint had detached. The splint was re-bonded and a referral to the Paediatric and Adult Dental Traumatology Clinic Faculty of Dentistry, Universidad de Chile for management was made.
Although a referral was made, the patient failed to attend in a timely manner. The parents gave several reasons for the lack of attendance, including transport difficulties and difficulties with taking a day off to bring their son to the clinic for dental treatment. Nine months after the date of the trauma, the patient attended the clinic.
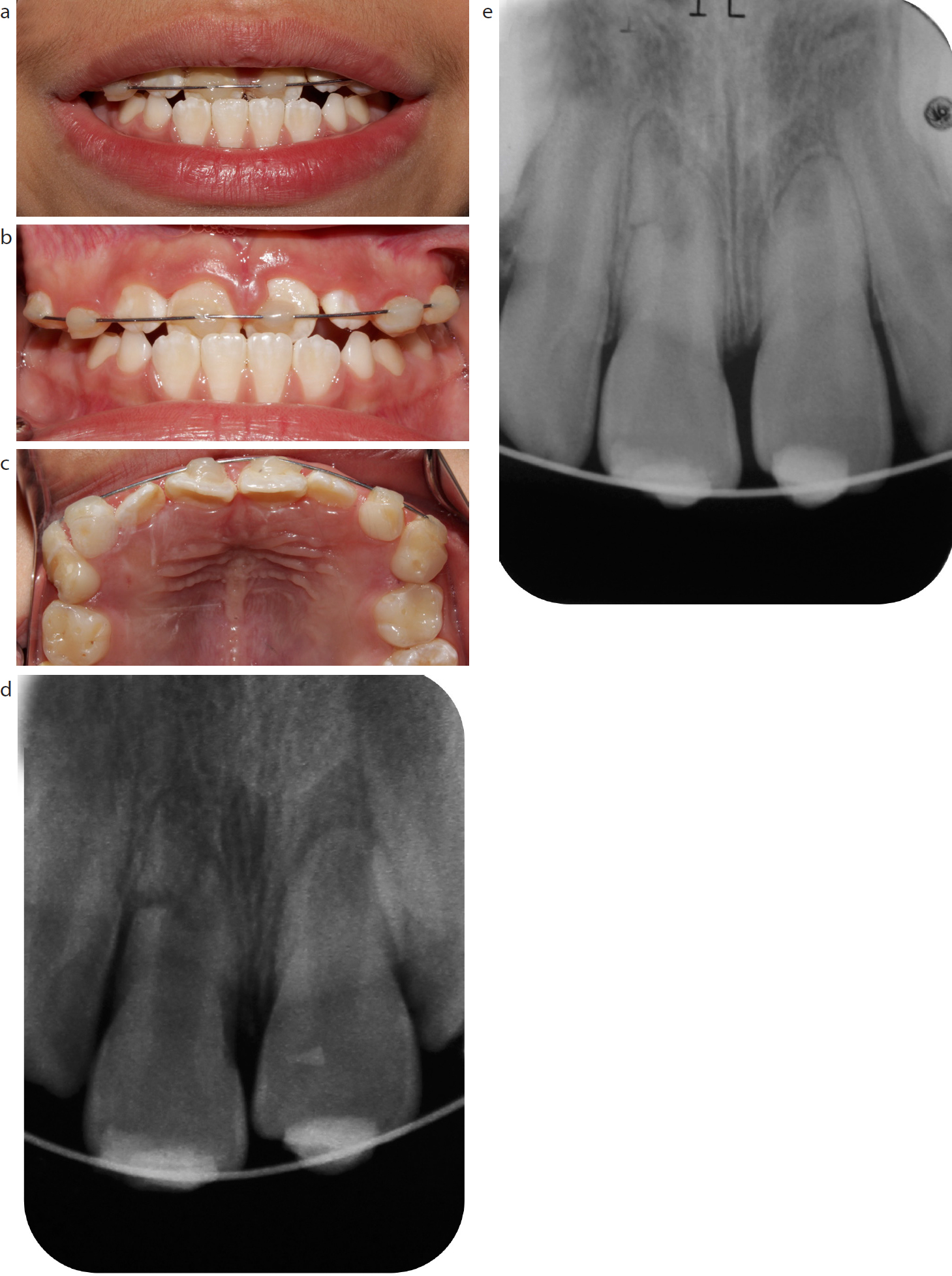
Intraoral examination revealed that the patient was in the mixed dentition stage with erupted permanent incisors and permanent first molars. The patient presented with a wire composite splint bonded to URD, URC, UR1, UL1, ULC, ULD (Figure 1). In the intercuspal position, there was an anterior cross-bite involving UR1 and UL1, and an anterior displacement on closing into centric occlusion was not detected. Deciduous canines and first primary molars had been expanded and the upper permanent incisors appeared to have retroclined as a result of the straight piece of splint wire. The teeth (UR1 and UL1) responded positively to cold stimulus (Endo Ice Hygenic, Coltene), showed physiological mobility and no pain was referred. The parents provided the previous peri-apical radiograph taken at the initial presentation (Figure 1). This radiograph showed that UR1 and UL1 had immature root development and UR1 was root-fractured in the apical third. A new peri-apical radiograph was taken and although the fracture was still evident in the distal root wall of UR1, further root formation was noted.
Figure 1.
(a–d) Clinical views at presentation (a), showing the anterior cross-bite (b) and occlusal view (c). Peri-apical radiograph taken immediately (d) and 9 months (e) after the dental trauma.
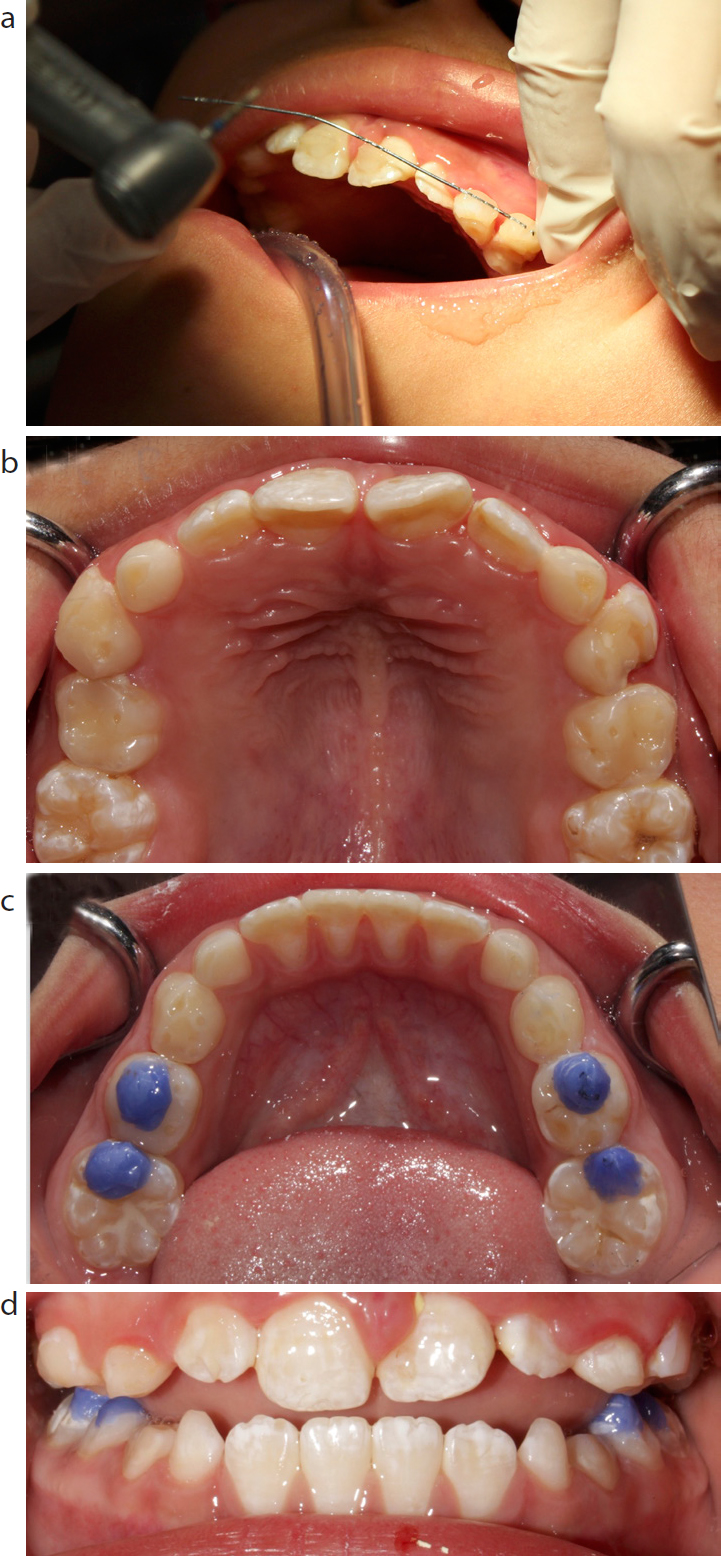
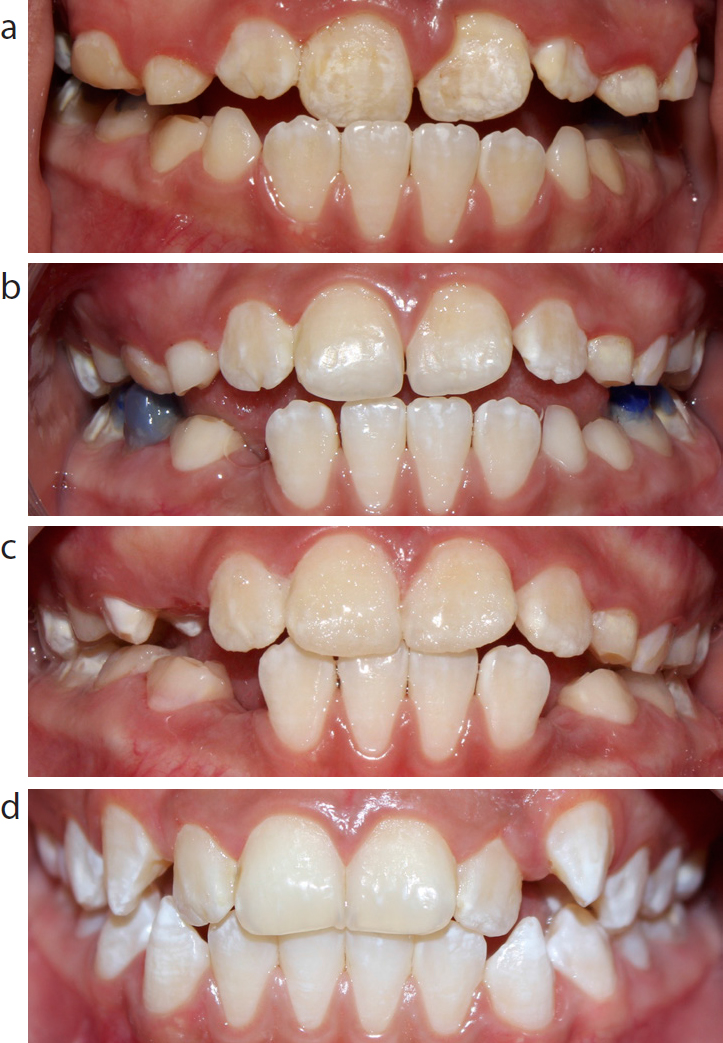
A treatment plan was discussed with the orthodontic specialists in conjunction with the parents. The plan included the immediate removal of the splint, placement of occlusal build-ups with resin composite in the primary molars, and a follow-up (Figure 2). Informed consent was obtained from the parents for the treatment and photography. On splint removal it was noted the wire was still active, that is, it was straight and had not been shaped to the arch (Figure 2a). Blue resin composite build-ups were placed in LRE, LRD, LLD, LLE to open the bite and allow correction of the cross-bite. The patient and parents were scheduled for recall visits on a monthly basis. The pulp and peri-apical tissues of the traumatized tooth were monitored periodically in addition to any changes in occlusion. Intraoral examination revealed gradual changes in the arch and the cross-bite (Figure 3). After 9 months, the cross-bite was corrected, with an overjet of 1 mm and an acceptable maxillary arch shape. The decision was taken to remove the occlusal build-ups and the patient continued his operative dental treatment.
Figure 2.
(a) Removal of active splint. (b) Maxillary arch with quadrangular shape. (c)Occlusal build-ups in lower molars. (d) Frontal view showing the open bite created.Figure 3.
(a) Frontal view after 3 weeks), and (b) after 9 months of the occlusal build-ups, when they were removed. Follow-up visits after (c) 1 and (d) 2 years consecutive to the removal of the build-ups.
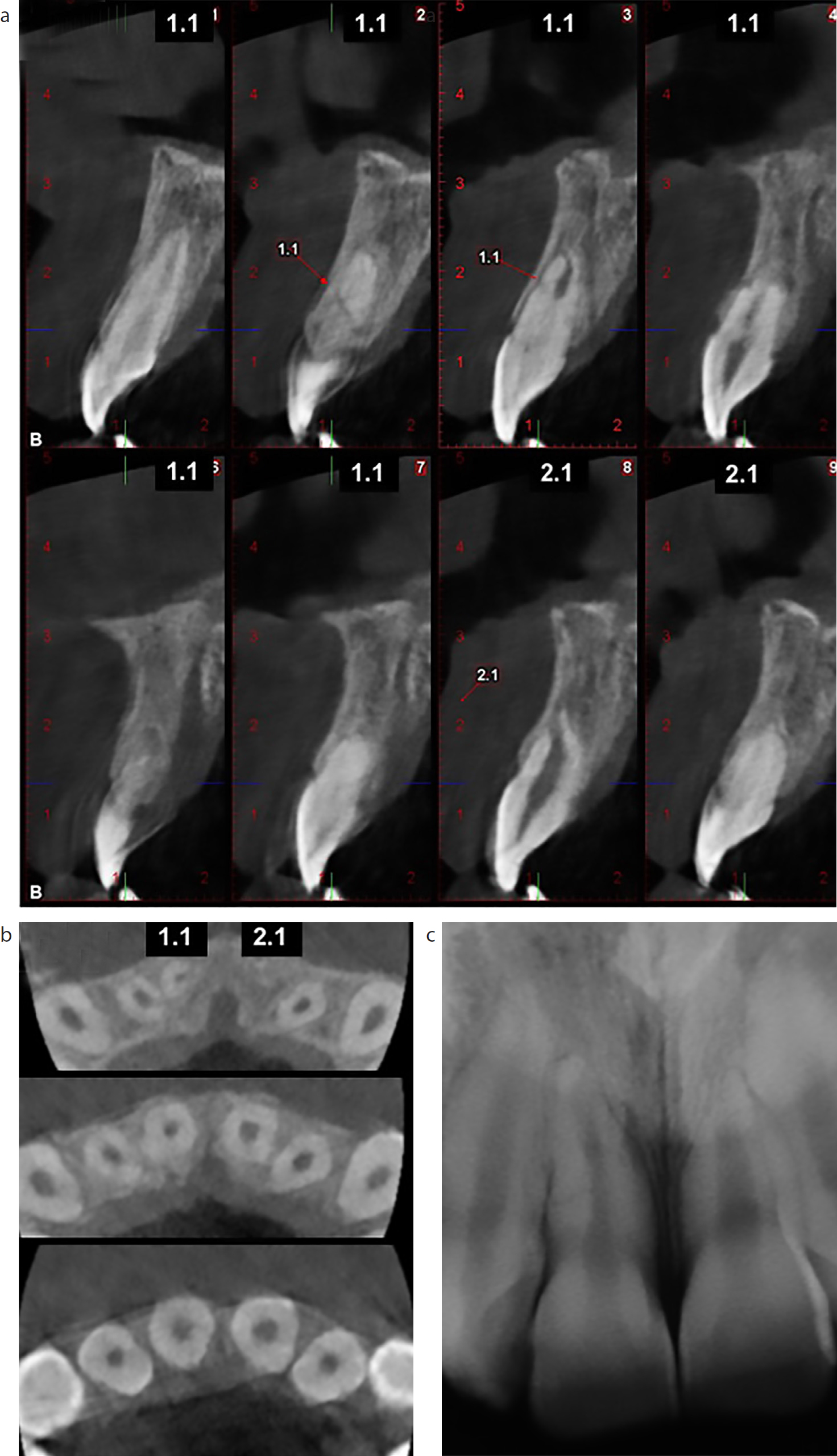
Four years after the dental trauma, the patient presented with a good outcome. Follow-up appointments were performed yearly. At clinical examination, UR1 and UL1 were asymptomatic and responded positively to the sensibility test. Radiographic and cone-beam CT images (Figure 4) indicated that UR1 had continued root development with healing of the root fracture partly through hard tissue, associated with pulp canal space reduction, and that UL1 had continued root development with dentinal wall apposition, although the root length of UL1 was shorter than that of UR1.
Figure 4. Cone-beam CT images with (a) sagittal and (b) axial, views of UR1 and UL1, and (c) peri-apical radiograph 4 years after the dental trauma.
Discussion
Root fracture compromises several tissues (the dentine, cementum, and pulp) and healing involves a complicated series of events.5 Its management, according to the International Association of Dental Traumatology (IADT), involves the use of short-term, non-rigid splints.2 However, there is a lack of substantial high-quality evidence on the effect of the type of splint or its duration on healing outcomes.2,4
Despite the best intentions, splints can have a detrimental effect on healing.3 Provision of a splint can injure teeth during their application, impede optimal oral hygiene, or, in cases of rigid splints, restrict physiological movement.4 A splint in a growing individual can also act as an orthodontic appliance if it is not passive or if it is not removed at the requisite time. In the case presented here, the patient had an anterior cross-bite, which developed after maintaining an active splint for 9 months. In addition to the compromised aesthetics of an anterior cross-bite, if left untreated it could lead to further negative consequences.7
An anterior cross-bite in mixed dentition can be corrected by orthodontic therapy with removable or fixed appliances.8,9 However, orthodontic treatment in teeth with a history of trauma has not been widely reported, and therefore definitive conclusions and recommendations are difficult to extract.10 In this case, a simple and economical method was used with occlusal build-ups on the lower primary molars, avoiding the need for other orthodontic appliances. This method allowed correction of the cross-bite through natural movement and soft tissue pressure, such as that from the tongue and cheeks. This so-called myofunctional approach has been used where anterior cross-bites are present with no associated skeletal imbalances.11
The use of resin composite buildups in primary molars interferes minimally with speaking and mastication.11 One notable advantage of using contrasting coloured composites was the ease of removal. Monitoring is fairly straightforward with this approach and monitoring at 5–6 weekly intervals has been advised.12 One complication that has been reported is the intrusion of composite bonded units; however, this was corrected spontaneously within 2–3 months of the removal of the build-ups.12
In this case, it is thought that maintaining an active splint for 9 months after the trauma was responsible for the development of the anterior cross-bite, with retroclined upper central incisors, and upper primary canines and first primary molars in a more buccal position. Fortunately, because the patient was a child with growing potential, it was possible to correct the cross-bite with a simple myofunctional approach. In addition, the root fracture in UR1 successfully healed with hard and connective tissue and the root development continued.
Conclusions
This case highlights the importance of follow-up visits with patients after dental trauma and the risk of splints in generating malocclusions in children when the splints are active and maintained for too long. In addition, a simple and effective method for treating the anterior cross-bite created as a consequence of the splint is shown.