Bartlett D, Dugmore C. Pathological or physiological erosion – is there a relationship to age?. Clin Oral Investig. 2008; 12:S27-S31 https://doi.org/10.1007/s00784-007-0177-1
Schlueter N, Luka B. Erosive tooth wear – a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018; 224:364-370 https://doi.org/10.1038/sj.bdj.2018.167
Bartlett DW, Lussi A, West NX Prevalence of tooth wear on buccal and lingual surfaces and possible risk factors in young European adults. J Dent. 2013; 41:1007-1013 https://doi.org/10.1016/j.jdent.2013.08.018
Loomans B, Opdam N, Attin T Severe tooth wear: European consensus statement on management guidelines. J Adhes Dent. 2017; 19:111-119 https://doi.org/10.3290/j.jad.a38102
Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM. Current concepts on the management of tooth wear: part 1. Assessment, treatment planning and strategies for the prevention and the passive management of tooth wear. Br Dent J. 2012; 212:17-27 https://doi.org/10.1038/sj.bdj.2011.1099
Wazani BE, Dodd MN, Milosevic A. The signs and symptoms of tooth wear in a referred group of patients. Br Dent J. 2012; 213 https://doi.org/10.1038/sj.bdj.2012.840
Mehta SB, Loomans BAC, Banerji S An investigation into the impact of tooth wear on the oral health related quality of life among adult dental patients in the United Kingdom, Malta and Australia. J Dent. 2020; https://doi.org/10.1016/j.jdent.2020.103409
Bartlett D. A personal perspective and update on erosive tooth wear – 10 years on. Part 1: diagnosis and prevention. Br Dent J. 2016; 221:115-119 https://doi.org/10.1038/sj.bdj.2016.555
O'Toole S, Pennington M, Varma S, Bartlett DW. The treatment need and associated cost of erosive tooth wear rehabilitation – a service evaluation within an NHS dental hospital. Br Dent J. 2018; 224:(12)957-961 https://doi.org/10.1038/sj.bdj.2018.444
Mehta SB, Loomans BAC, Bronkhorst EM A study to investigate habits with tooth wear assessments among UK and non-UK dental practitioners. Br Dent J. 2020; 228:429-434 https://doi.org/10.1038/s41415-020-1326-z
Pindborg J. Pathology of the Dental Hard Tissues.Copenhagen: Munksgaard; 1970
Litonjua LA, Andreana S, Bush PJ, Cohen RE. Tooth wear: attrition, erosion, and abrasion. Quintessence Int. 2003; 34:435-446
Carvalho TS, Colon P, Ganss C Consensus report of the European Federation of Conservative Dentistry: erosive tooth wear – diagnosis and management. Swiss Dent J. 2016; 126:342-346
Hammoudi W, Trulsson M, Smedberg JI, Svensson P. Clinical presentation of two phenotypes of tooth wear patients. J Dent. 2019; 86:60-68 https://doi.org/10.1016/j.jdent.2019.05.028
Hammoudi W, Trulsson M, Smedberg JI, Svensson P. Phenotypes of patients with extensive tooth wear. A novel approach using cluster analysis. J Dent. 2019; 82:22-29 https://doi.org/10.1016/j.jdent.2019.01.001
Banerji S, Mehta S.B, Opdam N, Loomans B. Practical procedures in the management of tooth wear.Chichester: Wiley-Blackwell; 2020
Wetselaar P, Faris A, Lobbezoo F. A plea for the development of an universally accepted modular tooth wear evaluation system. BMC Oral Health. 2016; 16 https://doi.org/10.1186/s12903-016-0309-6
Bartlett D, Ganss C, Lussi A. Basic Erosive Wear Examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008; 12:S65-S68 https://doi.org/10.1007/s00784-007-0181-5
Dixon B, Sharif MO, Ahmed F Evaluation of the basic erosive wear examination (BEWE) for use in general dental practice. Br Dent J. 2012; 213 https://doi.org/10.1038/sj.bdj.2012.670
Huysmans MC, Young A, Ganss C. The role of fluoride in erosion therapy. Monogr Oral Sci. 2014; 25:230-243 https://doi.org/10.1159/000360555
Lussi A, Hellwig E, Zero D, Jaeggi T. Erosive tooth wear: diagnosis, risk factors and prevention. Am J Dent. 2006; 19:319-325
Austin RS, Rodriguez JM, Dunne S The effect of increasing sodium fluoride concentrations on erosion and attrition of enamel and dentine in vitro. J Dent. 2010; 38:782-787 https://doi.org/10.1016/j.jdent.2010.06.009
Carvalho JC, Scaramucci T, Aimée NR Early diagnosis and daily practice management of erosive tooth wear lesions. Br Dent J. 2018; 224:311-318 https://doi.org/10.1038/sj.bdj.2018.172
Bizhang M, Riemer K, Arnold WH Influence of bristle stiffness of manual toothbrushes on eroded and sound human dentin – an in vitro study. PLoS One. 2016; 11 https://doi.org/10.1371/journal.pone.0153250
Turssi CP, Binsaleh F, Lippert F Interplay between toothbrush stiffness and dentifrice abrasivity on the development of non-carious cervical lesions. Clin Oral Investig. 2019; 23:3551-3556 https://doi.org/10.1007/s00784-018-2776-4
Kaidonis JA. Oral diagnosis and treatment planning: part 4. Non-carious tooth surface loss and assessment of risk. Br Dent J. 2012; 213:155-161 https://doi.org/10.1038/sj.bdj.2012.722
Bartlett D, Sundaram G, Moazzez R. Trial of protective effect of fissure sealants, in vivo, on the palatal surfaces of anterior teeth, in patients suffering from erosion. J Dent. 2011; 39:26-29 https://doi.org/10.1016/j.jdent.2010.09.007
Milosevic A, Agrawal N, Redfearn P, Mair L. The occurrence of toothwear in users of Ecstasy (3,4-methylenedioxymeth amphetamine). Community Dent Oral Epidemiol. 1999; 27:283-287 https://doi.org/10.1111/j.1600-0528.1998.tb02022.x
Tschammler C, Müller-Pflanz C, Attin T Prevalence and risk factors of erosive tooth wear in 3–6 year old German kindergarten children. A comparison between 2004/05 and 2014/15. J Dent. 2016; 52:45-49 https://doi.org/10.1016/j.jdent.2016.07.003
Shellis RP, Featherstone JD, Lussi A. Understanding the chemistry of dental erosion. Monogr Oral Sci. 2014; 25:163-179 https://doi.org/10.1159/000359943
Buzalaf MAR, Magalhães AC, Rios D. Prevention of erosive tooth wear: targeting nutritional and patient-related risks factors. Br Dent J. 2018; 224:371-378 https://doi.org/10.1038/sj.bdj.2018.173
Kelleher M, Bishop K. Tooth surface loss: an overview. In: Ibbeston R, Eder A (eds). London: BDJ Books; 2000
Scaramucci T, Hara AT, Zero DT In vitro evaluation of the erosive potential of orange juice modified by food additives in enamel and dentine. J Dent. 2011; 39:841-848 https://doi.org/10.1016/j.jdent.2011.09.004
Dent J, El-Serag HB, Wallander MA, Johansson S. Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2005; 54:710-717 https://doi.org/10.1136/gut.2004.051821
Ghai N, Burke FJ. Mouthwatering but erosive? A preliminary assessment of the acidity of a basic sauce used in many Indian dishes. Dent Update. 2012; 39:721-726 https://doi.org/10.12968/denu.2012.39.10.721
Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM. Current concepts on the management of tooth wear: part 4. An overview of the restorative techniques and dental materials commonly applied for the management of tooth wear. Br Dent J. 2012; 212:169-177 https://doi.org/10.1038/sj.bdj.2012.137
With adult dentitions being retained for longer, issues relating to the wear of teeth are increasingly becoming of relevance to the general dental practitioner. As with any treatment plan, prevention is a fundamental and an important stage in the management of tooth wear. This article outlines the contemporary preventive features that the general dental practitioner should be aware of when dealing with patients presenting with tooth wear or exhibiting a susceptibility to this.
CPD/Clinical Relevance: An understanding of the factors relevant to the prevention of tooth wear will enable an effective preventive regimen to be prescribed. This will play an integral role in the management of tooth wear and its sequalae.
Article
Introduction
As teeth continue to function, they will be routinely exposed to erosive, abrasive and attritive factors. The wearing-away of tooth tissue may therefore be considered as an age-related phenomenon.1 Clinically, however, patients will often present with differing extremes and patterns of tooth wear. Using the available data, a mean global prevalence of erosive tooth wear that is between 20% and 45% in permanent teeth, and between 30% and 50% in deciduous teeth, has been estimated.2 Visible signs of erosive tooth wear were also reported on the buccal and lingual surfaces from 29% of a sample of 3187 adults aged 18–35 years from seven European countries, and the UK had the highest levels of tooth wear.3
Patients with tooth wear may report symptoms of tooth sensitivity and/or pain, functional difficulty and orofacial aesthetic impairment.4,5,6 Progressive tooth wear may also risk the integrity of the patient's residual dentition and have an adverse impact on their quality of life.4,7 However, as the progression of tooth wear is amenable to prevention,8 the prescription of a tailored preventive plan may negate the need for complex and costly longer-term restorative intervention and aftercare,4,9 or at least, help to defer the need.
The implementation of a suitable preventive programme for a patient with tooth wear is, however, dependent on the treating clinician performing appropriate and timely clinical assessments of the extent and severity of the condition, and undertaking careful risk assessments. Although nationally accepted guidance for both tooth-wear risk assessment,10 and for the prevention of tooth wear,11 has been readily available in the UK for quite some time, a recent study by Mehta et al12 reported inconsistencies among UK (and non-UK based dentists) with the undertaking of risk assessments and the use of clinical indices for tooth-wear assessment.
The aim of this paper is to briefly outline the aetiology of tooth wear and to discuss how tooth wear may be practically prevented.
The diagnosis and classification of tooth wear by aetiology
Historically, the established aetiological factors for tooth wear, hence, abrasion, erosion and attrition have also been used to classify the type of tooth wear observed.13 However, these factors do not always take place independently and other processes may be concomitantly involved.14 Nevertheless, as erosive factors are reported to be frequently involved,15 the application of the term, ‘erosive tooth wear,’ has become commonplace, especially within the European literature.
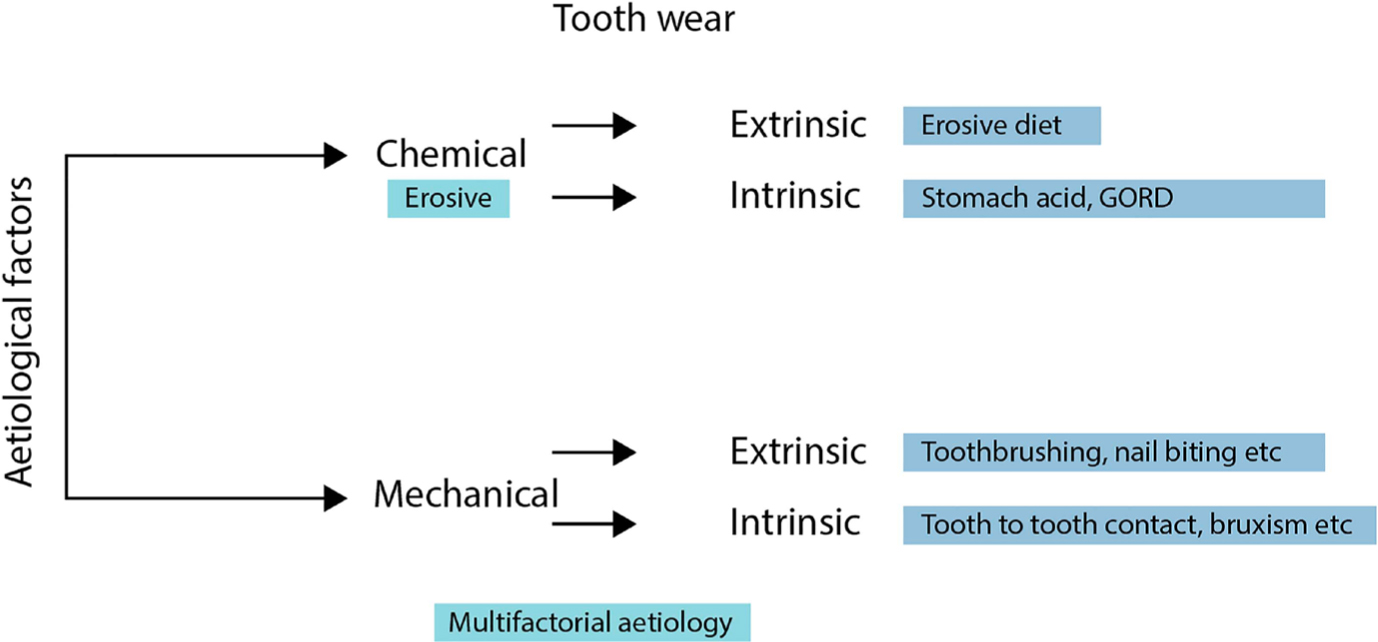
Using cluster analysis, clinical features have been more recently described to distinguish individuals with signs of tooth wear from a chemical cause, a mechanical aetiology, or a combination of both.16,17 By obtaining a careful patient history, and undertaking appropriate patient assessments, the nature of the presenting tooth wear may therefore be broadly divided into mechanical or chemical wear, with four sub-forms (Figure 1):18
Mechanical intrinsic tooth wear as a result of chewing or bruxism, also called attrition;
Mechanical extrinsic tooth wear due to factors other than chewing and/or bruxism, also called abrasion;
Chemical intrinsic tooth wear as consequence of gastric acid, also called erosion;
Chemical extrinsic tooth wear as a result of an acidic diet, also known as erosion. Tables 1 and 2 include a summary of the medical, dental and socio-behavioural factors that may have a role in the initiation and progression of tooth wear.
Figure 1. Chemical and mechanical aetiology of tooth wear. Most cases have a multifactorial aetiology.
Factor
Description
Gastric disorders
Gastro-oesophageal reflux (GORD), gastric ulceration, sphincter incompetence, hiatus hernia, rumination, regurgitation, oesophagitis and increased gastric volume and pressure
Vomiting tendencies
As a result of psychosomatic, gastrointestinal and/or metabolic conditions, or where nausea may occur as a side effect of other medical conditions, or their treatment
Eating disorders
Especially conditions associated with self-induced vomiting, such as bulimia nervosa
The taking of potentially erosive medications or supplements
Hydrochloric acid for achlorhydria (lack of gastric acid)
Iron preparations
Chewable vitamin C tablets
Some types of asthma medication in the form of inhalational aerosols, which may act directly (or indirectly) by leading to a possible relaxation of the oesophageal sphincter
Drugs that may reduce the production of saliva, such as diuretic agents, tranquilizers, antihistamines, anti-emetics, anti-psychotics, anti-Parkinson medication and some antidepressants
Conditions that may reduce saliva
Sjögren's syndrome, Prader–Willi syndrome and congenital rubella23
Psychological conditions
Including anxiety, ADHD, inattention and/or hyperactivity–impulsivity, where the tendency towards bruxist activity may be increased
Chronic alcoholism
May be associated with regurgitation or reflux, as well as possible wear by attrition due to a tendency towards bruxism.
A history of radiation therapy involving the head and neck region.
Factor
Description
Oral hygiene home care habits
Method and frequency of tooth brushing, especially noting a relationship between the timing of brushing and eating, drinking or vomiting, which may exacerbate abrasive wear of a tooth softened by prior acid exposure, especially within the first 1 hour
Relative dentine abrasivity (RDA) of the dentifrice used
Toothbrush filament arrangement, density and the texture of toothbrush used
Diet history
Acidic food and beverage consumption as well as methods of consumption (swishing erosive drinks, retention of erosive agents prior to swallowing and use of a straw), as well as a vegetarian diet. Some patients may also demonstrate the habit of holding citrus fruits against their teeth. Consumption of spicy foods
Alcohol intake
As discussed in Table 1, as well as, smoking and higher levels of caffeine intake, which have been reported to aggravate bruxism
Psychological stress levels, sleep apnoea and a habit of snoring
May serve to aggravate a bruxist tendency
Recreational
Vigorous exercise, which may result in dehydration especially if erosive ‘sports drinks’ are consumed post exercise
Wine tasting
Recreational drugs, such as ecstasy, are associated with reduced saliva and excessive clenching, often manifesting as occlusal attrition (as opposed to incisal attrition)
Occupational
Includes environmental acid exposure and/or abrasive wear seen among carpenters, musicians and hairdressers, stemming from the use of their teeth to hold, nails, mouthpieces and hair clips, respectively
For the undertaking of a clinical tooth-wear examination, descriptive qualitative assessments (such as ‘mild’, ‘moderate’ and ‘severe’ tooth wear) are commonly used to determine and record the extent and severity of the presenting condition. However, such evaluations may be subjective.19 Quantitative assessments of the levels of tooth wear (usually performed using a numerically based clinical index applying agreed grading or scoring based on clinical descriptions) have the scope to offer greater intra- and inter-assessor agreement and help determine deterioration and progression with greater reliability.19
A multitude of tooth-wear indices have been described in the literature;20 however, the Basic Erosive Wear Examination (BEWE) proposed by Bartlett et al21 in 2008, has been reported to offer ease of use and has good acceptance among examiners when it is used to carry out erosive wear assessment.22 The BEWE applies the concepts of a partial scoring system, such as the Basic Periodontal Examination (BPE).
The prevention of tooth wear
Given the reported prevalence of tooth wear among all age groups, preventive measures involving the implementation of population-based strategies, such as the modification of the composition of soft drinks, emphasis on healthy nutrition and public health campaigns to increase the awareness of tooth wear, would appear logical.11,23 However, on the basis of insufficient evidence to support the recommendation for a population-level approach towards the prevention of tooth wear, 11 much of the available literature is focused on preventive measures aimed at the individual level: ‘secondary prevention.’23 Accordingly, these will involve the identification and removal of likely aetiological factors, and the professional recommendation for lifestyle changes, as well as any necessary further advice. The latter information should also be placed in the context of the biological and financial risks of not following the professional advice given, and the importance of the patient taking responsibility for the prevention of their tooth wear, must be stressed at the outset.
The role of fluoride in the prevention of tooth wear
The role of fluoride in the prevention of dental caries is well established. Although the benefits of fluoride application for the management of tooth wear have been demonstrated by some in vitro studies, evidence from clinical investigations is not as convincing.23 Nevertheless, it has been suggested that fluoride application is very likely to have a role in the prevention of erosive tooth wear, in particular, the prescription of acidic preparations, containing higher concentrations of fluoride.24 Preparations with monovalent fluorides, with lower to medium concentrations of fluoride and at neutral pH (e.g. those contained in most fluoride toothpastes and mouth rinses) are, however, likely to be of little or minimal benefit in the prevention of erosive tooth wear.24 The use of mouth rinses containing stannous fluoride may also offer some scope with the prevention of erosive tooth wear, as they have been shown to reduce solubility at the tooth surface level.24
Based on the available information,11 patients with signs of erosive tooth wear may be prescribed the twice-daily use of toothpaste containing at least 1450 ppm fluoride.11,25 Consideration should also be given to the use of high-fluoride concentration toothpastes for the protection of the enamel tissue (5000 ppm).26 While the professional application of high-concentration topical fluoride preparations (in the form of gels and varnishes) may be an option, this may not be practical, especially where there may be frequent episodes of acidic exposure.27
Preventive measures where a mechanical cause is suspected
Mechanical extrinsic tooth wear
Improper tooth brushing habits may culminate in abrasive, mechanical extrinsic tooth wear. Patient advice may therefore include the use of low abrasivity toothpastes,11 the use of appropriate toothbrushes, tooth brushing techniques and clear instructions about the use of a suitable level of force, the type of brush bristle and the frequency of tooth brushing. While it is often believed that the use of a harder stiffness bristle may be associated with an increased risk of tooth wear, Bizhang et al28 reported higher levels of dentine loss with the use of soft bristles (compared to hard bristle brushes). Turrsi et al29 reported the bristle stiffness to be an irrelevant factor for the risk of development of non-carious cervical lesions (NCCLs) when brushing with water or a lower-abrasive slurry; however, greater levels of wear were observed when using medium and hard toothbrushes with medium and higher abrasive slurries. Some toothpastes containing polymers (such as sodium hexametaphosphate and chitosan), which have the potential to be adsorbed into the dental hard tissues, may also offer further protection against tooth wear, and may be appropriate for patients with tooth wear.27 Abstaining from tooth brushing immediately after the intake of acidic foods or beverages, or immediately after an episode of vomiting (where recurrent vomiting has been diagnosed), to enable some remineralisation by saliva to take place and reduce the risk of further abrasion of the eroded tissues, is also advisable. 11
The consumption of certain types of abrasive foods, such as nuts and seeds (especially the nibbling of watermelon and pumpkin seeds between incisor teeth),30 may also contribute towards the pattern of observed abrasive tooth wear, as may habits, such as bone chewing, pencil biting, continual pipe smoking, or holding hairpins, also prove to be important for the prevention of tooth wear.
Dentine hypersensitivity is a symptom that may sometimes be reported with tooth wear. The application of dentine bonding agents and fissure sealant to eroded areas may be helpful in providing some level of protection and, concomitantly, help to reduce the symptoms of dentinal hypersensitivity. The latter may offer a longer level of protection from the progression of erosive tooth wear, for up to a period of 9 months.27,31
Mechanical intrinsic tooth wear
Mechanical intrinsic tooth wear (attrition-related tooth wear) may result from bruxism. The latter may be subdivided into awake bruxism (associated with jaw clenching), or nocturnal bruxism (associated with a tooth-grinding habit).32 Psychological stress and anxiety have been associated with the former variety of bruxism, while the latter is now classified as a sleep-related movement disorder. Stress management may therefore be appropriate for some patients diagnosed with awake bruxism.
Bruxism may also be exacerbated by the taking of recreational drugs, such as ecstasy (MDMA 3,4-methylenedioxymethamphetamine),32 which has also been associated with symptoms of a marked dry mouth that may last for a period of 6–8 hours and prompt users to consume copious amounts of carbonated drinks.33 Prescription medications, such as selective serotonin 5-hydroxytryptamine reuptake inhibitor (SSRI) antidepressants, have also been suggested to cause bruxism,32 especially when pharmacological therapy is commenced. Patients should be advised accordingly, and in the latter scenario, patients with concomitant signs of oral disease (or a potential higher risk of disease), advised to discuss alternative options with their medical practitioner.
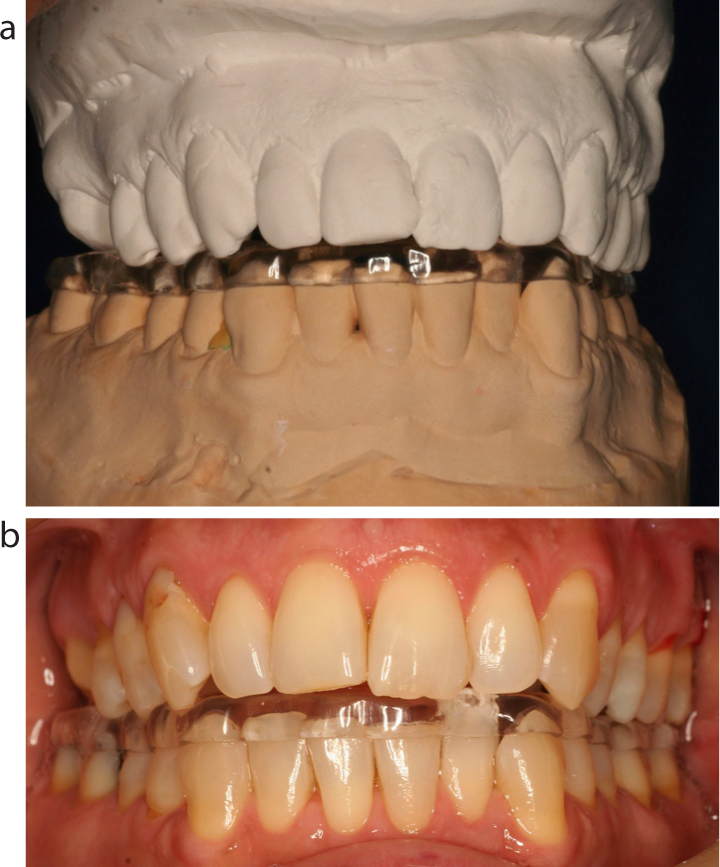
Splint therapy with full coverage appliances may be advised for patients diagnosed with bruxism,5,11 particularly those in the post-restorative phase to ensure long-term protection of the restorations against destructive occlusal forces. A variety of occlusal splints may be prescribed, including soft splints, hard splints and hybrid splints. However, compliance with splint therapy can be inconsistent. The decision to fabricate an appliance for the upper arch or lower arch is also very much based on operator preference. Hard, full coverage acrylic splints, such as a Michigan splint (Figure 2 a–f) or a Tanner appliance (Figure 3a, b) that are fabricated with a specific occlusal prescription, offer the added merits of facilitating the recording of centric relation (by allowing some reduction in the level of masticatory muscle spasm present), a reduction in the risk of unwanted tooth movement and enabling an assessment of a patient's acceptance of a planned change in their occlusal prescription, where restorative treatment may involve a change in the patient's occlusal vertical dimension.5 However, the skills required to fabricate such appliances and the affiliated costs, may limit their prescription in general dental practice.
Figure 2. (a) An upper Michigan full occlusal coverage stabilization splint. (b) The splint shown in (a) in situ positioned on the maxillary dentition of the patient. (c) Close up of the tooth contacts with the opposing mandibular teeth against the occlusal surface of the Michigan splint shown in (a) and (b). (d) The occlusal contacts have been marked on the splint using black articulating paper. Note the even centric stops and the excursive contacts anteriorly to give posterior disclusion. (e) As the patient's mandible protrudes the posterior teeth are discluded. (f) Patient in full protrusion with the posterior teeth discluded.Figure 3. (a) A lower Tanner full occlusal stabilization splint. (b) The splint shown in (a) in situ on the patient's mandibular dentition.
Caution is required when providing splints to patients with erosion from gastric reflux, as acidic substances may accumulate within the splint appliance. The use of a splint may, however, be considered beneficial in cases of a suspected erosive aetiology, where the splint may take the form of a soft vacuum-formed appliance that is modified to include reservoirs into which fluoride gels, or alkali in the form of milk of magnesia or sodium bicarbonate solution can be applied, respectively. The use of Recaldent-containing products (CPP-ACP: casein phosphopeptide-amorphous calcium phosphate) may also be helpful when attempting to facilitate improvement of the tooth tissues, because calcium and phosphate ions are released from the protein (CPP) when there is a drop in the pH level.30
Chemical extrinsic tooth wear
The observed increased prevalence of erosive tooth wear has been attributed to extrinsic factors, such as the frequent consumption of fruit juices and soft drinks. There has been a substantial increase in the consumption of soft beverages over the course of the past few decades.34,35 Unfortunately, because fruits and fruit juices are generally perceived to be healthier dietary options, many patients do not properly understand the risks of their copious consumption with respect to the initiation and propagation of tooth wear.
Where chemical extrinsic wear is suspected, further details about the patient's daily habits should be attained by requesting them to keep a clear record of their food and beverage intake, medication usage and the use of oral healthcare products, for a period of 4 days.27 A template diet sheet provided by the dental healthcare professional may prove helpful to ensure the recording of the appropriate details. This record should specify when and how much was ingested, and include some weekends and weekdays.36 The outcomes should be carefully analysed and discussed with patients or their guardians. It is paramount for patients to develop an understanding of their role in the prevention of tooth-wear progression and to establish realistic goals.
A number of acids, such as citric, phosphoric, lactic, tartaric, ascorbic and maleic acids, are contained in commonly consumed food and drinks.36 However, items containing citric acid, such as citrus fruits or juices (oranges and lemons), some soft drinks, canned foods, sports drinks and iced tea have a greater erosive potential as a result of this acid's ability to chelate calcium ions in saliva, thereby reducing the concentration of calcium available for the remineralisation of the tooth surface.27 It is therefore important for a dental professional to have some insight into the erosive potential of commonly consumed items. Although the pH values of some frequently consumed soft drinks have been well documented,37 the clinician should also have an awareness of their buffering capacity to properly understand their full erosive impact. A higher buffering capacity is associated with the need for a longer period of time to neutralise acidic exposure.27,36 Orange juice has both a higher pH and a relatively greater buffering capacity than some of the more popular carbonated drinks, and its erosive effects will, therefore, be relatively more prolonged in the oral cavity.
The concentration of calcium and phosphate ions has also been shown to have an effect on the extent to which an erosive food or drink may have on the level of tooth dissolution.36 In theory, a solution containing a higher concentration of calcium ions could potentially lower the overall erosive effect. The substitution of the usual soft beverage with one that has been supplemented with calcium has been shown help to reduce the erosive effect.38 However, the consumption of such drinks should be advised with some caution, due to potential possible side effects on the patient's general health.27
In general, where chemical extrinsic tooth wear is suspected, patients should be counselled to: avoid the frequent consumption of acidic foods and drinks; limit their consumption of erosive beverages to mealtimes; limit the number of fruit drinks to once a day; consider the use of a wide-bore straw placed towards the back of the mouth to ensure the drink does not make contact with teeth; consume cooled acidic drinks; avoid swirling the beverage in their mouths; refrain from taking small sips to complete the beverage over a prolonged period; and refrain from retaining the drink for a period of time prior to swallowing it.11,27,36 Diet advice sheets highlighting the foods and beverages associated with a higher risk to tooth wear and further proactive dietary advice to ensure optimal health gain, may also be of merit.
Where possible, water should be encouraged as a substitute and the health benefits of drinking water for the overall management of thirst and hydration also emphasised.27 Rinsing with water immediately after an acidic exposure may also help minimise the erosive impact. This may also be encouraged as a practical measure among wine tasters, where the regular use of fluoride-containing products and regular observation by a dental professional would also be advised.27
Where a lifestyle factor with the exposure to extrinsic acidic substrates may be aetiological (Table 2), patients should be counselled accordingly.
Chronic alcoholism may be associated with extrinsic and intrinsic chemical tooth wear, and again, multi-disciplinary management, with the involvement of dental practitioner may be necessary.27 There may also be the need to revert to the patient's physician when the pattern of tooth wear may be due to the prescription of medication with known erosive potential, or where the drug(s) may act to reduce the flow of saliva,11 as listed in Table 1.
Chemical intrinsic tooth wear
A plethora of medical conditions have been associated with intrinsic erosive tooth wear; some of which are listed in Table 1. It is of course beyond the scope of this article to address each of these conditions. However, given that the prevalence of gastro-oesophageal reflux disease (GORD) is estimated to be 65%,39 this condition perhaps warrants some further discussion. Symptoms associated with GORD may include heartburn, regurgitation, bloating, belching, dysphagia, nausea, Barrett's oesophagus, adenocarcinoma, non-cardiac chest pain, chronic cough, asthma, hoarseness, laryngitis, pharyngitis and erosive tooth wear.40 When a diagnosis of GORD is suspected by a dental practitioner, a referral to a medical practitioner is indicated. However, at times, convincing patients of a possible diagnosis of GORD and the need for a referral when there may be an absence of any prevailing symptoms or clear concerns, may prove challenging. For patients with GORD, simple and practical advice that may be offered by a dental professional to help manage their tooth wear, may include the following:40
Recommending the consumption of smaller meals and refraining from larger meals especially before sleeping;
Adjusting the sleeping position by raising the head over night;
Reducing alcohol consumption;
Smoking cessation;
Weight loss;
Stress management;
Caution with spicy foods,41 citrus foods and coffee.
Proton pump inhibitor (PPI) drugs that inhibit gastric reflux are often used as the first line of pharmacological treatment for GORD; however, there can be long-term side effects associated with taking these drugs.40 The use of sugar-free and fluoride- or carbamide-containing chewing gums may also help to stimulate salivary flow and be of help with the management of patients with GORD.
Antacids, or the use of appropriate preparations containing bicarbonate, may also be advised for patients diagnosed with GORD, as well as during other instances, when there may be a concomitant reduction in the intra-oral pH due to intrinsic acid, such as when happens with recurrent vomiting and heartburn. For patients with recurrent vomiting, rinsing their mouths immediately after an episode has taken place with water, milk, sodium bicarbonate solution or a fluoride-containing mouthwash may be also be advisable.
Dry mouth
As saliva has a key role in the prevention of tooth wear, dry mouth may put patients at a higher risk for tooth wear. The quality and quantity of saliva are critical factors. For patients with hyposalivation and a higher risk for tooth wear, simple preventive measures may include advice to regularly sip water, chew gum, consume hard cheese, use high-viscosity (non-low pH) saliva substitutes that may also contain calcium, phosphate and fluoride, and rinsing with water (or an appropriate mouth rinse) after acidic exposure.33 Some patients with dry mouth may opt to consume higher quantities of acidic sweets to help with their symptoms; this may have a profound effect on their oral health. For patients with more severe forms of dry mouth, referral to a colleague with expertise in this field may be necessary, when, for more severe cases of xerostomia (that may be associated with Sjögren's syndrome, or radiation to the head and neck areas), drugs such as pilocarpine may be prescribed.
Monitoring tooth wear
Having diagnosed tooth wear, undertaken a risk assessment and provided the necessary preventive advice for patients, vigilant professional monitoring is required. During periodic reassessment, a careful patient history must be taken, as well as an assessment of the progression of the tooth wear and the patient's compliance with the prescribed preventive plan. The periodic use of a clinical index (that may also be applied alongside indirect methods, such as the use of study models, 3D digital casts, or clinical photographs) may help to identify whether the wear has been progressive. Digital intra-oral scanning devices may also be of merit for this purpose. Where progressive tooth wear is suspected, further investigation of its aetiology may be required, as may the need to consider a referral to a dental or medical colleague, and/or some revision of the prescribed preventive plan.
Some patients will, of course, fail to comply with the advice given, and these individuals can be challenging to manage. However, the temptation to embark on often costly and complex restorative treatment must be given very careful consideration if the clinician is not satisfied that the preventive strategy has been effective. The prognosis for the restored dentition may be significantly compromised if the likely aetiological factors are not properly identified and effectively managed.42
Conclusion
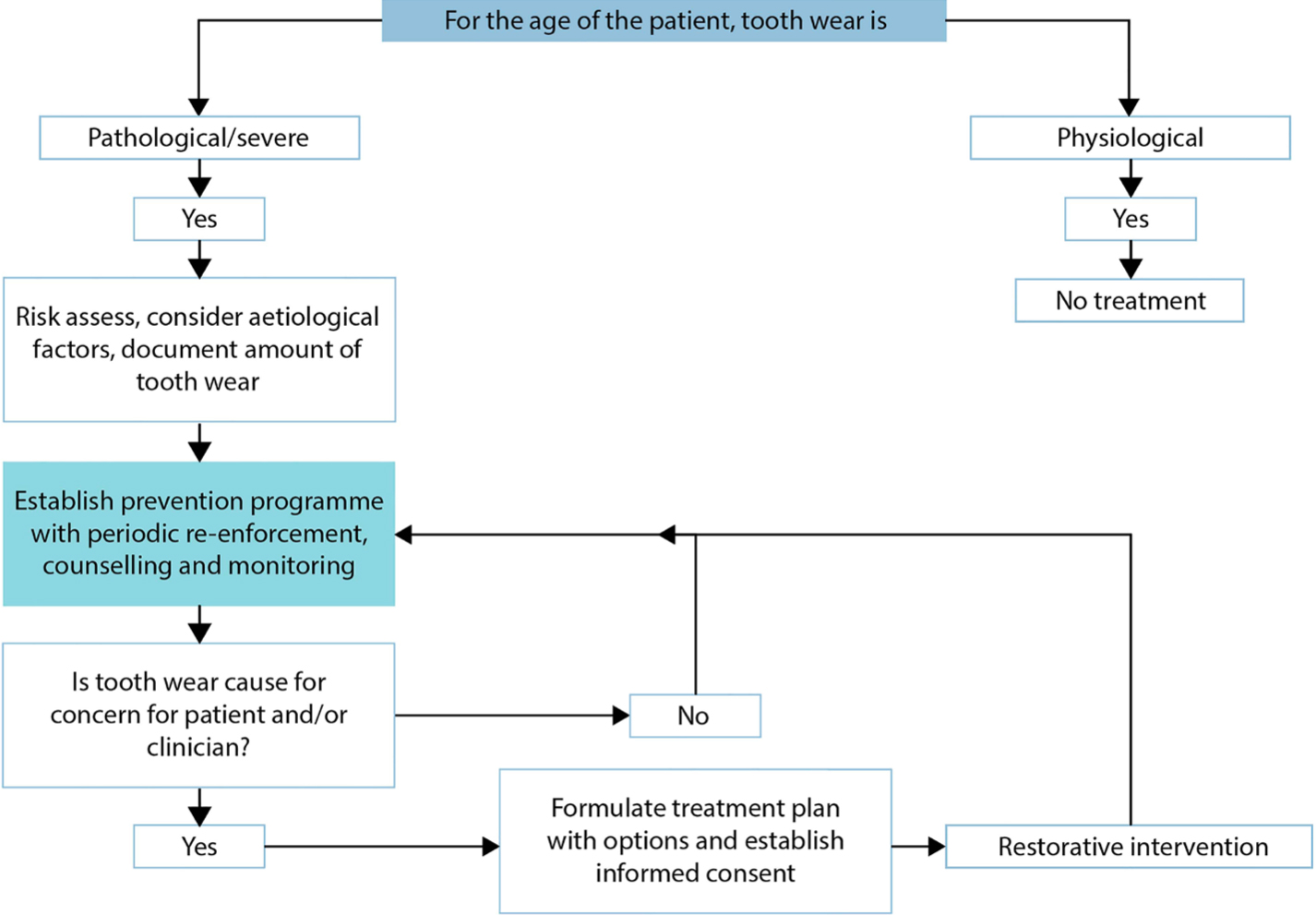
With tooth wear being a common clinical diagnosis established in clinical practice, an effective prevention protocol is an integral step in its management (Figure 4). An understanding of its aetiology and preventive agents, protocols and strategies enables the general practitioner to establish patient care to prevent or manage it if it has become established or has been restored.
Figure 4. Flowchart to highlight the integral role of prevention in the management of tooth wear.