Barrowman RA, Grubor D, Chandu A. Dental implant tourism. Aust Den J. 2010; 55:441-445
Miyagi K, Auberson D, Patel AJ, Malata CM. The unwritten price of cosmetic tourism: an observational study and cost analysis. J Plast Reconst Aesth Surg. 2012; 65:22-28
Jaapar M, Musa G, Moghavvemi S, Saub R. Dental tourism: examining tourist profiles, motivation and satisfaction. Tourism Management. 2017; 61:538-552
Gaviria L, Salcido JP, Guda T, Ong JL. Current trends in dental implants. J Korean Assoc Oral Maxillofac Surg. 2014; 40:50-60
General Dental Council. Standards for the Dental Team. 2013. https://tinyurl.com/ybqs4yga (accessed November 2020)
Martin MV. Training standards in implant dentistry for general dental practitioners. A report. Primary Dental Care. 2006; 13:117-118
Lunt N, Green ST, Mannion R, Horsfall D. Quality, safety and risk in medical tourism. Medical tourism: the ethics, regulation, and marketing of health mobility. Medical Tourism: The Ethics, Regulation, and Marketing of Health Mobility. 2012; 33:31-46
Shahed SS, Nagaral SC, Mujawar AM. Basal Implants: a breakthrough for atrophic ridges. J Appl Dent Med Sci. 2018; 4:50-54
Many patients travel abroad seeking cosmetic dental treatment, in particular dental implants. However, there are hundreds of dental implant systems being used globally by dentists of all training backgrounds. Furthermore, complications can occur that patients may expect their general dental practitioner in the UK to be able to manage. The following report describes the case of a 71-year-old, medically compromised patient who presented with complaints consistent with the immediate failure of dental implants that happened to be placed abroad. On closer examination, the dental implants themselves were highly questionable in their design and placement. An incidental finding was also made in the maxillary sinus.
CPD/Clinical Relevance: To acknowledge that implant dentistry is increasing in popularity as patients have the freedom to access dental implant treatment globally. UK dentists are expected to manage these dental implants on the return of patients to the UK who may present with post-operative complications involving unknown dental implant systems.
Article
Introduction
There appears to be an increase in the number of patients travelling abroad for dental treatment, coined by some as ‘dental tourism’.1,2 The drive for ‘dental tourism’ appears to be multifactorial; some of the more common reasons include the drive for dental care to meet patient-led timeframes and to gain dental treatment at a lower cost than that offered within the UK.3 In addition, low-cost flights mean that the cost of transportation combined with dental treatment abroad can be significantly lower than the cost of dental treatment in the UK. Furthermore, dental-tour packages are available to the public which, include dental treatment, travel and accommodation, all as part of the holiday package.
Implants within dentistry appear to have gained popularity in recent times, particularly noticeable within the last decade,4 as research on the design, materials and placement of dental implants has increased over the past few years. Additionally, implant placement can be carried out in a variety of settings including universities, specialist centres and increasingly by general dental practitioners (GDPs) in dental practices. Another variable factor is that of clinician expertise as there is currently no recognised subspecialty for implant dentistry. For the most part, dental implants are seen as an alternative treatment option compared with the conventional options for space restoration. Despite this, dental implants are not only an alternative treatment modality, but in many cases, they are the first choice for patients, as they offer more perceived benefits over other treatments. For example, in cases where teeth have been lost from the aesthetic zone, or in cases of severely atrophic edentulous ridges.5
In the UK, the dental profession is regulated by the General Dental Council (GDC), which states that ‘You must only carry out a task or a type of treatment if you are appropriately trained, competent, confident and indemnified.’6 Regarding dental implants, the GDC has provided guidance that the concept of dental implants as a mode of treatment to replace missing teeth should be introduced to dental students during their time as dental undergraduates in order to familiarise them with this treatment modality. Currently, this means that a UK-qualified dentist is not deemed to be competent to perform implant dentistry without undergoing structured postgraduate training and assessment of their competence.5
The Faculty of General Dental Practice (UK) published and regularly updates its ‘Training Standards in Implant Dentistry’, which is supported by the GDC. The guidance serves as a framework to provide a baseline of standards to be met by institutes that provide training in implant dentistry in the UK, such as universities, hospitals, Royal colleges and courses run by commercial providers and individuals. The development of these standards safeguards patient safety, while concurrently providing consistency to those teaching and attaining knowledge and clinical skills in implant dentistry. Additionally, the FGDP guidance provides a reference for the GDC when considering patient complaints regarding the malpractice of dentists who are allegedly performing implant dentistry without possessing the necessary competence.7
Below is a description of a case of ‘dental-implant tourism’, which led to post-operative complications, including the complete failure of the dental implants provided to the patient. The subsequent treatment required to stabilise the patient is described.
Case report
A 71-year-old female patient was referred by their GDP to the oral and maxillofacial surgery department with the principal complaint of a mobile bridge in the upper right quadrant and an associated bad taste (Figure 1). She gave a history of having travelled abroad to have a number of dental implants placed. She suffered from sarcoidosis, type II diabetes, hypertension, ischaemic heart disease and was taking warfarin for atrial fibrillation. Social history was unremarkable as the patient never smoked and did not drink alcohol.
Figure 1. Intra-oral view of the failed implant bridge replacing the UR4/UR5/UR6.
Clinical examination revealed a partially dentate patient with an extensively restored dentition. There was a grade II mobile bridge replacing the upper right premolars and first molar in the upper right quadrant, a root filled upper right canine retained root and edentulous spaces in the lower left quadrant (Figure 1). Most of the patient's upper anterior sextant and entire lower anterior sextant were crowned with continuous splinted crowns, with some of these teeth having been root filled.
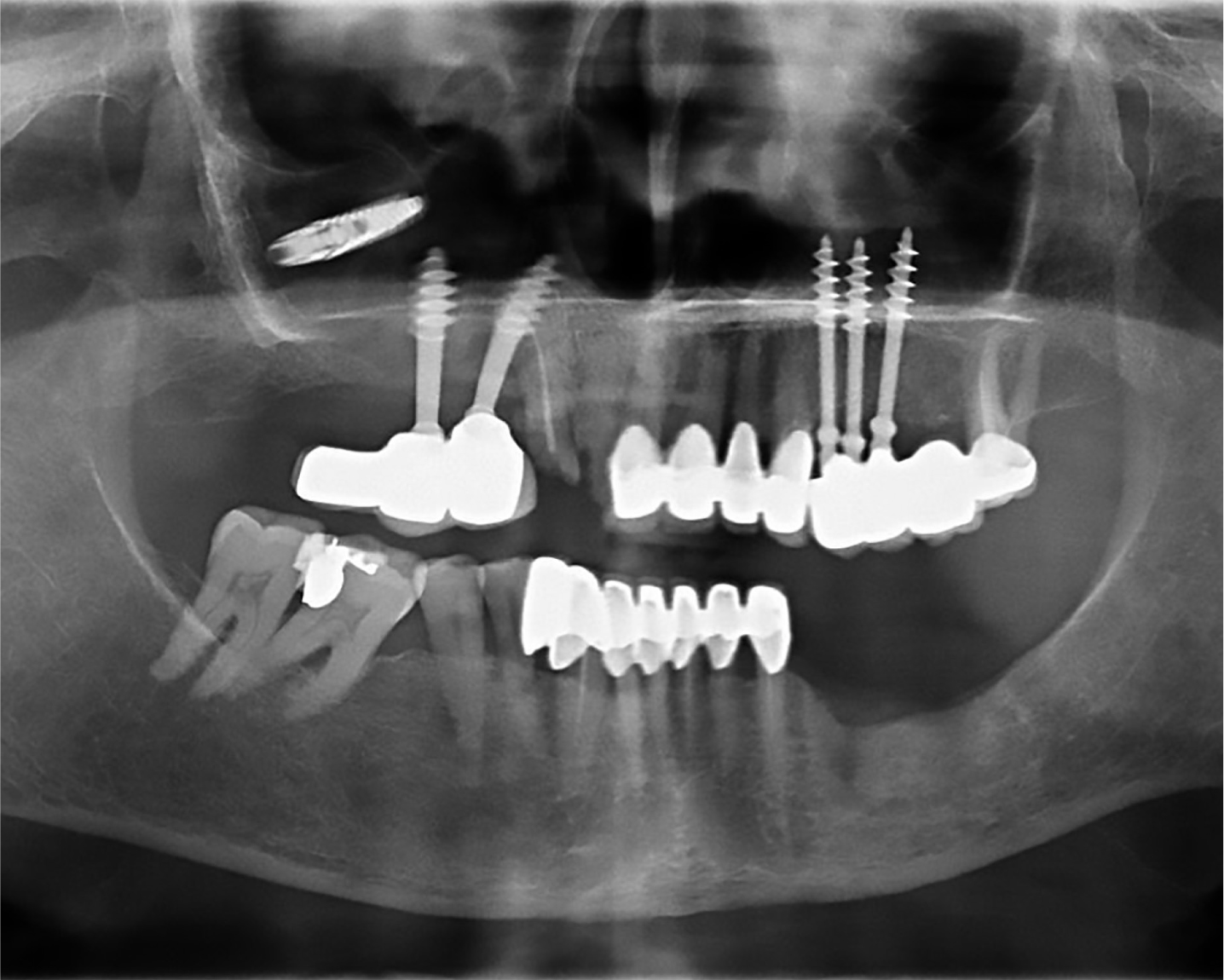
Radiographic examination (dental panoramic radiograph) showed dental implants replacing the upper right and left premolars and first molars, with severe bone loss surrounding the upper right premolar and first molar, and a dental implant retained within the right maxillary sinus (Figure 2).
Figure 2. Pre-operative panoramic radiograph showing failed implants, and an implant in right maxillary sinus.
Procedure
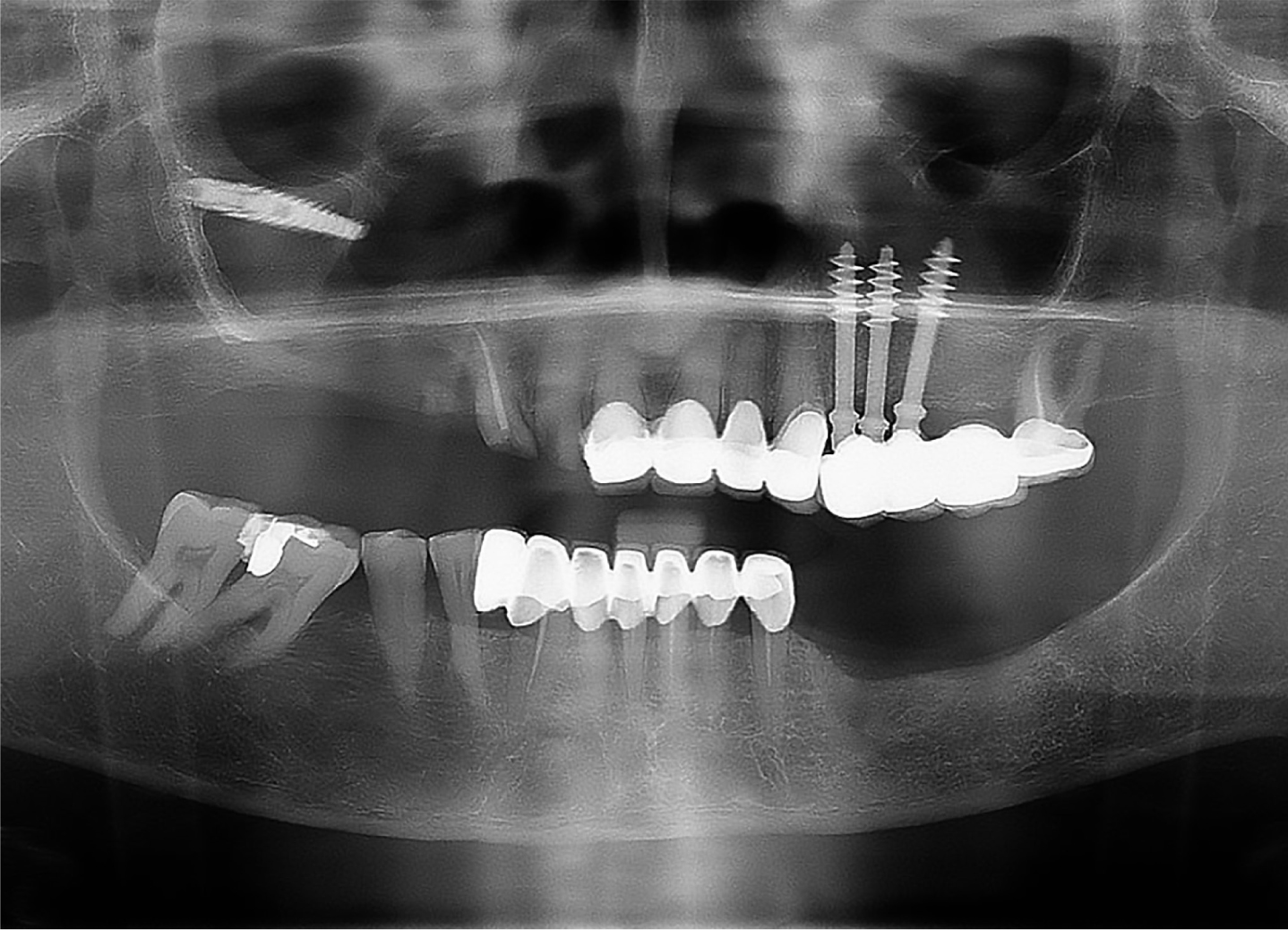
The aim of treatment was to relieve the patient's symptoms by addressing the principal complaint of a mobile bridge in the upper right quadrant with an associated bad taste. It was therefore decided that the first phase of treatment would involve removal of the mobile dental implants replacing the upper right premolar and first molar (Figures 3 and 4). The removal of the dental implants created an oro-antral communication (OAC) in the upper right quadrant, which was managed surgically with primary closure. The outcome was positive as healing of the OAC had occurred and was present clinically (Figure 5) and radiographically (Figure 6). A decision was made to conservatively manage the symptom-free dental implant within the right maxillary sinus with regular clinical and radiographic review.
Figure 3. Implants removed from upper right quadrant.Figure 4. Intra-oral view after removal of implants in the upper right quadrant.Figure 5. Intra-oral view at the review appointment showing closure of the OAC.Figure 6. Post-operative Panoramic Radiograph showing closure and bony infil of the OAC.
Discussion
With increased patient expectations, dentists have to balance patient needs versus patients' wants and desires. This may translate into patients who are deemed orally unsuitable for dental implants in the UK deciding to seek this treatment abroad, where their expectations can be met by their clinician. In doing so, these patients are at risk of potentially receiving suboptimal treatment and an increased long-term cost, both financially and to their oral health.8 However, we must take into account and respect the patient's prerogative to seek a second opinion and make an informed decision, irrespective of the consequences.
It is important to note that suboptimal treatment may arise due to a plethora of reasons including the following:
Differences in training;
Surgical technique;
Uncertified systems;
Materials and systems at a low cost to the buyer;
Untested materials and systems;
A lack of clinical governance in places where dentists can be unregulated or poorly regulated;
Patients unaware or given little choice in the types of implants they can receive;
Reduced labour costs of dentists;
Lack of availability of resources;
Patient-specific factors including: patient time availability, compliance, pre-existing medical conditions, social habits, oral hygiene practices and the health of their pre-existing dentition.
This is exemplified by the case mentioned above that demonstrates a case of misjudged treatment using inappropriate prostheses, which led to a multitude of consequences for the patient. The dental implants used for this patient were variable in diameter, length and fixture design. There was a dental implant resembling mainstream-design unanchored and free-floating within the right maxillary sinus. The longer dental implants resembled monobloc basal cortical screw dental implants. These are dental implants designed to incorporate both a long smooth span and apical screw threads. This type of dental implant is advocated in instances of immediate loading with the theory that the screw fixture will be placed into basal bone for anchorage, negating the need for a bone graft. It is therefore believed to be suitable for a resorbed ridge. The unthreaded smooth part of the dental implant is designed to prevent bacterial colonisation, with the belief that this will prevent the occurrence of peri-implantitis.9
Cases of this nature may be encountered in increasing numbers by clinicians in primary care and via referral to specialist oral and maxillofacial surgery departments. This particular case would have benefited from a multidisciplinary approach given the associated dental and medical complexities.
The case in question highlighted some of the problems faced by clinicians and surgeons as a result of questionable implant dentistry. In this particular case, as a result of the dental implant treatment received abroad, the patient required removal of the failed dental implants to regain oral stability and will require further treatment to regain satisfactory function and aesthetics.
What is difficult to ascertain overall is whether the dental implants failed due to patient factors, clinician factors or due to factors related to the dental implant systems themselves. It is the authors' opinion that the reasons for failure were multifactorial and could be attributed to both the patient and the dental implants themselves, but we believe the crux of the failure was a result of inappropriate treatment planning. Specifically, the dental implant system used was believed to be a ‘one-for-all’; however, the clinician may not have taken into account the need for bone grafting and the importance of maintaining good oral hygiene. Instead, reliance was placed solely upon the dental implant system's apparent ability to integrate into cortical bone and prevent the adherence of bacteria, with no other peri-operative factors in place to secure their success, including oral hygiene and maintenance. Readers should be aware that due to the increased prevalence of dental implant tourism, they may be faced with an increasing number of cases of compromised, or even failed treatment, with some of these cases complicated further by unknown systems and, therefore, unknown management techniques. Dentists in the UK may be expected to rectify these clinical problems when patients present with post-operative complications. This means that dentistry within the UK may see an increased element of reparative work in order to stabilize such patients.
The medical tourism industry poses a threat to the UK economy and to its dentists due to the fact that that the global health market will continue to attract consumers, and so dentists must be prepared to face the consequences of this prevalent practice.8 In light of Brexit and its ongoing negotiations, patients may find that travelling further afield, beyond the European Union (EU), is more appealing overall as border controls may be introduced within the EU, and the cost of air flight to Europe may increase. British citizens will be excluded from the European Health Insurance Card, which entitles UK citizens to free or a reduced cost of treatment in other EU countries, as a consequence of leaving the EU.10
Summary
As yet, there is no clearly defined or nationally recognised post-operative surgical implant management protocol.11 Therefore, until such protocols are designed and a consensus can be reached nationally on dental implant management, clinicians need to be primarily aware of the increase in dental implant tourism and crucially be prepared to manage the consequences of unorthodox dental implant techniques and systems. Where rectification is required in cases with a high index of complexity, it would be prudent to seek a specialist opinion either by referring the patient for treatment planning advice and guidance, or to seek definitive management from their implant dentist abroad. As a GDP, if the decision is made to treat these cases without seeking specialist opinion, it is advisable to discuss the proposed treatment plan with an indemnifier as the responsibility for the failed treatment and subsequent treatments may be left with their GDP in the UK.