Public Health England. Child oral health: applying All Our Health. 2019. https://tinyurl.com/yyrfbrfp (accessed November 2020)
Goodwin M, Sanders C, Pretty IA. A study of the provision of hospital based dental general anaesthetic services for children in the northwest of England: part 1 – a comparison of service delivery between six hospitals. BMC Oral Health. 2015; 15 https://doi.org/10.1186/s12903-015-0028-4
A conscious decision.London: Department of Health; 2000
Shaw AJ, Meechan JG, Kilpatrick NM, Welbury RR. The use of inhalation sedation and local anaesthesia instead of general anaesthesia for extractions and minor oral surgery in children: a prospective study. Int J Paediatr Dent. 1996; 6:7-11 https://doi.org/10.1111/j.1365-263x.1996.tb00201.x
Jameson K, Averley PA, Shackley P, Steele J. A comparison of the ‘cost per child treated’ at a primary care-based sedation referral service, compared to a general anaesthetic in hospital. Br Dent J. 2007; 203 https://doi.org/10.1038/bdj.2007.631
Blain KM, Hill FJ. The use of inhalation sedation and local anaesthesia as an alternative to general anaesthesia for dental extractions in children. Br Dent J. 1998; 184:608-611 https://doi.org/10.1038/sj.bdj.4809708
Hosey MT UK National Clinical Guidelines in Paediatric Dentistry. Managing anxious children: the use of conscious sedation in paediatric dentistry. Int J Paediatr Dent. 2002; 12:359-372 https://doi.org/10.1046/j.1365-263x.2002.03792.x
Ekbom K, Jakobsson J, Marcus C. Nitrous oxide inhalation is a safe and effective way to facilitate procedures in paediatric outpatient departments. Arch Dis Child. 2005; 90:1073-1076 https://doi.org/10.1136/adc.2004.060319
Arch LM, Humphris GM, Lee GTR. Children choosing between general anaesthesia or inhalation sedation for dental extractions: the effect on dental anxiety. Int J Paediatr Dent. 2001; 11:41-48 https://doi.org/10.1046/j.1365-263x.2001.00238.x
Lyratzopoulos G., Blain KM. Inhalation sedation with nitrous oxide as an alternative to dental general anaesthesia for children. J Public Health Med. 2003; 25:303-312 https://doi.org/10.1093/pubmed/fdg068
Frankl SN, Shiere FR, Fogels HR. Should the parent remain with the child in the dental operatory?. J Dent Child. 1962; 29:150-163
Soldani F, Manton S, Stirrups DR, Cumming C, Foley J. A comparison of inhalation sedation agents in the management of children receiving dental treatment: a randomized, controlled, cross-over pilot trial. Int J Paediatr Dent. 2010; 20:65-75 https://doi.org/10.1111/j.1365-263X.2009.01005.x
Bryan RA. The success of inhalation sedation for comprehensive dental care within the Community Dental Service. Int J Paediatr Dent. 2002; 12:410-414 https://doi.org/10.1046/j.1365-263x.2002.00400.x
Foley J. A prospective study of the use of nitrous oxide inhalation sedation for dental treatment in anxious children. Eur J Paediatr Dent. 2005; 6:121-128
Galeotti A, Garret Bernardin A, D'Antò V Inhalation conscious sedation with nitrous oxide and oxygen as alternative to general anesthesia in precooperative, fearful, and disabled pediatric dental patients: a large survey on 688 working sessions. Biomed Res Int. 2016; 2016 https://doi.org/10.1155/2016/7289310
Chinn GA, Sasaki Russell JM, Sall JW. Is a short anesthetic exposure in children safe? Time will tell: a focused commentary of the GAS and PANDA trials. Ann Transl Med. 2016; 4 https://doi.org/10.21037/atm.2016.10.43
Routh JC, Bacon DR, Leibovich BC How long is too long? The effect of the duration of anaesthesia on the incidence of non-urological complications after surgery. BJU Int. 2008; 102:301-304 https://doi.org/10.1111/j.1464-410X.2008.07663.x
Ing C, Hegarty MK, Perkins JW Duration of general anaesthetic exposure in early childhood and long-term language and cognitive ability. Br J Anaesth. 2017; 119:532-540 https://doi.org/10.1093/bja/aew413
Paediatric dental treatment under inhalation sedation by a therapist in secondary care: An audit Elara Palmer Sarah-Jayne Campbell Lee Foo Dental Update 2024 47:11, 707-709.
We investigated the success of paediatric dental treatment under inhalation sedation (IHS) with nitrous oxide completed by a dental therapist, as an alternative to general anaesthesia (GA) in secondary care. We found that 94% of had treatment successfully completed under IHS by a therapist. These patients were assessed as being suitable for IHS and were referred to the therapist via a new patient clinic. The success of therapists treating paediatric patients with IHS could help reduce pressure on GA waiting lists. As well as being a safer treatment option, this method allows effective conservative treatment to be completed and thereby reducing the number of extractions required, which is a major benefit to patients' future health and wellbeing.
CPD/Clinical Relevance: This study shows the success of treatment under inhalation sedation by a dental therapist. Appropriate referral to therapists has the potential to reduce the need for procedures under general anaesthesia. This has the affect of reducing the strain on our general anaesthetic waiting lists, as well as having a positive impact on the health and wellbeing of our patients with IHS being considered the safer option.
Article
In 2013, the most recent survey by the Health and Social Care Information Centre concluded that almost half of all 8 year olds (46%) and one-third of 5 year olds (31%) in England, Wales and Northern Ireland had experienced obvious dental decay in their deciduous teeth.1 While dental treatment is often successfully completed in the primary care setting, many children require more specialist treatment and are referred to hospital for dental treatment under conscious sedation (CS) or general anaesthesia (GA). The NHS is under a great deal of pressure to provide GA for paediatric dental treatment, with £35 million spent on hospital-based extractions for those under the age of 18 in 2014–2015.2 As well as being an obvious financial strain on the NHS, the high demand for dental general anaesthetic services results in subsequently long waiting times. This is illustrated in a study by Goodwin and colleagues who found the average waiting times over six hospitals to be 8 months.3 These factors highlight the importance of finding methods to reduce the number of hospital admissions for paediatric dental extractions under GA. A review by the Department of Health in 2000 advised that inhalation sedation with nitrous oxide is a safer and more cost-effective alternative to general anaesthetic for dental treatment.4 Further studies also found inhalation sedation (IHS) to be a more cost-effective treatment option in comparison to GA.5,6,7
Inhalation sedation (IHS) using nitrous oxide is the preferred method for conscious sedation in paediatric dentistry.8 This is largely due to its desirable qualities, which include rapid onset and recovery of sedation, minimal side effects and actions as an analgesic and anxiolytic.9 Previous reports of nitrous oxide for use in dental treatment of children have concluded that there was a significant reduction in patient dental anxiety after undergoing IHS for treatment when compared with GA.10 IHS has also been found to be more satisfactory by both patients and parents.11 Many papers have studied the use of IHS with nitrous oxide as an alternative to general anaesthetic in paediatric patients, but few have studied the success and benefits of a therapist in carrying out the IHS and treatment. The use of therapists in this way could help to relieve the pressure on GA waiting lists as well as reduce costs associated with dental treatment in hospitals. An additional benefit is that it has the potential to be carried out, successfully and safely in the community in primary dental care, without the need for treatment within the hospital or referral to secondary care.
Aims and outcomes
We investigated the success of paediatric dental treatment under IHS with nitrous oxide, as an alternative to GA, by a therapist. To register this service as a useful alternative to GA, we set a standard that at least 90% of those referred should be treated successfully. This is in line with reported success rates.13,14,15,16,17 A further objective was to consider whether successful treatment is dependent on patient age, referral source, type of treatment or Frankl behaviour scores.
Method
Data were collected retrospectively from the electronic data management (EDM) system used by St George's Hospital. Electronic notes were collected for all patients who had undergone dental treatment under IHS by a therapist from November 2015 to May 2018.
Initial data collected included: the age of the patient, which staff member referred the patient for IHS, what type of treatment the patient was referred for (eg conservative treatment only, extractions only or conservative treatment as well as extractions), the Frankl behaviour score (Table 1) of the child at assessment, and whether the planned treatment under IHS by the therapist was successful or unsuccessful. ‘Successful’ was denoted by the completion of all planned treatments using IHS. ‘Unsuccessful’ treatment denoted a treatment plan that was not completed under inhalation sedation. When this occurred, notes were made about why and what action was taken for the child to receive treatment. Patients who did not attend for complete treatment were also considered to have unsuccessful treatment.
Negative: child reluctant to accept treatment, some evidence of negative attitude
3
Positive: acceptance of treatment, cautious at times, willingness to comply with dentist at times with reservation, follows directions
4
Definitely positive: good rapport with dentist, interest in dental procedures, laugher and enjoyment
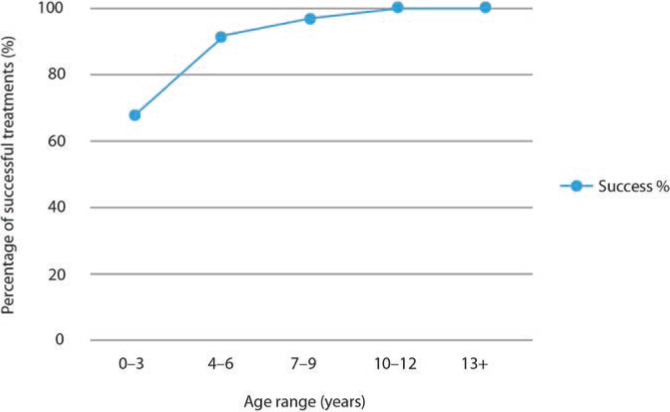
Graphs and tables were used to reflect the percentage of successfully treated patients (Figure 1) dependent on their age (Table 2), treatment type (Table 3), Frankl behaviour score (Table 4), and referring staff member.
Figure 1. Line chart showing percentage of successful treatment across age ranges.
Age of patients (years)
Success (%)
0–3
67
4–6
91
7–9
96
10–12
100
13+
100
Treatment type
Success (%)
Conservation
98
Conservation and extractions
93
Extractions
9
Frankl score
Success (%)
2
94
3
98
4
100
Unknown
76
Data from 202 paediatric patients were included. Any notes not part of the EDM system were excluded, along with patients undergoing active treatment.
Results
Out of 202 patients, 189 treatment plans were completed, giving a success rate of 94%. Treatment was unsuccessful with 13 patients, 12 of whom subsequently had their treatment completed under GA. While four of the patients in the unsuccessful treatment group had initial extractions with IHS, they could not cope with further extractions under IHS when attempted. Six patients would not allow any treatment after the administration of nitrous oxide, and two patients coped well with fissure sealants and the administration of local anaesthetic but could not cope with extractions. One patient did not return to have treatment completed.
Discussion
Overall, 94% of referred patients had treatment successfully completed under IHS by a therapist. As expected, increasing age saw a higher percentage of patients completing the treatment plan (Table 2).
Although one specialist referred a higher number of patients, both specialists made an appropriate number of referrals: 93% and 94% of patients referred by clinicians 1 and 2, respectively, had treatment successfully completed. Table 3 gives the number of patients referred for conservative treatment and extractions, extractions alone and conservative treatment alone. Treatment was less successful when extractions were involved. Despite treatment being deemed unsuccessful for 13 patients, successful conservative treatment meant that a shorter time under GA was required for the remaining extractions, which is thought to be safer.18,19
Increasing Frankl behaviour rating score resulted in a higher percentage of successfully treated patients (Table 4).
Conclusion
This audit shows that treatment under IHS is a very successful method for treatment of paediatric patients with decay. The 181 patients who were treated with IHS alone avoided GA entirely. Other points that can be concluded from this review include that the Frankl behaviour scale is useful in identifying patients who may be able to cope with treatment under IHS and that specialists appropriately refer patients to the therapist for treatment under IHS.
Of the successfully treated patients, 94% exceeded the standard of at least 90% of patients referred to the dental therapist for inhalation sedation be treated successfully. This level of success is similar to dentists' success rates of treatment using IHS in paediatric dentistry.13,14,15,16,17
The success of therapists treating appropriate paediatric patients with IHS would help reduce pressure on GA waiting lists. As well as being a safer treatment option, it also allows successful conservative treatment to be completed, reducing the number of necessary extractions, which is beneficial for patients' future health and wellbeing. It is, however, integral that realistic treatment planning is carried out, as there was an increase in failure rates when the treatment plan included extraction. The one patient who did not attend to complete treatment, had extractions carried out at the last appointment they attended.