This case describes the presentation of dens evaginatus on a maxillary central incisor in an 8-year-old Caucasian male, its subsequent monitoring and later management. Dens evaginatus is a dental anomaly most commonly noted as an accessory tubercle on the occlusal surface of premolars and the palatal aspect of incisors as a talon cusp. Complications can result in loss of pulp vitality, sometimes causing periapical periodontitis. Clinicians should be aware of the presentation and the advantages of different approaches to the management of dens evaginatus.
CPD/Clinical Relevance: To raise awareness of dens evaginatus in dental professionals working in primary and secondary care.
Article
Dens evaginatus (DE) is a rare dental developmental anomaly that is found in teeth where the enamel outer surface appears to have an anatomic anomaly, or an extra cusp in the form of a tubercle, or both. The tubercle is composed of an outer enamel layer, a dentine core and prominent pulp tissue, which can extend to the main part of the pulp.1
Upper incisors are less frequently affected than premolars, which are the most common teeth to display extra cusps. These can occur bilaterally and can be symmetrical. The occlusal surfaces of posterior teeth and labial or palatal surfaces of anterior teeth are commonly affected.2,3
The prevalence of DE ranges from 0.06% to 7.7%, depending on race.4,5
DE occurs more commonly in Asian patients6 and has been reported to have higher rates amongst Chinese7 populations. DE is more common in men than women,5 and occurs more frequently in the mandible than the maxilla.8 Patients with Ellis-van Creveld syndrome, Mohr syndrome, Rubinstein-Taybi syndrome and Sturge-Weber syndrome are at a higher risk of having DE.9–12
Cause
The exact aetiology of DE remains unclear and it might be an isolated anomaly. However, it is thought to arise from an aberrant folding of the inner enamel epithelium and subjacent ectomesenchymal cells of the dental papilla into the stellate reticulum of the enamel organ during the bell stage of tooth development.3,4
Mitchell first reported a horn-like projection of a maxillary central incisor in 1892.13 Since then, the literature has offered varying terms for what is now known as DE, including tuberculated premolar, evaginated odontoma, Leong's premolar, occlusal enamel pearl, odontome of axial core type and talon cusp.
Dens evaginatus can be associated with a number of dental issues and anomalies including:14,15
Occlusal disharmony;
Aesthetic problems;
Supernumerary teeth;
Odontomes;
Megadonts;
Shovel-shaped incisors with prominent marginal ridges (Figure 1);
Figure 1. Shovel-shaped UR1 with prominent marginal ridges and a labial groove.
Diagnosis
The appearance of DE usually makes the diagnosis easy, but knowing exactly what to do about the pulpal status at any given time can be more difficult, particularly when there are no signs or symptoms of pulpal necrosis.8 In assessing a developing tooth with DE, it can be problematic to differentiate between a periapical lesion due to a tooth being dead and the normal periapical radiolucency of an immature apex.
Sensibility testing on immature teeth can be misleading, as they are known to give unreliable results. Occasionally, DE can be seen radiographically prior to eruption.16
Case Report
A young Caucasian male presented with his parents when he was about 8 years old. It was obvious what the problems were (Figures 2, 3 and 4). The upper right central incisor was malformed with an unsightly and irregular, rough-looking, disto-labial surface with an obviously protruding pearl. Explanations were given to the patient and his concerned parents about the ‘dens evaginatus’ condition. The acronym ‘BRAN’ was used to draw attention to the Benefits, Risks Alternative (doing) Nothing.
Figure 2. View of the upper right central incisor (UR1) showing DE on the labial surface.Figure 3. Lateral view of UR1 showing labial extent of the tubercle.Figure 4. Close up view showing UR1.
After some discussions ‘doing nothing’ was chosen because both the patient and parents were happy to wait and see to allow further pulpal development. It was agreed that they would report any changes, or if he was getting teased at school. Many years passed without any problems and he had fixed orthodontic treatment to improve his malocclusion.
When he was 15 years old, the appearance of the upper right central incisor was troubling the patient and, while part of the enamel pearl was no longer present, it was decided to tidy the appearance up by adding direct resin composite to the labial aspect of the malformed upper right central incisor tooth (Figure 5).
Figure 5. Labial view following orthodontic treatment and loss of the tubercle.
Sensibility testing revealed that the upper right central incisor was vital. The root had completed growth and the radiograph showed that there was no sign of a periapical radiolucent area.
Following explanations and consent, topical anaesthetic was applied. The surface of the upper right central incisor was roughened very gently with a diamond bur to get down to a surface that could be made reactive. It was then etched for 20 seconds with standard 37% phosphoric acid gel with only cotton wool roll as isolation (Figure 6). This was deliberate because the use of a rubber dam involves dehydrating the teeth, which does not help to choose the correct colour of resin composite for the direct bonding.
Figure 6. UR1 being acid etched.
The phosphoric acid was evacuated from the surface and the area was washed and dried to produce visibly frosty enamel (Figure 7). That process is called ‘check etching’. It is important to check that a frosty etched enamel appearance has been achieved before proceeding further. If there is any doubt about the surface on to which one is attempting to bond, the etching process needs to be repeated.
Figure 7.
A ‘gold standard’ 3 bottle system was therefore used for the bonding system (Allbond 2®, Bisco, USA). The hydrophilic resins were applied and air dried (Figure 8).
Figure 8. Applying bonding agent to UR1.
The unfilled resin was then applied, blown to a thin layer and cured for 15 seconds. Charisma® shade A1 was used freehand. The result can be seen in Figures 9 and 10 and the patient and parents declared themselves happy with the result. There was no post-operative pain or any complications.
Figure 9. Post-op restoration UR1.Figure 10. Close-up view of UR1 restored with composite restoration.
A second case highlights the issues that can arise with late presentation of DE. Figure 11 shows a maxillary left first molar with a previously fractured DE on the occlusal table.
Figure 11. The maxillary first permanent molar has a pink hue visible through the occlusal surface; evidence of the inflammatory process as a result of DE.
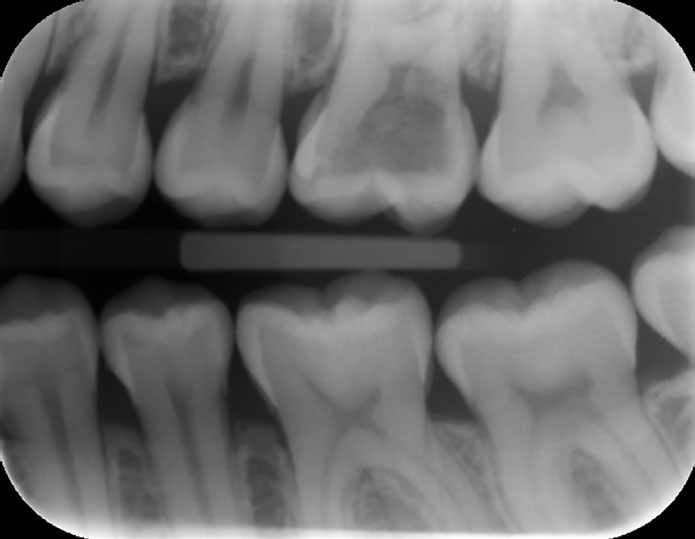
Radiographic examination (Figures 12, 13) revealed gross coronal resorption due to the pulpal necrosis caused by a fractured tubercle.
Figure 12. Bitewing radiograph showing a radiolucency extending through the enamel to the occlusal table, indicating the pulpal extension into the fractured tubercle.Figure 13. Periapical radiograph showing large radiolucent abnormality within the coronal aspect of the UL6. The radiolucency extends from the occlusal table to the base of the pulp chamber.
The tooth has a pink hue due to the vascular changes as a result of the fractured tubercle. In this case, endodontic treatment was required. After gaining access to the pulp chamber complex of the UL6, extensive hyperaemic tissue was removed, and a significant pulp stone noted to be present over the canal orifices. The pulp stone was removed with ultrasonic instrumentation and three canal orifices were located. Further exploration of the access cavity confirmed an approximate 0.5 mm communication distally between the pulp chamber and mouth at the level of the cemento-enamel junction. It was confirmed that the communication was clear of inflammatory tissue and it was sealed with a zinc-oxide eugenol-based material. This was chosen in preference to mineral trioxide aggregate (MTA) as it was felt that the MTA might be susceptible to being washed away by local saliva during its setting process (approximately 24 hours). The pulp chamber was dressed with non-setting calcium hydroxide paste and sealed with a temporary restoration. At a subsequent appointment, access to the pulp chamber and canals was regained, the restoration used to seal the distal perforation was intact and the seal was confirmed. The canals were shaped using a combination of hand and rotary files. Extensive exploration for an MB2 canal using microscopic illumination and magnification was carried out and no trace was found. Sodium hypochlorite was used to irrigate throughout. Following shaping, obturation was completed using a warm vertical condensation technique and an amalgam Nayyar core was placed. This case highlights long-term complications of late diagnosis of DE and importance of early diagnosis and intervention, where it is appropriate.
Classification
A number of classifications have been described to categorize DE. Some of the classifications are as follows.
Lau's classification, which is based on their anatomical shapes:18
Smooth;
Grooved;
Terraced;
Ridged.
Oehler's et al classification is based on the histology of the pulp contents within the tubercle:19
Wide pulp horns (34%);
Narrow pulp horns (22%);
Constricted pulp horns (14%);
Isolated pulp horn remnants (20%);
No pulp horn (10%).
Schulge's classification described five categories of DE based upon the location of the tubercle:7
A cone-like enlargement of the lingual cusp;
A tubercle on the inclined plane of the lingual cusp;
A cone-like enlargement of the buccal cusp;
A tubercle on the inclined plane of the buccal cusp;
Tubercle arising from the occlusal surface obliterating the central groove.
Hattab et al's classification, described the features based on the formation and extent of DE and is limited to anterior teeth:3
Type 1 – Talon, a well-defined additional cusp that projects palatally and extends at least half the distance from the cemento-enamel junction (CEJ) to the incisal edge (Figure 14).
Type 2 – Semi-talon, an additional cusp that extends less than half the distance from the CEJ to the incisal edge.
Type 3 – Trace talon, prominent cingula.
Figure 14. Type 1 talon cusp based on the Hattab et al classification.
Management
Early identification can allow for a number of preventive strategies. If the tooth is asymptomatic, and unlikely to encounter occlusal trauma, then no treatment may be required.20 A preventive regimen, including oral hygiene instruction, application of neutral topical fluoride and application of fissure sealant,5,21,22 can be used alongside regular recall.
If the tooth is likely to encounter occlusal trauma, then a more invasive approach may be required. This can include gradual selective cusp grinding.23 The aim of this is to induce formation of secondary and tertiary dentine and hopefully cause closure of the pulp horn. Cusp grinding can be unpredictable and cause exposure of the pulp. It should be considered when there is no expected pulpal extension into the tubercle. The patient will require numerous visits with this approach and the possibility of sensitivity or causing pulpal death.
For teeth with a vital pulp, direct resin composite bonded around the vulnerable projection can be used to reinforce the tubercle.24 Pulp and periapical tissues assessment can be completed annually. When there is adequate pulp recession, the tubercle can be removed and tooth can be restored. This may need to be completed in conjunction with adjustment of the opposing occluding tooth. In theory at least, one could consider prophylactic pulp capping,25 using mineral trioxide aggregate (MTA) or other novel bio-ceramic materials. In that scenario, tooth vitality might be maintained via dentine bridge formation.26
For immature teeth with an inflamed pulp, a shallow MTA pulpotomy could be performed and the tooth then restored with contrasting colour conventional glass ionomer, possibly along with some superficial contrasting colour composite. For mature teeth with inflamed or necrotic pulps, conventional root canal therapy can be completed, and the teeth restored. If the teeth are discoloured, the teeth can be restored with contrasting colour conventional glass ionomer cement, in case re-entry for inside/outside bleaching is ever required.27 For necrotic immature teeth with open apices, apexification should be completed with the use of MTA or an appropriate bio-ceramic material and restored appropriately. In some cases, where there is gross infection, failed endodontic treatment or for orthodontic reasons, extraction can be considered.24
Discussion
Dens evaginatus is a rare dental anomaly which commonly presents as a tubercle on the labial surface of anterior teeth. It is usually detected by clinical examination alone. If the problem occurs on the cingulum/occlusal surface of the teeth, then the extra cusp can cause an occlusal interference or displace the affected tooth and/or the opposing teeth. The presence of the tubercle can irritate the tongue when speaking or eating and, if present on the biting surface the extra cusp, can fracture easily.2,8,22 It is important to diagnose DE early, at which point close monitoring, or any necessary intervention, can be employed to improve long-term outcomes. Late diagnosis can lead to pulpal complications if and when the tubercle fractures. Pulp involvement may present as pulpitis, pulpal necrosis, or apical periodontitis. The patient may not always experience symptoms.
Conclusion
The aim of this report is to increase awareness amongst practitioners of the importance of early detection and conservative management strategies. Hopefully, this will prevent the need for complex treatment and ultimately improving care for patients with DE.