Gill P, Stewart K, Chetcuti D, Chestnutt IG. Children's understanding of and motivations for toothbrushing: a qualitative study. Int J Dent Hygiene. 2011; 9:79-86
Marinho V, Higgins J, Logan S, Sheiham A. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003; 1 https://doi.org/10.1002/14651858.CD002278
Walsh T, Worthington H, Glenny A Fluoride toothpastes of different concentrations for preventing dental caries. Cochrane Database Syst Rev. 2019; 3 https://doi.org/10.1002/14651858
Harris R, Gamboa A, Dailey Y, Ashcroft A. One-to-one dietary interventions undertaken in a dental setting to change dietary behaviour. Cochrane Database Syst Rev. 2012; 3 https://doi.org/10.1002/14651858.CD006540.pub2
Marinho VCC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013; 7 https://doi.org/10.1002/14651858.CD002279.pub2
Prabhu A, Prasanna B, Sakeenabhi B Effect of fluoride varnish and dentifrices and its combination on deciduous enamel demineralization: an in vitro study. J Pharm Bioallied Sci. 2017; 9:S112-S116 https://doi.org/10.4103/jpbs.JPBS_121_17
Timms LJH, Sumner O, Deery C, Rogers HJ. Everyone else is using it, so why isn't the UK? Silver diamine fluoride for children and young people. Community Dent Health. 2020; 37:143-149
Oliveira BH, Rajendra A, Veitz-Keenan A, Niederman R. The effect of silver diamine fluoride in preventing caries in the primary dentition: a systematic review and meta-analysis. Caries Res. 2019; 53:24-32
Ahovuo-Saloranta A, Forss H, Walsh T Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst Rev. 2017; 7 https://doi.org/10.1002/14651858.CD001830.pub5
Mickenautsch S, Yengopal V. Caries-preventive effect of glass ionomer and resin-based fissure sealants on permanent teeth: an update of systematic review evidence. BMC Res Notes. 2011; 4 https://doi.org/10.1186/1756-0500-4-22
Cascaes AM, Bielemann RM, Clark VL, Barros AJ. Effectiveness of motivational interviewing at improving oral health: a systematic review. Rev Saude Publica. 2014; 48:142-53 https://doi.org/10.1590/s0034-8910.2014048004616
Pine CM, Adair PM, Burnside G Dental RECUR randomized trial to prevent caries recurrence in children. J Dent Res. 2020; 99:168-174 https://doi.org/10.1177/0022034519886808
Caries is one of the most common diseases in the world and it is mostly preventable. Caries can have a large impact on a child's physical, social and mental health. There are a number of clinical interventions available to prevent caries and this article provides a summary of the general guidelines and tips on their implementation in relation to caries prevention in children.
CPD/Clinical Relevance: This article highlights the importance of caries prevention and the relevant interventions, especially in the context of limited access to health services. These guidelines can be beneficial for all dental health professionals.
Article
Introduction
Dental caries continues to be a prevalent disease among children. The most recent Child Dental Health Survey showed that nearly half (46%) of 15 year olds and one-third (34%) of 12 year olds had ‘obvious decay experience’ in their permanent teeth and nearly one-third (31%) of 5 year olds and nearly a half (46%) of 8 year olds had obvious decay experience in their primary teeth.1
Perhaps more worryingly, data from NHS Digital show that tooth decay is the leading reason for hospital admissions among 5–9 year olds (25,702 admissions in 2018–2019).2 For the most part, dental caries is a preventable condition, with many evidence-based approaches currently being recommended.
The following recommendations have been taken from the Department of Health publication ‘Delivering Better Oral Health: An Evidence Based Toolkit for Prevention’3 as well as the Scottish Dental Clinical Effectiveness Programme (SDCEP) guidelines, ‘Prevention and Management of Dental Caries in Children’.4
Toothbrushing
If clinicians were only allowed or, in reality, only had time to give one dental health message, it should be ‘brush your teeth twice a day with a fluoride toothpaste’. Brushing with a fluoride toothpaste is almost certainly the main reason seen for the decline in caries prevalence seen since the late 1960s.
Toothbrushing should start as soon as the first primary tooth erupts and should take place at least twice daily: last thing at night and at one other time. Most children will require supervision and assistance until they are 7 years old, or until they can brush effectively, and should be encouraged to spit out excess, and not rinse with water or mouthwash, as this will wash away the fluoride, diluting it, thereby reducing its caries-preventive effects.
There is no particular technique that has been shown to be better than another, but the patient's existing technique may need to be modified to maximize plaque removal, emphasizing the need to systematically clean all surfaces. For this, disclosing tablets or solutions can be used to help highlight missed areas. For all children, the SDCEP guidelines recommend demonstrating brushing on the child at least annually, and at each recall for those with a higher risk of caries.
Teeth are most caries-prone while erupting: this is because being not in occlusion, they are not cleaned by mastication or the action of the tongue, and being below the occlusal plain may be missed during toothbrushing. This means the tooth remains covered in plaque allowing caries to develop. A practical tip to deal with this is to teach people to brush erupting teeth from the side (Figure 1).
Figure 1. Brushing an erupting tooth from the side. From Rogers et al5 with permission.
There are now apps available to help children with brushing. The majority focus on motivating children to brush for approximately 2 minutes. Some include prompts to change sides and include the back teeth when brushing. Depending on the app, some have instructional videos about how to floss between teeth and maintaining a healthy diet and lifestyle. Popular apps include brushDJ, Chomper Chums, Toothsavers and Disney Magic Timer. These apps are all available for download on iOS and Android devices.6
Research into why children and adolescents brush their teeth clearly shows that they do not link brushing with the prevention of dental decay, but are driven by appearance and cosmetic reasons. This is one of the reasons why children and adolescents are more likely to brush in the morning than in the evening.7 Therefore, when giving toothbrushing advice, it would seem reasonable to piggy back your advice on this cosmetic motivation.
Toothpaste
Fluoride toothpaste has a clear caries-inhibiting effect.8 The evidence for the effects of using different concentrations of fluoride in toothpaste is more limited, and the choice of concentration of fluoride toothpaste should always balance the benefit of caries prevention with the low risk of fluorosis.9 A good tip to help manage toothpaste dosage is to advise people to dispense the toothpaste across the brush and not along it. Table 1 presents the current fluoride toothpaste recommendations by age and caries risk.
Under 3 years old
Aged 3 and above
Ages 7 years and above and young adults
No less than 1000ppm fluoride
1350–1500ppm fluoride for all except those who cannot be stopped from eating the toothpaste
Use fluoridated toothpaste 1350–1500ppm fluoride
No more than a smear of toothpaste is needed
A pea-sized amount of toothpaste
For children with active caries
Age 10+ years: prescribe 2800ppm fluoride toothpaste
Age 16+ years: prescribe either 2800ppm or 5000ppm fluoride toothpaste
Use of additional fluoride
Tablets and drops
These are not recommended as a first line for caries prevention and other additional methods should be considered in the first instance. This is because their use requires excellent compliance from patients and their carers, and there is more risk of over- or underuse. There is also a possible risk of fluorosis in children under 6.
Fluoride rinses
These have a concentration of 225ppm fluoride. They are recommended for patients aged 8 and above with active caries, and should be used in addition to the correct toothpaste and at a different time from brushing. They can only be used in children who can effectively spit the liquid out. A sensible regimen would be for children to brush their teeth morning and night and use the mouthwash when they come in from school.
Diet advice
Although the evidence to support the effectiveness of diet advice to prevent caries is lacking, it would be remiss not to provide it as caries and diet are so linked.10 General advice for caries prevention is that the frequency and amount of food and drinks containing free sugars should be reduced.
Free sugars are monosaccharides and disaccharides that are added to food or drinks, and are also sugars in syrups, honey and fruit juices. Free sugars do not include natural sugars in fresh, whole fruit and vegetables, or in milk and milk products. The key word here is ‘whole’ because once fruit is squeezed, and the sugar released from the cells, it is no different in its cariogenic potential from any other free sugar. This is something that patients and their carers are frequently not aware of, thinking that it is safe to drink fruit juice or smoothies when it is not.
Only plain water or milk should be taken between meals. ‘Safer snacks’, which should be encouraged, include fresh fruit and vegetables (eg carrot sticks), oatcakes and breadsticks.
When giving dietary advice to reduce consumption of sugars it is essential to assess the overall pattern of eating to establish the following information:
The number of intakes of food and drinks per day;
The number of intakes that contain free sugars and how many were consumed between normal mealtimes;
Whether any intakes containing sugars were taken within one hour of bedtime (when the caries protective effects of saliva are reduced).
To do this, the use of a diet diary may be helpful. Diet diaries should include all food and drinks consumed, and at what time. It is also useful to include tooth brushing times on diet diaries, as this supports comprehensive advice.
There are two approaches to taking a diet diary: one is a 3-day report and the other is to ask a patient to recall what they had to eat the previous day. Both approaches are equally as good.
Overall diet advice should be positive and practical. Patients do not respond well to being told not to do something, it is much more effective to offer options and alternatives, as suggested above. Put simply, say: ‘do this rather than that’.
Topical fluoride
The use of fluoride varnishes is an extremely effective way of delivering high-strength fluoride to children, and their role in preventing dental caries has been reported by many studies and confirmed by systematic reviews and meta-analyses.11 The mechanism of action of this substance is by the steady release of fluoride ions to the tooth surface, which are deposited in the porosities and micro-channels of the enamel, thereby promoting remineralization.12 There is now evidence that suggests that fluoride varnish can arrest caries on smooth surfaces of primary teeth. The most widely used formulations contain sodium fluoride 1% and 5%. Current guidance recommends that for children over 2 years, sodium fluoride varnish 5% should be applied twice a year, with an additional 1–2 applications yearly for children with a high caries risk.3 Application of the product is straightforward, and dental nurses can be trained to provide this service under the prescription of a dentist. Although it is recommended that deposits of plaque are removed before application, drying the teeth surface with a cotton roll can be sufficient, which is particularly useful in the face of a global COVID-19 pandemic. For a small number of patients, the colophony component in some preparations of fluoride varnish presents a risk of a hypersensitivity reaction. For these patients, colophony-free varnishes are available (Figure 2).4
Figure 2. An example of a colophony-free fluoride varnish.
Silver diamine fluoride
While fluoride varnish application is a well-established intervention for preventing dental caries, silver diamine fluoride (SDF) is attracting increasing attention.13 The literature mainly reports its use in the management of existing caries, but there is increasing evidence of its effectiveness in caries prevention in the primary and permanent dentition. A recent systematic review by Oliviera and co-workers found a 54% decrease in new carious lesions in primary teeth with annual SDF application, compared with quarterly fluoride varnish.14 One of the issues with SDF when used to treat caries is that it turns the lesion black. This side-effect does not occur when it is used for primary prevention. As more evidence becomes available, it appears likely that SDF will be increasingly used for caries prevention, as well as control.
Fissure sealants
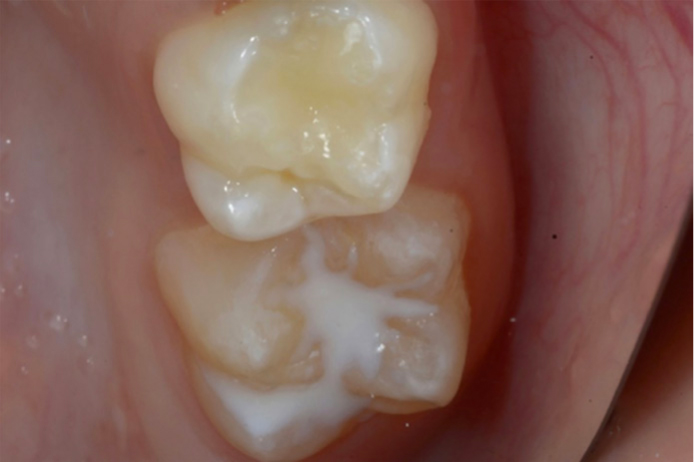
Fissure sealants help to prevent caries, mainly in the pits and fissures of occlusal tooth surfaces, the most caries-prone areas. The most recent Cochrane review reporting on the effectiveness of sealants indicates a caries reduction of over 50% for sealed surfaces compared with non-sealed surfaces after 4 years.15 There are currently two types of fissure sealants: resin-based and glass ionomer sealants (Figures 3 and 4). Historically, the evidence suggested resin sealants were superior to glass ionomer ones, but with improvements in materials, this difference is disappearing. Glass ionomer sealants have the disadvantage that they are more likely to require maintenance and re-application more frequently than resin ones.16 However, glass ionomer sealants are of particular value when the conditions for placement are suboptimal.4 This includes poor patient cooperation, poor moisture control and partially erupted teeth.
Figure 3. Resin sealant on an upper first permanent molar. (From Rogers et al5 with permission.)Figure 4. Fissure sealing of LL6 and LLE with a glass ionomer sealant material (GC Fuji TRIAGE).
DCby1 (Dental Check by One)
In 2017, the British Society of Paediatric Dentistry (BSPD), in partnership with the Office of the Chief Dental Officer for England, introduced a scheme that ensured all children see a dentist as their teeth erupt, or at least by the age of one. This scheme has proven to be a success nationally. The scheme enables clinicians to deliver preventive advice, such as oral hygiene instructions and diet advice, to parents from an early stage. Currently, the scheme is not active during the COVID-19 pandemic. However, the BSPD have worked on creating posters and interactive videos available online for patients, detailing preventive advice.17
Motivational interviewing
Motivational interviewing is a patient-centred approach that encourages the patient's own will for change. The foundation for this approach is based on the relationship between the dentist and the patient. It can be difficult to influence someone's attitudes and behaviours because these are determined by a number of factors, including an individual's beliefs, societal norms, attitudes of family members among many other components.18 Behavioural change can be complex because there are many moving parts to it. Traditionally, behaviour-changing mechanisms have been rooted in the clinician directing their beliefs and wishes onto the patient. Nowadays, the patient is at the centre of the conversation and has the right to exercise their autonomy when it comes to their own health. The motivational interviewing approach is patient centred, engaging and evokes the patient's emotions, to motivate them to bring about changes to their own dental health.
This approach includes four aspects: partnership, acceptance, compassion and evocation. The first step is to engage the patient and develop a good relationship with them and their parents, focusing on building a good rapport. The second stage involves focusing on the issue at hand and identifying the problems that need to be addressed. Following on from this, clinicians need to evoke and identify the patient's own motivation to change. The clinician and the patient will then need to make a plan and implement a strategic way of reaching the desired outcome (agree achievable goals). Reviewing the patient to monitor their progress builds the dentist–patient relationship, and allows a chance for feedback.19 Ultimately, communication and behaviour management is a crucial element in caries prevention in children. The effectiveness of motivational interviewing is well recognized: for example, a trial looking at reducing the risk of repeat general anaesthetics found a 29% decrease in the development of new caries in the group receiving motivational interviewing compared with more traditional preventive advice.20
Summary
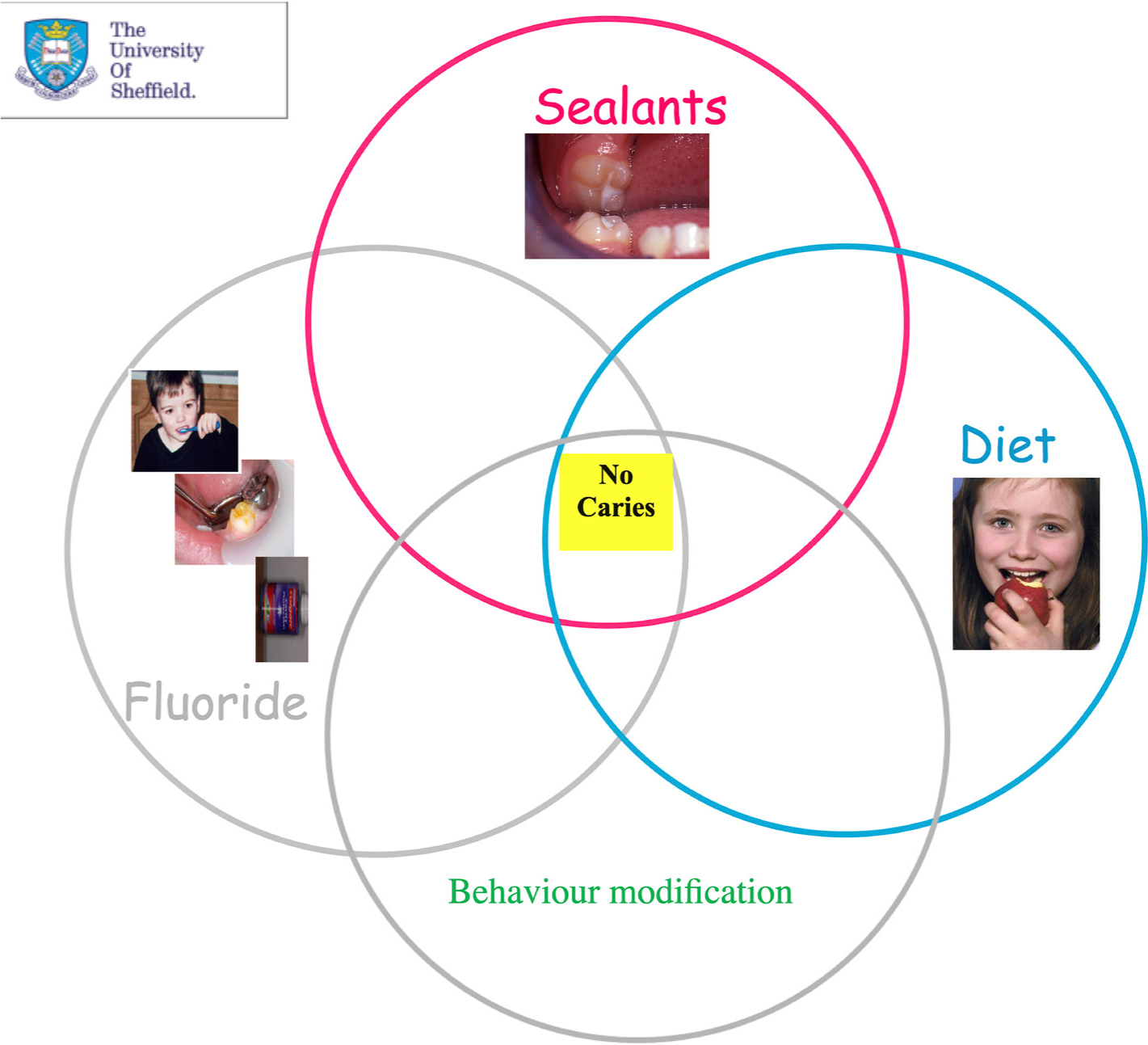
Caries is almost completely preventable using the interventions discussed above, and summarized in Figure 5, together with fully exploring the patient's concerns and goals for their dental health in a supportive and non-judgemental way. Lowering the prevalence of caries can have massive impacts economically and improve the quality of life of children.
Figure 5. Summary of caries preventive strategies.