
Article
The goal of any dentist when carrying out a tooth extraction is to ensure ease of removal with minimal force in a swift manner that preserves socket integrity, minimizes trauma and improves the patients' trust in the surgical ability of the operator. The importance of prior planning, attention to root morphology, assessment of available coronal tooth structure and bony architecture will help guide the clinician to achieve this goal.1 We would like to describe one scenario that readers may like to reflect upon – the extraction of the lower molar tooth.
As one of the first permanent teeth to erupt, together with their unique position and morphology, lower first molars are more frequently affected by dental caries than any other mandibular tooth.2 This, together with the extensive restorative work that usually follows, renders these teeth structurally fragile and they, therefore, frequently fracture on removal. We would like to discuss a common dilemma faced by clinicians in choosing either a cowhorn or eagle beak forceps for the lower molar extraction. A better understanding of the mechanical principles of exodontia can help the operator select the most appropriate instrument.
Mechanical principles of exodontia
Human teeth are highly tolerant of damage, their structural integrity under stress is vital to functional longevity, but also for successful removal.3 The most common intra-operative complications of exodontia are fracture of teeth and alveolar bone, which are frequently the result of excessive forces being transmitted onto the tooth through the instrument, together with incorrect hand movements.4 The amount of force required to remove a tooth is determined by the functional alveolar bone level, dimensions of the periodontal lamina, configuration and angle of root divergence.5
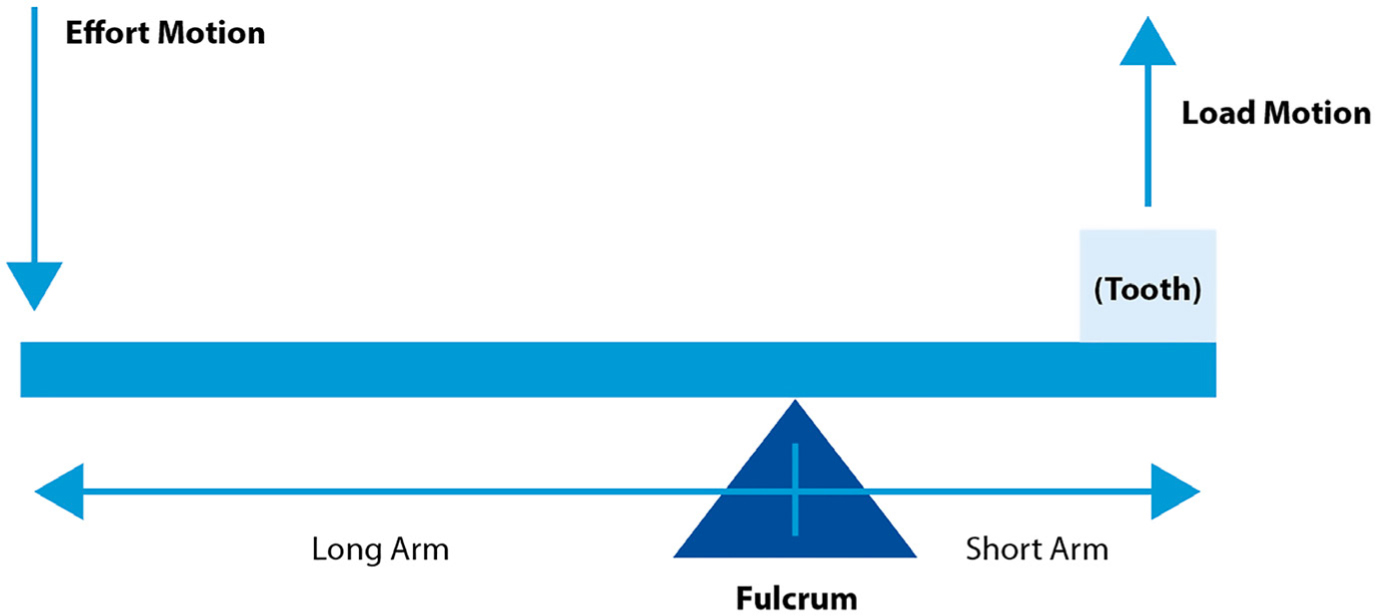
Extraction forceps and elevators both work by the principle of first class leverage to gain a mechanical advantage of small forces generating larger movements (Figure 1). Elevators use the alveolar bone adjacent to the point of application as the fulcrum. Forceps can be thought of as two first class levers connected by a hinge that acts as a fulcrum. The handle acts as the long arm of the lever and the force applied is related to the effort applied by the operators' hand strength. The blades act as the short arm of the lever and transmit force directly onto the tooth.
The blades of extraction forceps are narrow and sharp enough to engage into the periodontal ligament space, thus creating a wedging effect. This firm grasping of the tooth will allow for appropriate expansion of the socket through apical pressure, buccal, lingual and rotational motion, together with tractional forces to separate its periodontal ligament attachments and deliver the tooth out of its alveolar housing. When compared to rotational movements, rocking forces (buccal and lingual) require greater strength.6 It is vital to ensure forceps of the correct size and shape, which mould to the morphology of the tooth, are selected. This should simplify the extraction movements by reducing the applied strength needed and, therefore, the risk of fracture.
Discussion
Lower eagle beak forceps were first designed in Sheffield in 1956 and can be thought of as a hybrid between cowhorn and conventional lower molar forceps. Both the cowhorn and eagle beak forceps incorporate long, thin and sharp blades that engage in the furcation area to firmly wedge the tooth as the grip is tightened. So that the investing soft tissue is not crushed, care should be taken to ensure the sharp blades sit between the gingival margin and tooth. When the roots are conical and convergent the simple application of either forceps into the furcation may alone elevate the tooth, obviating the need for additional movements.
One fundamental design difference between the two is the wider wing design incorporated into the eagle beak forceps (Figure 2). The wings act as a buttress against the root mass to create a positive locking mechanism to prevent slippage. This may protect maxillary teeth from iatrogenic damage caused by sudden release of the forceps as seen with cowhorns' when the tooth ‘pops out’. The blades sit on top of the alveolar crestal margins and are not drawn into the socket as the beak closes, reducing the risk of root fracture at the furcation. This may prevent the need for additional surgical bone removal to establish a point of application for elevation, which is associated with increased risk of infection, swelling and prolonged healing.7

It is important to remember that mandibular molar teeth are set in denser bone than their maxillary counterparts, as demonstrated by the thicker buccal cortical bone and a more condensed pattern of trabeculation seen radiographically. They also exhibit a greater variation of root inclination and angulation.8 Therefore, it is not uncommon for excessive uncontrolled forces to be applied to these teeth during exodontia, which are then distributed and contribute to the post-operative development of temporomandibular disorders (TMD). Symptoms include myofascial pain, clicking and limitation of mouth opening. Treatment for this ranges from initial conservative measures such as non-steroidal analgesia, massage and jaw physiotherapy, to occlusal splints and occasionally surgery.
Where sufficient supracrestal tooth structure remains, together with favourable root morphology, eagle beak forceps are, in the authors' opinion, more efficient at removing lower molars. This technique uses less force, in a more controlled manner, and reduces the procedure time – all factors vital in preventing TMD. There is also inherently less trauma to the surrounding soft tissues, which helps to better preserve the alveolar socket integrity.9 This will contribute to a smoother recovery with fewer post-operative complications as mentioned above.
Conclusion
We believe the lower eagle beak forceps are an excellent asset to the dentists' armamentarium for mandibular molar extractions. Handled with care and dexterity, they provide a more effective way to remove lower molar teeth intact, while minimizing trauma and reducing the need for a surgical approach.