Black GV. A work on operative dentistry.Chicago: Medical Dental Publishing; 1908
Elderton RJ. The prevalence of failure of restorations: a literature review. J Dent. 1976; 4:207-210
Maltz M, Henz SL, de Oliveira EF, Jardim JJ. Conventional caries removal and sealed caries in permanent teeth: a microbiological evaluation. J Dent. 2012; 40:776-782 https://doi.org/10.1016/j.jdent.2012.05.011
Fejerskov O, Kidd EAM. Dental caries: the disease and its clinical management.Oxford: Blackwell; 2003
Schwendicke F, Frencken JE, Bjorndal L Managing carious lesions: consensus recommendations on carious tissue removal. Adv Dent Res. 2016; 28:58-67 https://doi.org/10.1177/0022034516639271
Pires PM, Neves AA, Makeeva IM Contemporary restorative ion-releasing materials: current status, interfacial properties and operative approaches. Br Dent J. 2020; 229:450-458 https://doi.org/10.1038/s41415-020-2169-3
FDI policy statement on minimal intervention dentistry (MID) for managing dental caries. Adopted by the General Assembly. September 2016, Poznan, Poland. Int Dent J. 2016; 67:6-7 https://doi.org/10.1111/idj.12308
Innes NP, Frencken JE, Bjorndal L Managing carious lesions: consensus recommendations on terminology. Adv Dent Res. 2016; 28:49-57 https://doi.org/10.1177/0022034516639276
Bjorndal L, Fransson H, Bruun G Randomized clinical trials on deep carious lesions: 5-year follow-up. J Dent Res. 2017; 96:747-753 https://doi.org/10.1177/0022034517702620
Mertz-Fairhurst EJ, Curtis JW, Ergle JW Ultraconservative and cariostatic sealed restorations: results at year 10. J Am Dent Assoc. 1998; 129:55-66
Schwendicke F, Dorfer CE, Paris S. Incomplete caries removal: a systematic review and meta-analysis. J Dent Res. 2013; 92:306-314 https://doi.org/10.1177/0022034513477425
Bjorndal L. Reentry may not be needed after partial caries removal in mainly young permanent molars with caries involving half or more of the dentin thickness. J Evid Based Dent Pract. 2013; 13:62-63 https://doi.org/10.1016/j.jebdp.2013.04.008
Banerjee A, Frencken JE, Schwendicke F, Innes NPT. Contemporary operative caries management: consensus recommendations on minimally invasive caries removal. Br Dent J. 2017; 223:215-222
Innes NP, Evans DJ, Stirrups DR. The Hall technique; a randomized controlled clinical trial of a novel method of managing carious primary molars in general dental practice: acceptability of the technique and outcomes at 23 months. BMC Oral Health. 2007; 7 https://doi.org/10.1186/1472-6831-7-18
(Deep) dentine caries and restorative care: Adopted by the FDI General Assembly: 7 September 2018, Buenos Aires, Argentina. Int Dent J. 2019; 69:7-8 https://doi.org/10.1111/idj.12464
Slimani A, Terrer E, Manton DJ, Tassery H. Carious lesion detection technologies: factual clinical approaches. Br Dent J. 2020; 229:432-442 https://doi.org/10.1038/s41415-020-2116-3
Schwendicke F, Gostemeyer G. Understanding dentists' management of deep carious lesions in permanent teeth: a systematic review and meta-analysis. Implement Sci. 2016; 11 https://doi.org/10.1186/s13012-016-0505-4
Schwendicke F, Stangvaltaite L, Holmgren C Dentists' attitudes and behaviour regarding deep carious lesion management: a multi-national survey. Clin Oral Investig. 2017; 21:191-198 https://doi.org/10.1007/s00784-016-1776-5
Chai B, Tay B, Chow C Treatment preferences for deep caries lesions among Australian dentists. Aust Dent J. 2020; 65:83-89 https://doi.org/10.1111/adj.12740
Burke F. Technique tips: patient information leaflet information for patients for whom deep caries has been sealed into a vital asymptomatic tooth. Dental Update. 2018; 45
Bjorndal L, Darvann T, Thylstrup A. A quantitative light microscopic study of the odontoblast and subodontoblastic reactions to active and arrested enamel caries without cavitation. Caries Res. 1998; 32:59-69 https://doi.org/10.1159/000016431
Bjorndal L, Reit C, Bruun G Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci. 2010; 118:290-297 https://doi.org/10.1111/j.1600-0722.2010.00731.x
Hevinga MA, Opdam NJ, Frencken JE Does incomplete caries removal reduce strength of restored teeth?. J Dent Res. 2010; 89:1270-1275 https://doi.org/10.1177/0022034510377790
Tjaderhane L, Tezvergil-Mutluay A. Performance of adhesives and restorative materials after selective removal of carious lesions: restorative materials with anticaries properties. Dent Clin North Am. 2019; 63:715-729 https://doi.org/10.1016/j.cden.2019.05.001
Minimally Invasive Selective Caries Removal put into Practice Bhupinder Dawett Sarah Young Chris Deery Avijit Banerjee Dental Update 2024 47:10, 707-709.
Authors
BhupinderDawett
BDS MDPH
Doctoral Research Fellow, School of Clinical Dentistry, University of Sheffield
Professor of Cariology & Operative Dentistry, Hon Consultant in Restorative Dentistry, King's College London Dental Institute at Guy's Hospital, KCL, King's Health Partners, London, UK
Dental caries remains a significant health problem globally, causing morbidity in those affected and consuming health resources. The management of caries consumes considerable finances both for individuals and the public purse. The scientific understanding of the dental caries process has evolved considerably over the last four decades with a move towards a minimum intervention oral care (MIOC) approach to managing patients. The minimally invasive operative intervention that retains demineralised, caries-affected dentine under a well-sealed restoration in order to avoid instrumentation close to the pulp, has shown clinical efficacy in treating individual teeth, as part of the MIOC framework. However, implementation of the selective caries removal approach in deep lesions is still not thought to be practised routinely by clinicians both globally, and in the UK. This article discusses some of the issues that may account for this and describes a case study using this operative strategy.
CPD/Clinical Relevance: Restoring deep carious lesions can be a challenge, but using selective caries removal approaches will help minimise the adverse effects of pulp trauma.
Article
Introduction
Background
Although epidemiological surveys over the last four decades have shown an improvement of the rates of dental caries in the UK, caries is still a common problem with the 2009 Adult Dental Health Survey indicating that 84% of UK adults have at least one restoration.1 The Child Dental Health Survey 20132 reported that nearly half (46%) of 15 year olds in the UK have obvious caries experience and a similar number (45%) of 15 year olds reported that their daily life had been affected by problems with their teeth and mouth in the preceding 3 months.2 Over a third (35%) of parents of 15-year-old children reported that their child's oral health had impacted negatively on family life and, over the same period, nearly a quarter of parents had needed to take time off work because of their child's oral health.3 Children indicating engagement with positive oral health behaviours were less likely to have severe or extensive caries. Furthermore, the burden of severe or extensive caries was borne unequally across society, with those most deprived being more affected.
Traditionally, caries was considered an infectious disease. The caries process was synonymous with the resulting carious lesion and was to be cured by the entire surgical removal of the disease-causing microorganisms together with the affected tooth tissue.4 Traditional restorative materials were retained macro-mechanically and cavities were overprepared to facilitate this, as well as removing the bacteria and demineralised dentine. This approach led to large restorations, resulting in weakening of the tooth-restoration complex,5 so ultimately placing the tooth at a greater risk of fracture (see Figure 1).
Figure 1. Fracture lines in tooth with ageing dental amalgam restoration.
The above surgical modus operandi usually encompasses the need for local anaesthesia and the onerous use of the dental handpiece and rotary bur. It is recognised that both of these are factors that compound dental anxiety in patients.
Clinical and scientific research over the decades has advanced the understanding of the caries process and now places emphasis on less destructive, primary, secondary and tertiary prevention-based management options. A study found that mechanical removal alone was unable to eradicate all bacteria from the cavity.6 Management of the disease process now focuses primarily on controlling the plaque biofilm, depriving the disease-causing bacteria of carbohydrates and encouraging remineralisation at the reversible stages of disease progression.7 It is accepted that the traditional need to remove completely the caries-affected tooth tissue prior to restoration placement is no longer necessary or advocated.8 The placement of contemporary restorative biomaterials, employing adhesive technology for retention, can effectively isolate the remaining bacteria, within the depths of the lesion, from the surface biofilm. With this realisation, removal of carious tissue should only be necessary to provide a suitable tooth-restoration interface for effective adhesion and seal, and to give support to the tooth-restoration complex against the forces of mastication.9
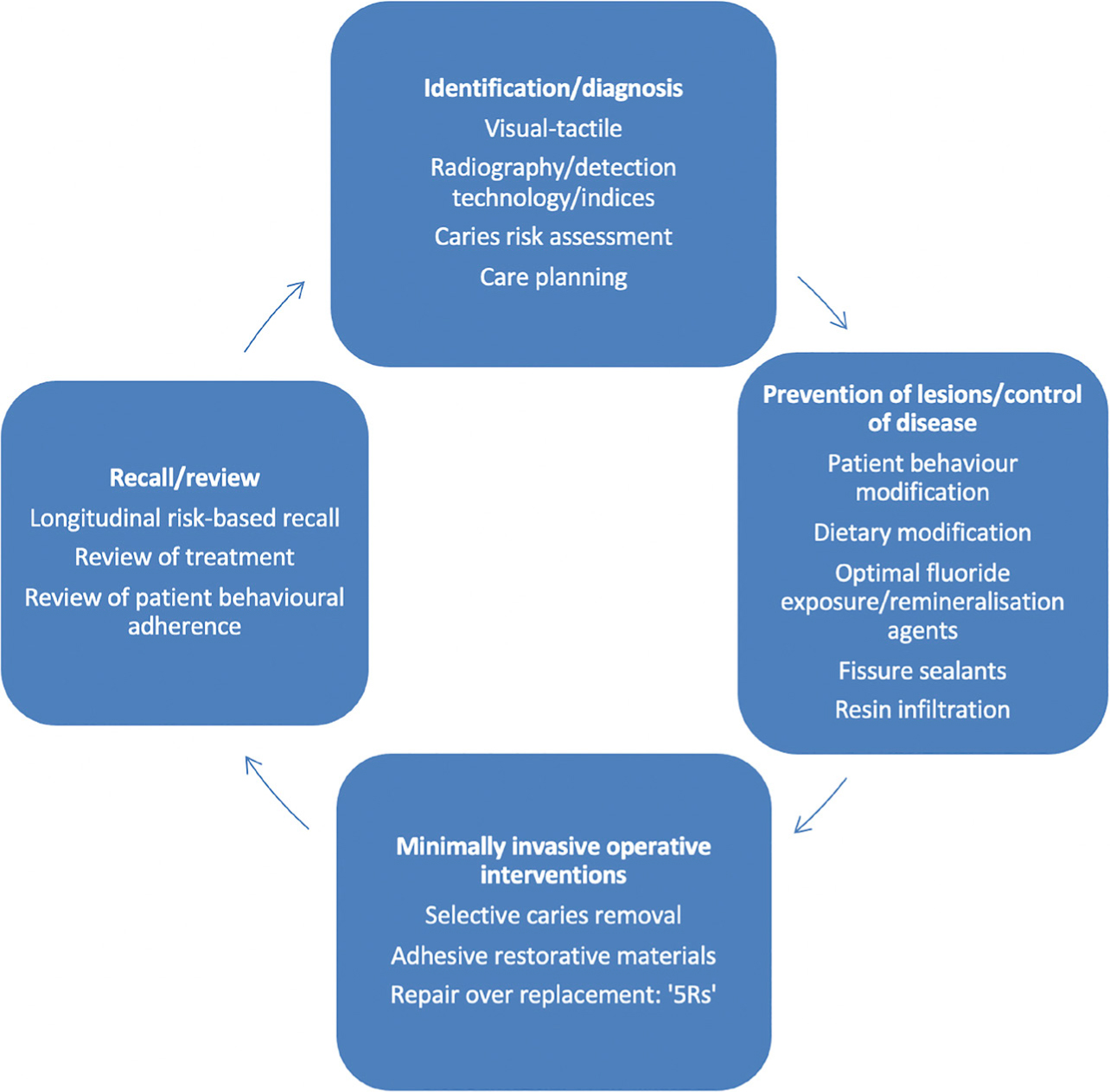
The holistic journey of patient-focused care, oral healthcare team-delivered caries management, constitutes the minimum intervention oral care (MIOC) framework (Figure 2).10,11 It comprises four interlinked care domains, and can be applied to all aspects of restorative dentistry, to patients of all ages, with suitable modifications where required. Even though the domains follow a logical order, patient care may start at different places within the cycle. As can be seen in Figure 2, minimally invasive dentistry (MID) forms one of the treatment domains, focusing on the treatment of individual teeth, not the patient as a whole.
Figure 2. The four interlinked domains of the minimum intervention oral care framework.10,11
The carious lesion
Carious lesion instigation and progression is a result of the microbial activity in the overlying dysbiotic plaque biofilm. Where the overlying biofilm and availability of fermentable carbohydrates (free sugars) in the diet can be controlled, this is all that is required to arrest the advancement of the lesion.
If a lesion progresses uncontrolled to cavitation, this provides shelter for biofilm accumulation and stagnation. This, in turn, offers potential for the caries process to proceed in this area unabated. Facilitating easier access to cleaning of this area by the patient may be achieved in some cases – non-restorative cavity control (NRCC). For example, where an enamel overhang exists on a buccal cavity then just smoothing or removing this ledge may be all that is required for the patient to remove overlying biofilm regularly and apply topical remineralising agents helping to arrest the lesion. This is difficult if the lesion is in the occlusal fissure system, or affects a proximal surface. Hence in these clinical scenarios, removal of minimal amounts of tissue may be required to facilitate placement of a restoration and protect the tooth tissue from any overlying biofilm. Also, proximal lesions can be difficult to assess when vision and tactility are compromised by the presence of an adjacent tooth.
The use of therapeutic resin-based fissure sealants where the occlusal surface is not cavitated can be an effective treatment in providing a barrier to the overlying biofilm (Figures 3 and 4). It is important that these micro-invasive interventions are evaluated regularly in the recall consultations.
Figure 3. Early occlusal fissure lesion.Figure 4. Resin-based fissure sealant provides a barrier from overlying biofilm and enables improved biofilm disruption by the patient.
Caries removal in deep carious lesions
Consensus terminology on the extent of a carious lesion is useful to avoid ambiguity. A deep carious lesion is defined as one which, on radiographic appearance, reaches the inner third or quarter of dentine, and operative intervention would risk pulp exposure (Figure 5).12
Figure 5. Bitewing radiograph of tooth 16 (UR6): arrow indicates deep carious lesion.
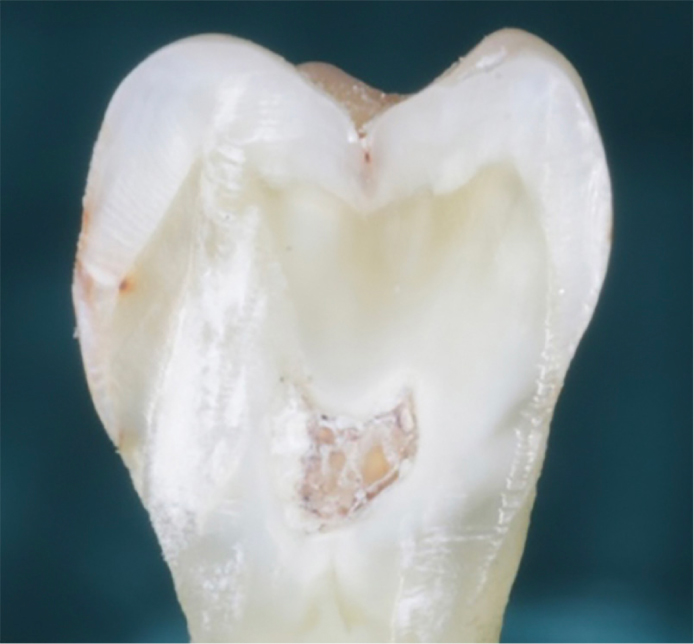
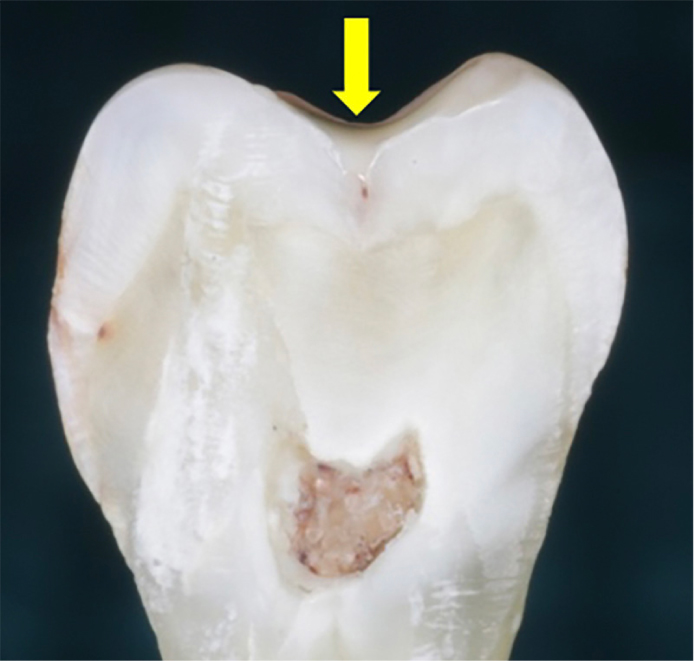
Deep carious lesions are highly likely to have surface cavitation (Figure 6). Treatment has to be respectful to the risk of pulp trauma that may arise during the process of carious dentine removal. It is important to try to maintain pulp sensibility. Avoidance of pulp exposure can improve the likelihood that pulp sensibility is maintained and that the tooth remains asymptomatic.13 This approach can reduce the need for endodontic treatment or even extraction.
Figure 6. Surface cavitation of a deep lesion.
The traditional approach described by GV Black over 100 years ago, and still unfortunately to a large extent practised today, suggested removing all tooth tissue affected by caries and shaping a cavity to maximise mechanical retention before placing a dental amalgam restoration.4 Prior to placing an amalgam in the tooth it was accepted that the cavity should have been prepared so that a ‘hard pulpal floor’ was reached. Such a macro-retentive and biologically unfavourable cavity design is not warranted today given the development of adhesive dental restorative biomaterials and dental adhesives. Operative removal of tooth tissue can now be kept to a minimum, with resultant cavities kept minimal in size and volume. The reasons for removal of carious tooth tissue are: (1) to enable sufficient integrity and support of the restoration; (2) to enable effective bonding to the periphery of the cavity in order to affect a seal; and (3) protect the dentine-pulp complex.
A 10-year prospective clinical study by Mertz-Fairhurst et al in which carious dentine was retained under sealed restorations, demonstrated that the caries process could be arrested and that importance should be laid on attaining a good marginal seal and patient oral hygiene.14 This study assessed the treatment of clearly cavitated carious lesions on occlusal surfaces of molars and premolars. The three restorative treatments studied were: sealed self-curing resin composite restorations where only the enamel was bevelled and no carious dentine removed; localized sealed amalgam restorations without an extension for prevention; and a traditional conventional amalgam restoration with extension for prevention. In both the amalgam restoration arms, caries was removed to hard dentine. This study showed that in the sealed resin composite group, the lesions had arrested. This study concluded that occlusal cavitated lesions visible radiographically into dentine (outer 1/2) that were restored with sealed restorations performed better than those with an unsealed traditional amalgam approach.
For a carious cavity, there are no consistently valid clinical technologies available to determine the exact endpoint in dentine excavation for attaining an optimal biological restoration. Also the terms used in dentistry relating to the level of caries removal can be confusing. In 2015, the International Caries Consensus Collaboration (ICCC) met to try to agree terms for caries removal.12 The following terms were agreed:
Selective removal of carious tissue: including selective removal to soft dentine and selective removal to firm dentine;
Stepwise removal: including stage 1, selective removal to soft dentine, and stage 2, selective removal to firm dentine 6–12 months later;
Non-selective removal to hard dentine: formerly known as complete caries removal.
A review by Schwendicke et al in 2013 indicated that selective dentine caries removal (SCR) in deep lesions may be advantageous in reducing the risk of pulp exposure and postoperative symptoms.15 Also, for these lesions, a second operative stage, as in the stepwise removal technique, may not be required.16 The ICCC reached a consensus on caries removal with the endpoint to firm dentine being the acknowledged standard in shallow to moderate, cavitated lesions.17 However, in deep lesions within close proximity to the pulp, caries removal to soft dentine over the pulp floor of the cavity is recommended to reduce the risk of pulp damage.8 The move away from traditional complete caries removal means that softer dentine with more dentine tubular obliteration is retained. However, concerns have been raised regarding the bond strength owing to an incompletely penetrated hybrid layer. Furthermore, the lack of support provided by softer, carious dentine is feared to increase the risk of mechanical failure of the overlying restoration. A review by Schwendicke et al15 reported that less invasive caries removal does not increase the risk of restorative complications. However, retaining all carious tissue is very limited in its application in the permanent dentition owing to modern restoratives not being sufficiently stable to withstand high masticatory forces in shallow lesions spreading to the outer third of dentine radiographically. That said, in the primary dentition, sealing a carious lesion, without carious tissue removal, beneath a stainless steel crown (the Hall technique), has been advocated to be an effective management technique until the tooth exfoliates.18
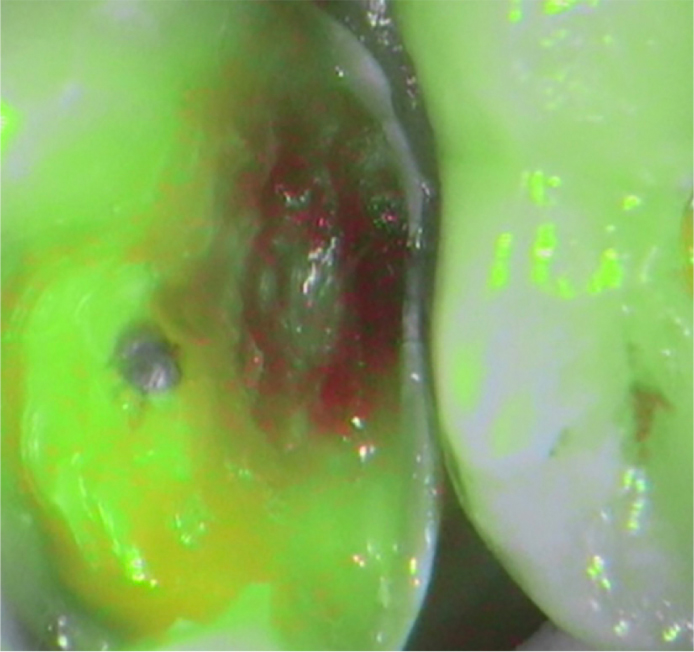
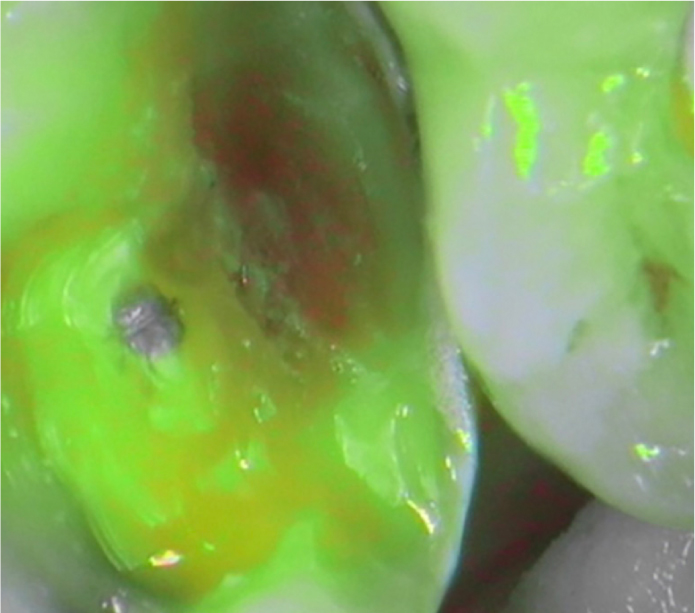
SCR has been adopted by the FDI in its policy statement in 2019.19 However, it must be acknowledged that the boundary between affected and infected dentine cannot clinically be distinguished precisely. Several devices exist to try to guide the practitioner to this endpoint of caries excavation, but these should not be used alone as a definitive decision-making technology (Figures 7–10).20
Figure 7. Soft carious dentine at base of proximal box (Soprolife (Acteon, France) camera daylight mode).Figure 8. Similar image with fluorescent activity showing red (Soprolife camera, caries mode).Figure 9. After selective caries removal (Soprolife camera, daylight mode)Figure 10. Similar image to Figure 9, with fluorescence showing clear margins (Soprolife camera, caries mode).
SCR put into practice
The degree to which SCR is carried out for deep-lesion management in general dental practice in the UK has not been determined. A review by Schwendicke and Gostemeyer in 2016 in Germany indicated that it could be lower than 50%.21 These authors also showed that there was some evidence of a decrease in the proportion of dentists favouring complete caries removal over time. The studies in this review, however, did not include clinicians in the UK. Also a multi-national survey in France, Germany and Norway showed that in Germany and France, a high proportion (66%) would continue to perform complete caries excavation to hard dentine, even in deep lesions.22 This was in contrast to a survey of Australian dentists that found that 85% self-reported that they would use SCR in deep lesions.23
So, with this evidence, what are the potential reasons for the lack of uptake of SCR in primary care?
Education and knowledge
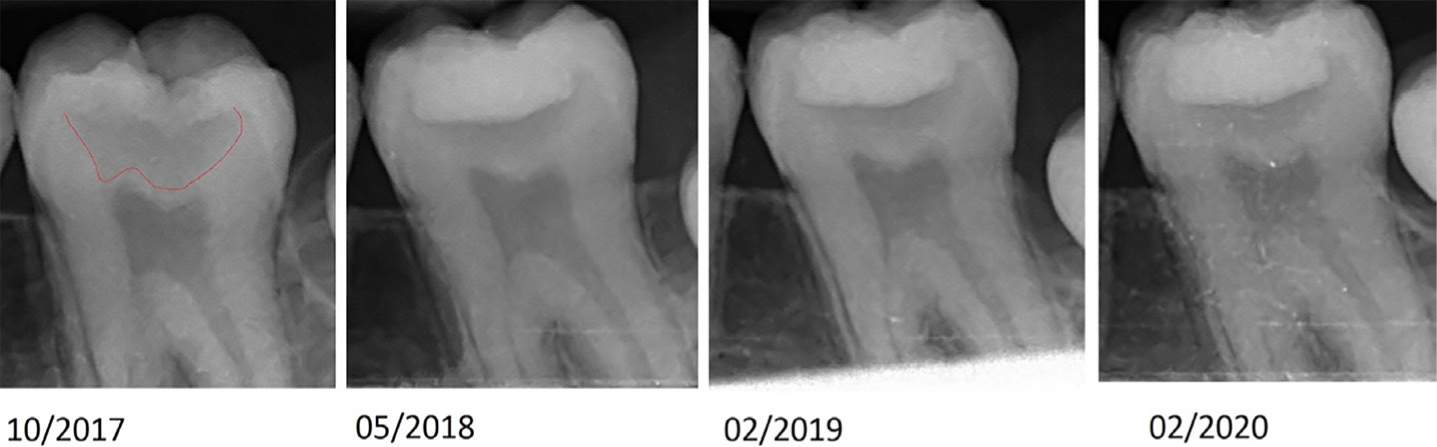
Demineralised, carious dentine is radiolucent. This radiolucency remains if carious dentine is sealed under a restoration (Figure 11). Without an adequate understanding of this and the history of the tooth, this appearance can be misinterpreted as a failing restoration with secondary caries and incur unnecessary re-treatments. For this reason, both patient and practitioner communication and education is important when employing incomplete caries removal techniques.24 It is, therefore, imperative that clinicians keep abreast of the advances in technology and techniques through ongoing continued professional development. It is notable that management of dental caries is neither a core requirement nor a recommended area of CPD for UK dentists or therapists. In 2011, Pitts et al expressed concern regarding the lack of effective teaching of MIOC in the dental curriculum.25 Although teaching in undergraduate curriculums has now progressed in this regard, it is recognised that clinicians who were taught the traditional complete caries removal approach may not have kept up to date and find any change a challenge. There are also postgraduate courses available (google ‘King's AMID’ for information about a blended-learning masters in advanced minimum intervention dentistry, open to practising dentists and therapists worldwide).
Figure 11. Baseline and follow-up radiographs of LL7.
Medico-legal considerations
Patient notes and radiographs would be a significant aid to understanding a previous dentist's intention with regard to the treatment of a lesion, and plotting any change to the extent of the lesion following treatment. However, in NHS general dental practice, unlike NHS general medical practice, patient records do not automatically transfer if a patient changes practice. This could pose a significant barrier to a GDP's willingness to employ increasingly less invasive techniques of caries removal if the clinician fears medico-legal action.26 No evidence exists on the feasibility or acceptability for patients and practitioners to have dental records ‘follow’ a patient from practice to practice. However by not offering a minimally invasive approach, such as SCR, clinicians may find themself at risk of litigation. This highlights the importance of informing and discussing with patients what is being done clinically, and accurately recording this. This should apply equally to those still practising the traditional approaches of complete surgical excision of the lesion, with explanations and the risks.
Economic implications
It is considered financially beneficial to maintain pulp sensibility and avoid endodontic treatment. However, there is no evidence of this cost-effectiveness within the NHS to date, as restorations and endodontic treatment fall within the same NHS treatment band. Furthermore, insufficient reimbursement for preventive care and oral health education is a frequent criticism of the 2006 NHS remuneration contract system based on units of dental activity (UDAs).27 The Steele report recommended explicit recognition of preventive activity.28 A key hurdle to such financial recognition is the difficulty in determining the impact of dental caries on the individual and wider society. The premise of rewarding clinicians weighted on surgical activity may not appear to directly affect the implementation of SCR for deep lesions compared with complete caries removal, but such factors require further investigation.
Evidence base
There is considerable evidence to support the retention of carious tooth tissue when using modern adhesive technologies for the treatment of dental caries.8,13,14,29,31. These show that the caries process can be arrested and the need for endodontic treatment reduced. An in vitro study suggested that incomplete caries removal may result in a reduced fracture strength of the tooth restoration complex.32 However, there is a lack of high-quality evidence comparing this with complete caries removal and its acceptability by NHS patients, practitioners and commissioners. To facilitate a move towards adoption of minimally invasive techniques in day-to-day patient care, it is incumbent on pragmatic primary care clinical trials being conducted in such a way as to recognize the wider influences on stakeholders' decision-making. This calls out for adoption of qualitative research methods to be used in such trials.21 In the UK, the SCRiPT (Selective Caries Removal in Permanent Teeth) trial, funded by the National Institute for Health Research (NIHR), is currently underway, and is looking at the clinical and cost-effectiveness of selective caries removal compared to complete caries removal in permanent posterior teeth.33 This pragmatic trial is taking place in primary care dental sites and, as such, this will help in implementation of any recommendations from the study.
Although some of the issues highlighted by the case study below have been considered, a thorough discussion of the barriers to successful implementation of less invasive caries removal strategies within an NHS dental setting is beyond the scope of this article. That said, the following case study is an example of how selective caries removal can be used to provide treatment for deep carious lesions within a routine NHS primary care general dental practice.
Case study
A 14-year-old patient attended for an urgent appointment for pain, reporting vague symptoms from the upper left quadrant. The patient, previously a regular attender, had been lost to recall for 3 years following extraction of all four, poor prognosis first molars as part of orthodontic treatment. Examination revealed fixed orthodontic appliances on both arches and evidence of extensive caries in the posterior dentition. Following immediate debond, radiographic examination revealed multiple deep carious lesions. Oral health education and prevention was provided to the child and parent in line with national recommendations.34
A deep carious lesion in the occlusal surface of the vital LL7 appeared as a cavitated enamel lesion with dentine shadowing. The LL7 showed a radiographic radiolucency into the pulpal third of the dentine. The carious LL7 was accessed from the occlusal aspect and the undermined peripheral enamel removed. Soft, wet, sticky caries-infected dentine was removed using hand excavators/rotary instruments from the enamel dentine junction until hard, scratchy sound dentine surrounded the cavity periphery. Soft, caries-infected dentine was retained over the pulp with the aim of avoiding pulp exposure and retaining pulp sensibility. The tooth was restored with an adhesive resin composite restoration using the selective etch technique and Scotch Bond Universal adhesive (3M, USA). Currently, the choice of restorative material to be placed after the selective caries removal procedure should be based on clinical judgement as there is no conclusive clinical evidence to confirm the superiority of one restorative material over another when selective caries removal has been carried out.35,36 The patient was given an information leaflet explaining the technique used, to follow up the discussion at the care planning visit.24
Subsequent reviews were undertaken and the LL7 remains vital and asymptomatic at the most recent 3-year recall consultation (Figure 11).
The pulp sensibility was checked at the recall intervals. Periapical radiographs also showed no apical radiolucency.
The patient has required intervention in other teeth with some early non-cavitated lesions progressing. This confirms an ongoing caries process with the patient not ‘cured’ of the disease. Given the initial presentation of the patient, that no extractions or endodontic treatment were required, could this be considered a positive outcome for this patient? The use of SCR may present benefits of patient acceptability and an increased likelihood of completion of an operative course of treatment.
Patient behavioural adherence and improvement of oral health behaviours has been acknowledged as vital to good outcomes in MIOC.37 Behaviour modification for patients using motivational interviewing skills from all oral healthcare team members can be very difficult and, as such, very frustrating for clinicians. Some may even feel that a MIOC approach in these circumstances may be doomed to fail, especially for the arrest of early lesions. Nevertheless, management of deep carious lesions with SCR can still be an effective option. It is important to appreciate that minimally invasive dentistry (MID) treats the tooth, but minimum intervention oral care (MIOC) manages the patient.
Conclusion
The MIOC framework places emphasis on the need to educate the patient in the importance of reducing their caries susceptibility, and attendance for regular monitoring and maintenance. That said, deep carious lesions do not afford the practitioner time to review behavioural adherence to oral health education prior to commencement of the treatment. However, unlike attempts at remineralisation of early lesions, there is no suggestion that adoption of a selective caries removal approach for deep lesions and subsequent failure to engage by the patient will have a negative impact on the outcome at a tooth level versus the traditional approach.
This article presents a case of application of SCR in a deep cavitated carious lesion. The oral healthcare team should be aware of SCR as an effective, minimally invasive operative treatment strategy for the management of deep carious lesions. Implementation also places emphasis on the need for effective communication between the team and patients, as well as maintaining contemporaneous records. Further research is warranted to investigate barriers to implementation of the MIOC framework especially within the NHS, and how they can be overcome.