Guthrie RC, DiFiore PM. Treating the cracked tooth with a full crown. J Am Dent Assoc. 1991; 122:71-73
Opdam NJ, Roeters JJ, Loomans BA, Bronkhorst EM. Seven-year clinical evaluation of painful cracked teeth restored with a direct composite restoration. J Endod. 2008; 34:808-811
Davis R, Overton JD. Efficacy of bonded and nonbonded amalgam in the treatment of teeth with incomplete fractures. J Am Dent Assoc. 2000; 131:469-478
Signore A, Benedicenti S, Covani U, Ravera G. A 4- to 6-year retrospective clinical study of cracked teeth restored with bonded indirect resin composite onlays. Int J Prosthodont. 2007; 20:609-616
Abbott P, Leow N. Predictable management of cracked teeth with reversible pulpitis. Aust Dent J. 2009; 54:306-315
Krell KV, Rivera EM. A six year evaluation of cracked teeth diagnosed with reversible pulpitis: treatment and prognosis. J Endod. 2007; 33:1405-1407
Kang SH, Kim BS, Kim Y. Cracked teeth: distribution, characteristics, and survival after root canal treatment. J Endod. 2016; 42:557-562
Kim SY, Kim SH, Cho SB, Lee GO, Yang SE. Different treatment protocols for different pulpal and periapical diagnoses of 72 cracked teeth. J Endod. 2013; 39:449-452
Banerji S, Mehta SB, Kamran T, Kalakonda M, Millar BJ. A multi-centred clinical audit to describe the efficacy of direct supra-coronal splinting – a minimally invasive approach to the management of cracked tooth syndrome. J Dent. 2014; 42:862-871
Tan L, Chen NN, Poon CY, Wong HB. Survival of root filled cracked teeth in a tertiary institution. Int Endod J. 2006; 39:886-889
Kontakiotis EG, Filippatos CG, Stefopoulos S, Tzanetakis GN. A prospective study of the incidence of asymptomatic pulp necrosis following crown preparation. Int Endod J. 2015; 48:512-517
Valderhaug J, Jokstad A, Ambjornsen E, Norheim PW. Assessment of the periapical and clinical status of crowned teeth over 25 years. J Dent. 1997; 25:97-105
Alley BS, Gray Kitchens G, Alley LW, Eleazer PD. A comparison of survival of teeth following endodontic treatment performed by general dentists or by specialists. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 98:115-118
Alkhalifah S, Alkandari H, Sharma PN, Moule AJ. Treatment of cracked teeth. J Endod. 2017; 43:1579-1586
Hood JA. Biomechanics of the intact, prepared and restored tooth: some clinical implications. Int Dent J. 1991; 41:25-32
Ricucci D, Siqueira JF, Loghin S, Berman LH. The cracked tooth: histopathologic and histobacteriologic aspects. J Endod. 2015; 41:343-352
Eltit F, Ebacher V, Wang R. Inelastic deformation and microcracking process in human dentin. J Struct Biol. 2013; 183:141-148
Forster A, Braunitzer G, Toth M, Szabo BP, Frater M. In vitro fracture resistance of adhesively restored molar teeth with different MOD cavity dimensions. J Prosthodont. 2019; 28:e325-e331
De Munck J, Van Meerbeek B, Yoshida Y, Inoue S, Vargas M, Suzuki K Four-year water degradation of totaletch adhesives bonded to dentin. J Dent Res. 2003; 82:136-140
Tezvergil-Mutluay A, Pashley D, Mutluay MM. Long-term durability of dental adhesives. Curr Oral Health Rep. 2015; 2:174-181
Panahandeh N, Torabzadeh H, Ziaee N, Mahdian M, Tootiaee B, Ghasemi A. The effect of composite thickness on the stress distribution pattern of restored premolar teeth with cusp reduction. J Prosthodont. 2017; 26:440-445
Lee MR, Cho BH, Son HH, Um CM, Lee IB. Influence of cavity dimension and restoration methods on the cusp deflection of premolars in composite restoration. Dent Mater. 2007; 23:288-295
Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in relation to configuration of the restoration. J Dent Res. 1987; 66:1636-1639
Kois DE, Chaiyabutr Y, Kois JC. Comparison of load-fatigue performance of posterior ceramic onlay restorations under different preparation designs. Compend Contin Educ Dent. 2012; 33:(2)2-9
Coulter J, McCracken G. Complications in managing tooth wear; exploring a potential pitfall of using the Dahl approach – a case study. Dent Update. 2018; 45:320-326
Banerji S, Mehta SB, Millar BJ. The management of cracked tooth syndrome in dental practice. Br Dent J. 2017; 222:659-666
Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010; 54:249-273
Lertchirakarn V, Palamara JE, Messer HH. Patterns of vertical root fracture: factors affecting stress distribution in the root canal. J Endod. 2003; 29:523-528
Mitov G, Anastassova-Yoshida Y, Nothdurft FP, von See C, Pospiech P. Influence of the preparation design and artificial aging on the fracture resistance of monolithic zirconia crowns. J Adv Prosthodont. 2016; 8:30-36
Fennis WM, Kuijs RH, Kreulen CM, Verdonschot N, Creugers NH. Fatigue resistance of teeth restored with cuspal-coverage composite restorations. Int J Prosthodont. 2004; 17:313-317
Majd H, Viray J, Porter JA, Romberg E, Arola D. Degradation in the fatigue resistance of dentin by bur and abrasive air-jet preparations. J Dent Res. 2012; 91:894-899
Ivancik J, Neerchal NK, Romberg E, Arola D. The reduction in fatigue crack growth resistance of dentin with depth. J Dent Res. 2011; 90:1031-1036
Mujdeci A, Gokay O. The effect of airborne-particle abrasion on the shear bond strength of four restorative materials to enamel and dentin. J Prosthet Dent. 2004; 92:245-249
Rosatto CMP, Bicalho AA, Verissimo C, Braganca GF, Rodrigues MP, Tantbirojn D Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J Dent. 2015; 43:1519-1528
Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013; 38:618-625
Abouelleil H, Pradelle N, Villat C, Attik N, Colon P, Grosgogeat B. Comparison of mechanical properties of a new fiber reinforced composite and bulk filling composites. Restor Dent Endod. 2015; 40:262-270
Mamoun JS, Napoletano D. Cracked tooth diagnosis and treatment: An alternative paradigm. Eur J Dent. 2015; 9:293-303
Kuijs RH, Fennis WM, Kreulen CM, Roeters FJ, Verdonschot N, Creugers NH. A comparison of fatigue resistance of three materials for cusp-replacing adhesive restorations. J Dent. 2006; 34:19-25
Yamamoto T, Nakamura Y, Nishide A, Kubota Y, Momoi Y. Contraction stresses in direct and indirect composite restorations compared by crack analysis. J Adhes Dent. 2013; 15:47-54
Fennis WM, Kuijs RH, Barink M, Kreulen CM, Verdonschot N, Creugers NH. Can internal stresses explain the fracture resistance of cusp-replacing composite restorations?. Eur J Oral Sci. 2005; 113:443-448
Meriwether LA, Blen BJ, Benson JH, Hatch RH, Tantbirojn D, Versluis A. Shrinkage stress compensation in composite-restored teeth: relaxation or hygroscopic expansion?. Dent Mater. 2013; 29:573-579
Heintze SD, Rousson V. Clinical effectiveness of direct class II restorations – a meta-analysis. J Adhes Dent. 2012; 14:407-431
Tjaderhane L. Dentin bonding: can we make it last?. Oper Dent. 2015; 40:4-18
Peumans M, De Munck J, Van Landuyt KL, Poitevin A, Lambrechts P, Van Meerbeek B. Eight-year clinical evaluation of a 2-step selfetch adhesive with and without selective enamel etching. Dent Mater. 2010; 26:1176-1184
Van Meerbeek B, Yoshihara K, Yoshida Y, Mine A, De Munck J, Van Landuyt KL. State of the art of selfetch adhesives. Dent Mater. 2011; 27:17-28
Pashley DH, Tay FR, Breschi L, Tjaderhane L, Carvalho RM, Carrilho M State of the art etch-and-rinse adhesives. Dent Mater. 2011; 27:1-16
Cardoso MV, de Almeida Neves A, Mine A, Coutinho E, Van Landuyt K, De Munck J Current aspects on bonding effectiveness and stability in adhesive dentistry. Aust Dent J. 2011; 56:31-44
Lynch CD, McConnell RJ. The cracked tooth syndrome. J Can Dent Assoc. 2002; 68:470-475
This article follows on from Part 1 which looked at the pathogenesis and diagnosis of cracked tooth syndrome (CTS). It combines a review of the available evidence with a discussion of established and more modern concepts of management, aiming to provide a clear, rational approach to the predictable management of CTS with the aid of case studies and a decision-tree.
CPD/Clinical Relevance: Allows the clinician to manage CTS predictably.
Article
Oliver Bailey
There are no universally accepted guidelines for managing cracked tooth syndrome (CTS). Contemporary approaches are quite diverse and have included operative crack removal, mechanical encirclement of the tooth, adhesive intra-coronal splinting, or splinting with extra-coronal coverage retained either adhesively or mechanically. In addition, restorations have been fabricated either in the mouth (directly), or in the laboratory (indirectly).1,2,3,4,5 Understandably, choosing the best option can be confusing.
Treatment of CTS aims to predictably restore and maintain a functional asymptomatic tooth, with a vital pulp, by stabilizing the crack, or cracks.
Clinical evidence base
The evidence base on management options for CTS is limited, with much experimental data missing.
Direct composite
A study involving 41 patients with CTS compared direct composite placed either intra-coronally, or overlaying the affected cusp following its reduction.2 In the overlay group (n = 21), 0% required pulpectomy and restoration survival was 100% at 7 years follow-up. In the intra-coronal group (n = 20), three teeth required pulpectomy (15%), two within 6 months and one at 7 years. Two of these teeth subsequently required extraction due to vertical fractures. Eighty-five percent of restorations survived in this group and the failures were non-catastrophic. Excluding the teeth requiring pulpectomy, a minority of teeth suffered from residual thermal sensitivity in both groups, but pain on biting resolved in all teeth.
Amalgam
Another study compared full occlusal coverage amalgams retained either mechanically with pins (n = 20), or adhesively with resin (n = 20) for the management of CTS.3 One tooth in the mechanically retained group (5%) required pulpectomy at 1 year and cold sensitivity remained similar to baseline levels. In the adhesive retention group, 0% required pulpectomy and cold sensitivity was reduced over the same period. Pain on biting resolved in all teeth and all restorations were intact at 1 year. Amalgam use has recently been phased-down, however and, with a complete phase-out on the horizon, it is likely to be unavailable for use and will not be considered further.
Indirect composite
Seven percent of teeth diagnosed with CTS that were treated with indirect composite onlays (n = 43), following initial stabilization with intra-coronal restoration replacement with direct composite, required pulpectomy within 6 months. Restoration survival was 93% during the follow-up period of 4–6 years. A small minority had persistent thermal sensitivity.4
Crowns
A study employing permanent or temporary crowns to manage CTS found that 21% of permanently crowned teeth required pulpectomy within 6 months of treatment (n = 127). The effects of crowning on CTS symptoms were not reported.6 In the temporary crown studies, the percentage of teeth requiring pulpectomy varied from 11% at 1 year (n = 28)1 to 29% (group size n = 38)7 and 43% (group size n = 21).8 The reporting of changes in symptoms was very limited in all of these studies, and the time frame from initiation of treatment to the requirement for pulpectomy was not specified in the latter two papers. Restoration survival was not reported in any of the studies.
Crack removal
Another study involved drilling out the visible cracks in teeth with CTS (n = 100), before placing a Ledermix lining and various glass ionomer cement-based temporary restorations.5 Fifteen percent required pulpectomy at this initial stage of stabilization and a further 5% required pulpectomy subsequently. The teeth were definitively restored with crowns or overlays, but the proportions were not reported, and there was a high level of participant dropout in the study. Restoration survival and post-treatment thermal sensitivity were not reported.
Direct composite splint (DCS) use with various definitive restorations
Minimally invasive management of CTS with a DCS was reported in an audit involving 151 patients.9 CTS was diagnosed by the disappearance of symptoms following application of a non-bonded DCS, as described in the first article of this series. The DCS was then adhesively bonded in supra-occlusion, resulting in disclusion of other teeth. Eleven patients fulfilling the inclusion criteria did not consent to bonding of the DCS, so had alternative management.
Tooth contacts were then allowed to re-establish over time through relative axial movement prior to definitive restoration. The restorations varied in design, but a large majority were direct composite onlays. Management therefore involved two stages, but meant that no or minimal occlusal reduction was required, as space was created by intrusion and extrusion of teeth. Three percent of patients reported intolerance to the DCS and 10% required replacement or repair of the DCS, but all of these complications were evident within the first 2 weeks following bonding. Seven percent of the teeth went on to develop irreversible pulpitis and 3% suffered complete fracture, while 3% of patients did not re-establish occlusal contacts within 3 months but were asymptomatic.9 While the follow-up interval is short and the number of patients affected is low, the management of cases where contacts do not re-establish, and the occlusion is disrupted by uncontrolled tooth movements, may be complex and costly. Simply removing the DCS may not allow full re-establishment of the occlusion. Bonding a DCS was not advised in a number of situations highlighted in Table 1 (blue text).9 Restoration survival and post-treatment thermal sensitivity were not reported.
Unable to tolerate non-bonded DCS
Antagonistic tooth vulnerable to fracture
Active periodontitis
TMD
Previous orthodontics
Reduced eruptive potential
Anterior open bite
Implants
Fixed bridges
Bony ankylosis
Class III incisal relationships
Prominent bony exostoses
Large horizontal RCP-ICP discrepancy
Already heavily restored tooth that would benefit from cuspal coverage even in the absence of a crack or cracks
Only 85% of root canal treated permanent teeth with cracks survived for 2 years in a tertiary care setting (n=50). These all initially presented as CTS and were initially managed with a cemented orthodontic band in an attempt to stabilize the cracks. The teeth were restored with crowns, or amalgam cores, with retention of the cemented orthodontic bands. The number of teeth receiving each restoration was not specified, however, and the relationship to tooth survival was not reported.10 Ninety percent of cracked teeth receiving root canal treatment from an endodontist survived for 2 years when subsequently restored with crowns (n = 88). This also included teeth that were diagnosed as non-vital at presentation however, which is not CTS. Teeth with an initial probing depth >6 mm had a statistically significantly lower survival of 74% compared to 97% in the remainder of the teeth.7
Summary of findings
Firm conclusions are difficult to make on the basis of limited data. Covering the affected cusp(s) with an adhesive restoration appears to be the most effective option for managing CTS in terms of resolving symptoms, reducing the need for pulpectomy and optimizing restoration survival in the short to medium term. Where specifically assessed, a minority of teeth with CTS showed persistent residual thermal sensitivity. Either attempting to drill out the visible cracks completely (see later discussion), or preparation of a tooth with CTS for a crown appears to increase the need for pulpectomy, over and above the generalized reported risk of loss of vitality associated with crowning teeth.11,12 Use of a bonded DCS to gain inter-occlusal space can be successful in resolving symptoms and minimizing the need for pulpectomy, but the technique can have complications and is not appropriate for everyone. Cracked teeth requiring root canal treatment appear to have a reduced prognosis compared to the reported general success of root canal treatment when managed by endodontists13 and the presence of a probing depth >6 mm is a negative prognostic factor.
Concepts of CTS management
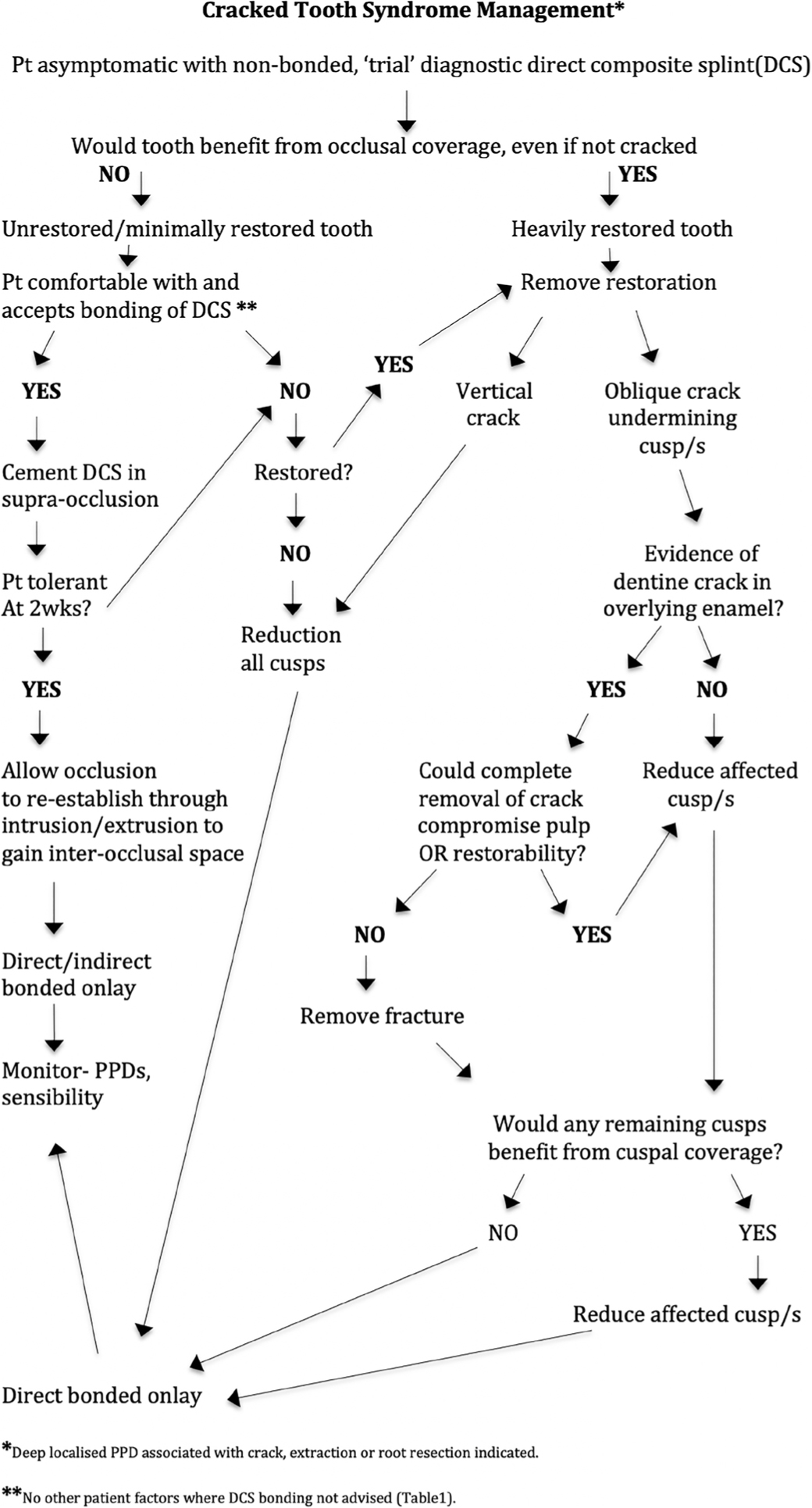
A decision-tree has been developed to aid decision-making in the management of CTS (Figure 1). This will be explained through the use of successfully treated case studies and a discussion of the relevant concepts.
Figure 1. CTS management decision-tree.
Effective management requires consideration of:
Rational retention of tooth structure;
Preparation optimization;
Restorative implications and choices.
Rational retention of tooth structure
This involves decision-making on:
The restorative status of the tooth;
Retention versus removal of cracks;
Provision of cuspal coverage.
1. The restorative status of the tooth
Classifying the restorative status of a restored tooth is difficult. For the purpose of managing a tooth with CTS, it is important to decide whether the existing restoration puts the tooth at an increased risk of fracture, even if the crack was not present. A tooth deemed to be at increased risk would be classified as ‘heavily restored’. The remaining restored teeth would be classified as ‘minimally restored’.
Defining which teeth are at risk of fracture, in the absence of a symptomatic crack, is very subjective, and a complex clinical judgement based on multiple factors. These include the presence of asymptomatic cracks, residual cusp dimensions, depth and configuration of the cavity, type and quality of dental substrate, restorative technique, position of the tooth in the arch, the nature and force of functional and potential parafunctional loading, periodontal support, alongside harder to define patient and dentist-related factors.14,15
Assessing fracture risk prior to removing a restoration involves unknowns, so is generally based on gauging whether any remaining cusp tips are likely to be supported by dentine, the depth of the restoration, and whether the marginal ridges are intact and supported by dentine.15
These factors are discussed in the case studies to help illustrate the decision-making process. Figures 2a, 4a, 6a and 7a show examples of where teeth were classified as being heavily restored, or minimally restored and the rationale explained.
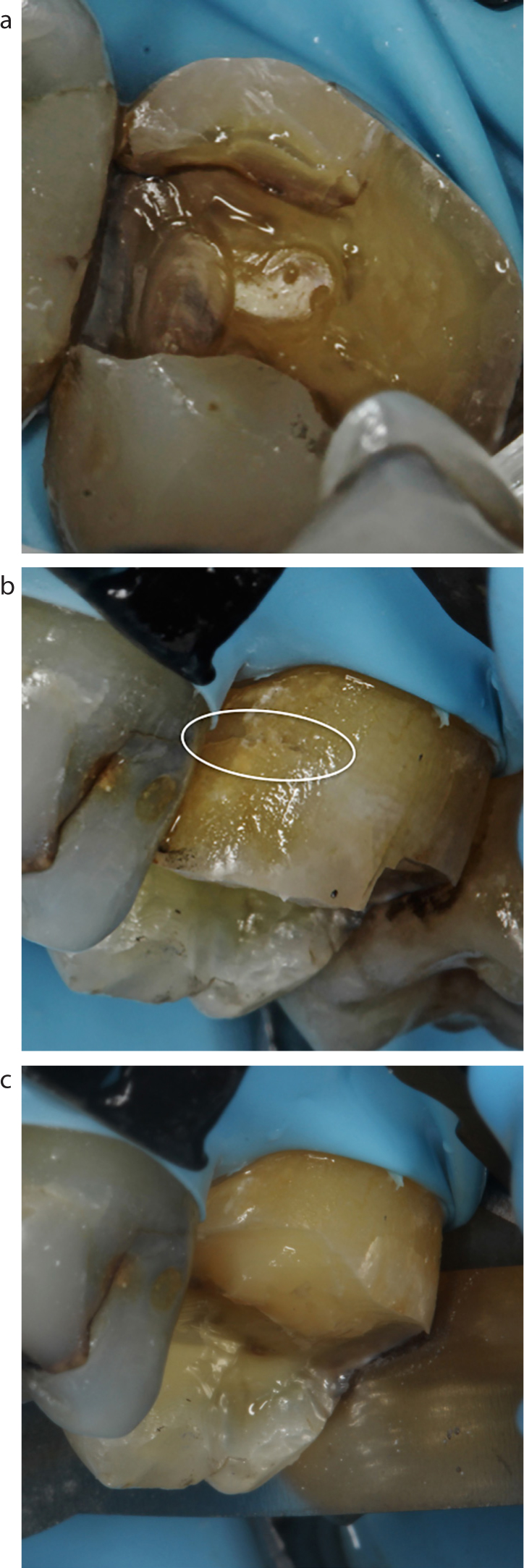
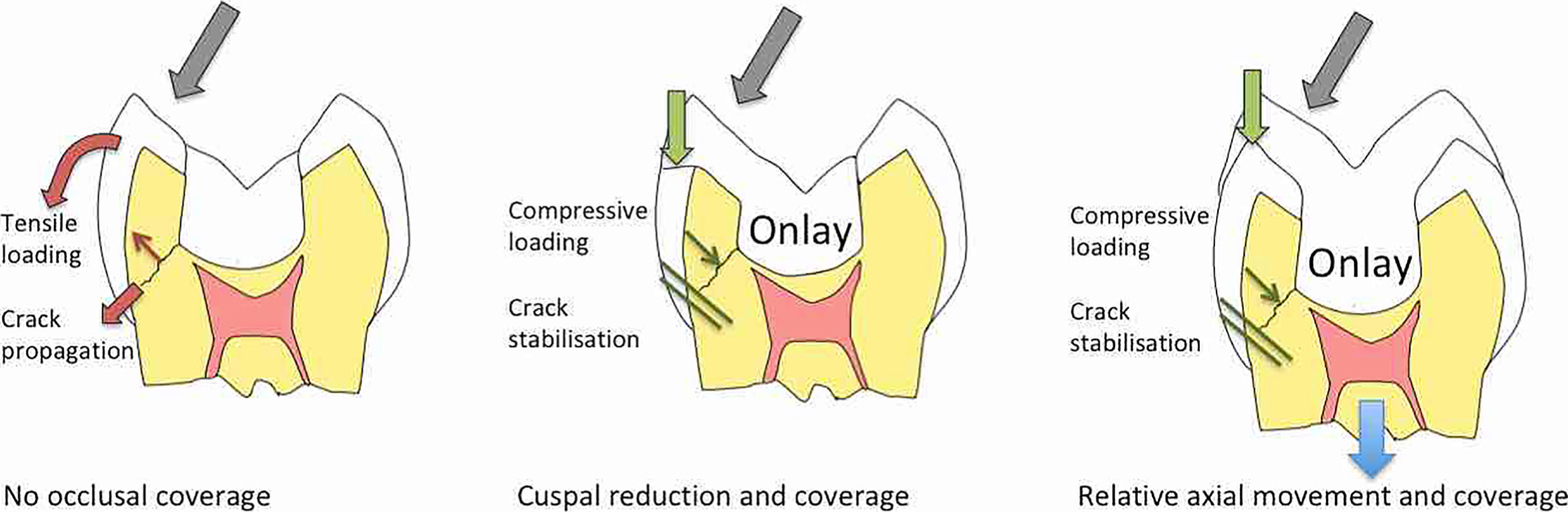
Figure 2. (a) Pain on biting LR6. Disto-buccal cusp reproducible pain on biting using Tooth Slooth. Thin remaining cusps likely to be unsupported, or minimally supported, by dentine at the tips, and broad, deep loss of mesial marginal ridge. Tooth heavily restored and therefore deemed to benefit from reduction to provide full occlusal coverage, even if not undermined by a crack. DCS bonding therefore inappropriate. (b) Same tooth as in (a). Disto-buccal portion fell away on removal of restoration, but multiple cracks noted with central vertical crack. This is an indication for full occlusal coverage, even if cusps had not previously been deemed to benefit from reduction prior to restoration removal. Cusps reduced 1.5–2 mm. (c) Full occlusal coverage composite. Patient informed of guarded prognosis. Pain resolved at recall and responsive to Endo-Frost (Roeko, Langenau, Germany) within normal limits.Figure 3. (a) Oblique crack undermining mesiobuccal cusp of UL7. Cusp initially lowered to provide occlusal coverage. (b) Same tooth as in (a). Crack noted in overlying enamel (exit point of crack apparent). Complete removal not deemed to compromise the pulp or restorability of the tooth. (c) Complete removal of the crack. Palatal cusps thick and well supported by dentine, therefore deemed not to benefit from cuspal coverage and not reduced. Tooth has a favourable prognosis.Figure 4. (a) Pain on biting UR6. Mesio-palatal cusp reproducible pain on biting and release of pressure using Tooth Slooth. Cusps likely supported by dentine and would not obviously benefit from occlusal coverage in the absence of a crack or cracks. Tooth minimally restored therefore suitable to consider bonding a DCS, however, patient has implant-retained restorations and therefore reduced eruptive potential. DCS bonding to gain inter-occlusal space therefore deemed inappropriate (Table 1). (b) Symptomatic oblique crack undermining mesio-palatal cusp of UR6. No exit point evident in overlying enamel. Cusp reduction required; crack removal not to be attempted. (c) Same tooth as (b). Asymptomatic oblique dentine cracks also undermining buccal cusps. No obvious exit points of cracks in overlying enamel. Cuspal coverage indicated, therefore buccal cusps also reduced. Disto-palatal cusp supported by dentine and marginal ridge intact, with no indication for reduction, however, reviewing the photos shows coverage may have been beneficial. Occlusal reduction of affected cusps by 1.5–2 mm before particle abrasion with 27 micron aluminium oxide powder in preparation for bonding. (d) Direct composite restoration with partial occlusal coverage. (e) Complete resolution of symptoms at 6-month recall, response to Endo-Frost within normal limits. Occlusal adjustment following (d) to preferentially load restoration over remaining cusp in attempt to reduce tooth fracture risk. Guarded long-term prognosis due to unknown parameters of remaining cracks, including direction and depth.Figure 5. Options for provision of cuspal coverage, and simplified representation of change in nature of loading of a cracked tooth when subject to occlusal forces.Figure 6. (a) Pain on biting from LR6. Reproducible pain on release of biting force using Tooth Slooth. Minimal occlusal composite placed 5 years previously. All remaining cusps are likely supported by dentine and marginal ridges intact. No cusps deemed to benefit from cuspal coverage, if not undermined by a crack. Tooth minimally restored, therefore cusp reduction to be avoided, if possible. (b) Peri-apical radiograph of LR6 shows no obvious apical pathology, a distal enamel lucency apparently confined to enamel and a shallow occlusal restoration. (c) Trial DCS placed on LR6 in composite to assess pain resolution. DCS is around 1.5 mm thick and wraps buccal and lingual cusps. Patient asked to close, explaining that the bite will feel high. Pain completely resolved. The DCS is not bonded to the tooth at this stage. (d) DCS removed and patient consented to treatment. See Table 1 for patients in whom to avoid DCS bonding and Table 2 for advice on information to discuss with patient. (e) DCS cemented in supra-occlusion. Flat surface to avoid deflective contacts. (f) Only first molars in contact. (g) Five-month review. Patient reports that pain resolved immediately. Difficulty eating for around two weeks, but no problems after that. (h) All teeth back in contact. LR6 responding within normal limits to Endo-Frost. (i) DCS and restoration removed. No occlusal reduction required. Particle abrasion 27 micron aluminium oxide in preparation for definitive restoration. Direct composite restoration selected to allow ease of access to, and subsequent restoration of, distal surface should the carious lesion progress and require operative intervention. (j) Cracks evident lingually, LR6. (k) Direct composite onlay placed LR6 and occlusion checked.Figure 6. (l) Asymptomatic LR6 at 6 month recall, responding within normal limits to Endo-Frost.Figure 7. (a) Initial presentation, reproducible pain on biting pressure LR6 MB cusp using Tooth Slooth. All remaining buccal cusps appear thin, likely unsupported or minimally supported by dentine towards the tips, therefore classified as heavily restored. Lingual cusps difficult to assess fracture risk, borderline thickness, likely minimal dentine support, thin marginal ridges likely unsupported by dentine and multiple enamel cracks present. Erring on side of caution, all cusps deemed to benefit from coverage, even if not undermined by a crack. Reduction deemed appropriate. DCS bonding to gain inter-occlusal space not appropriate. (b) Depth cuts made for 1.5 mm occlusal reduction. (c) Gross initial restoration removal and occlusal reduction performed. (d) Final cavity preparation following particle abrasion 27 micron aluminium oxide. (e) Peripheral walls built in conventional paste composite. Base filled with flowable bulk-fill composite. (f) Cusps restored with conventional paste composite. (g) Immediate post-op. (h) Two-week recall, complete resolution of symptoms, response to Endo-Frost within normal limits
When treating CTS, an unrestored, or minimally restored, tooth can be managed differently from a more heavily restored tooth by using a bonded DCS. This is not recommended in certain patient groups, however (Table 1) (see later).
2. Retention versus removal of cracks
Cracks always have the potential to propagate, and cracks that communicate with the oral environment usually harbour biofilm,16 which could cause periodontal and pulpal pathology. It may therefore seem logical to remove cracks from teeth by cutting them out, yet this is rarely helpful, especially when a crack is vertically oriented (Figure 2b), or when a tooth is unrestored or minimally restored (Figure 6a). Cracked dentine does have an ability to self-limit crack propagation, and the complex dynamics of the host response to biofilm in the manifestation of pulpal and periodontal health or disease are not well understood.
Cracks can run sub-gingivally and centrally, with no reversible means of assessing the point of termination (Figure 2b). It is impossible to know if a crack has been completely removed when there is no external termination point, as the crack tip and micro-cracks will not be visible with clinically obtainable magnification.17 Attempts to remove cracks result in unnecessary tissue loss in areas critical to prognosis of the tooth, notably in proximity to the pulp, and in the peri-cervical region, which is biomechanically important.18 This also potentially places the restorative margin in dentine rather than enamel, where the adhesive bond will subsequently degrade more rapidly over time.19,20
Vertical cracks: Vertical cracks without caries should therefore never be ‘explored’. It is advised that full occlusal coverage (this does not mean a crown) should be provided for teeth with vertical cracks (Figures 2 b and c), acknowledging that such teeth have a guarded prognosis.
Oblique cracks: Oblique cracks associated with restorations can be managed differently from vertical cracks. If a crack in dentine is visible in the overlying enamel, it is advised that removal be attempted, provided this will not compromise the pulp, or the restorability of the tooth (Figures 3 a–c). This is based on clinical experience of seeing (very) occasional issues of recurrence of CTS at follow-up when retaining such cracks. Where complete removal of the crack is deemed appropriate and subsequently performed, the tooth has a favourable prognosis (Figure 3c).
If removal would compromise the pulp or restorability of the tooth, or if the dentine crack cannot be seen on the external tooth surface, the crack should not be ‘explored’ or removed. Instead, the affected cusp should be overlaid (Figures 4 b–d). In this situation, the prognosis is more favourable than a vertical crack, but still guarded in the longer term, as the crack has unknown parameters, including depth and direction (Figure 4e).
3. Provision of cuspal coverage
Occlusal coverage makes the tooth less susceptible to fracture by stabilizing the crack and changing the loading of the affected cusp(s) by converting damaging, primarily tensile stress into supportive compressive stress21 (Figure 5).
Space is required to provide occlusal coverage of the affected cusp or cusps. This can be gained through relative axial movement (tooth intrusion and extrusion), following the application of a DCS, or through cuspal reduction. Both are useful in different situations (Figure 5).
Unrestored or minimally restored teeth
Unrestored or minimally restored teeth are excellent candidates for relative axial movement to provide space for occlusal coverage, as this means no tooth reduction is required (Figures 6 a–h). This maximizes retention of enamel, which is more predictable to bond to than dentine in the long term.19
Heavily restored teeth
In heavily restored teeth, thin cusps flex more, suffering tensile stress in function which puts them at increased risk of fracture.15,21 Though it may seem sensible to retain these cusps and gain space to cover them by relative axial movement, it is suggested that this is misguided.
When a tooth is heavily restored and unsupported enamel is present at remaining cusps tips (Figures 7 a and b) (whether crack affected or not, but especially in crack-affected cusps), leaving them unmodified, compared to reducing them, will increase flexure during definitive adhesive restoration. This is due to the less favourable cavity C-factor, and resultant increased development of interfacial contraction stress, which is unfavourable in an already cracked tooth.22,23
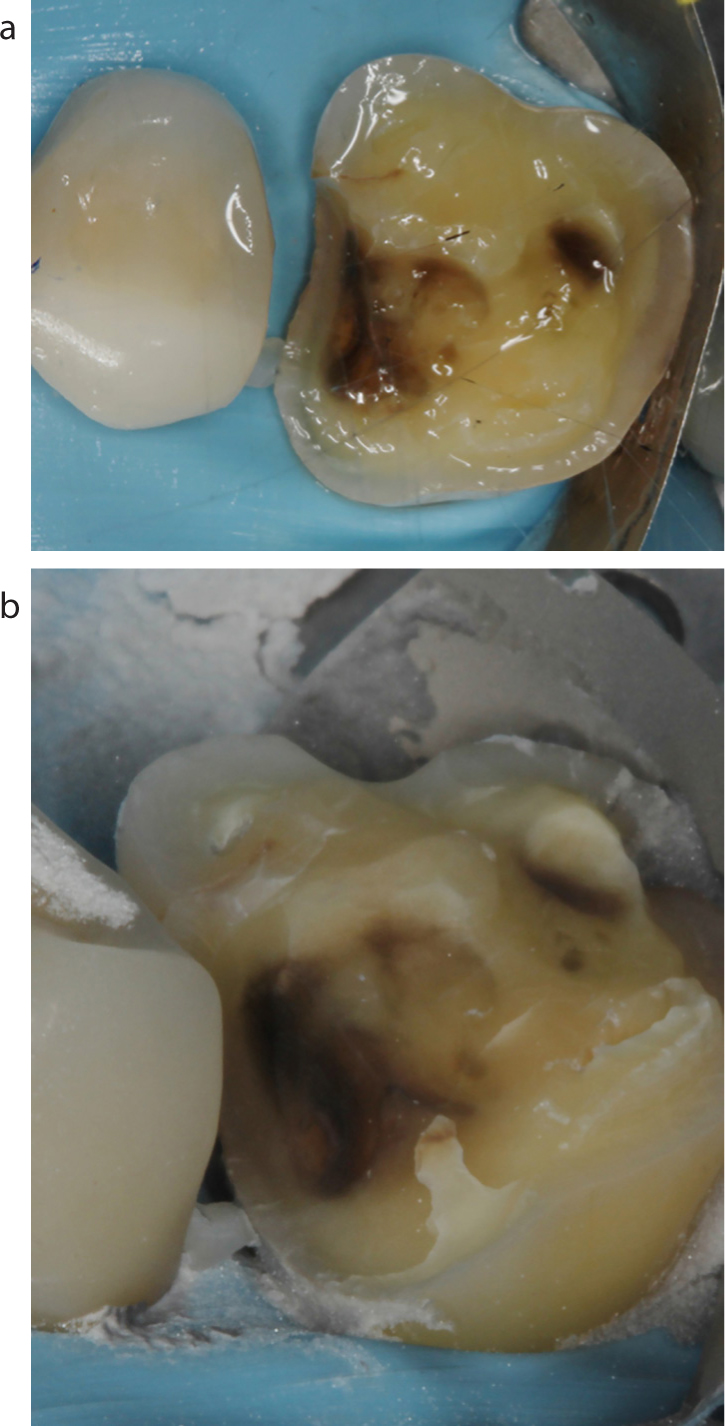
Thin cracked cusps quite commonly fall away during the removal of an existing restoration (Figure 8a), and retaining thin cusps where the crack in dentine is visible in the overlying enamel can be problematic, as described above. It is therefore often favourable to remove them, even if they remain. This would then lead to an increased height of restorative material being required to restore the tooth, if space has already been gained by relative axial movement. This is biomechanically unfavourable, resulting in increased relative cyclical fatigue at the restorative margin. Should the thin cusp be retained, there would be increased load transference to an internally initiated crack which, allied with the damaging contraction stress, could potentially lead to more rapid failure.24
Figure 8. (a) UR6 enamel fragment evident interproximally as cracked portions fell away during restoration removal. (b) UR6 crack remnant remained mesio-buccally which was obvious following particle abrasion with 27 micron aluminium oxide. It was not recognized prior to particle abrasion.
It is therefore recommended that there is no benefit in gaining inter-occlusal space by relative axial movement in more heavily restored teeth, where it has been assessed that any cusp(s) would benefit from coverage, even if a fracture was not present. In these situations, it would be better to obtain inter-occlusal space by cuspal reduction (Figures 2a, 7a and b) or removal (Figures 3 a–c), as dictated by the presence of the dentine crack in the overlying enamel as previously discussed.
Cuspal reduction also offers advantages over bonding a DCS in that it reduces patient chair-time, treatment duration, and therefore cost, while avoiding risks of occlusal contacts failing to re-establish, among others (see later). Bonding a DCS should therefore be avoided in heavily restored teeth diagnosed with CTS (Figures 2a and 7a) (Table 1 green text).
Further DCS considerations
Another important situation in which bonding a DCS should be avoided is in patients with a large horizontal slide from their retruded contact position (RCP) to the intercuspal position. This is because it is quite possible that a DCS could act to ‘deprogramme’ the muscles of mastication by taking their initial RCP guiding contact away, which in turn would allow the condyles to seat, putting the patient at risk of developing a large overjet and/or anterior open bite25 (Table 1 green text). Banerji et al9 also advise that there are a number of situations where bonding a DCS should be avoided. These seem sensible and are listed in Table 1 (blue text). Banerji et al9 also reported that bonding a DCS resulted in a number of other patient complaints. Table 2 summarizes these with a suggestion of information to discuss with a patient as part of the consent process prior to bonding a DCS.
Likely to feel strange for 2 weeks, difficult to chew, commonly settles after that
Small risk of intolerance to open bite
Small chance exacerbation of pain
Small chance DCS will break
Slight chance of increased tooth mobility
Slight chance teeth won't come back together
Slight chance jaw joint and muscle tenderness
To contact in case of concern
Banerji et al also suggest that the tooth with bonded DCS should immediately disclude on the canine.9,26 If the DCS is bonded at the recommended 1.5 mm thickness in the posterior,26 this roughly equates to an opening in vertical dimension of 3–4 mm at the canine. This opening would likely necessitate composites being placed on both canines to achieve immediate disclusion of the DCS-protected tooth in all cases. This was only performed in 12.6% of cases, however. The author suggests that this is unnecessary. Immediate disclusion on the canines was not established in the case shown (Figure 6f), but the DCS was made as a flat surface with no deflective incline contacts (Figure 6e). This did not compromise the outcome for the patient (Figure 6m).
Cuspal reduction – which non-CTS affected cusps, and how much?
Defining which cusps are at risk of fracture is difficult and involves consideration of multiple factors, as previously discussed. Figures 2a, 3c, 4a and c, 6a and b and 7a show examples of where cusps, that were not undermined by a painful crack, were considered to be at increased risk of fracture, where they were not, and where other factors were important. This determined whether or not cusps were subsequently reduced. Whilst decision-making is very subjective, if in doubt, it may be better to reduce the cusp (Figure 7a), as this is a non-critical area of the tooth, as opposed to the peri-cervical region, which is more important from the perspective of reduced future fracture risk and prolonged lifespan of the tooth.27,28,29 Preferentially loading the restoration, by eliminating contacts in static and dynamic occlusion on retained cusps, may also be beneficial, aiming to move the eventual failure mode from the tooth to the restoration (Figure 4e).
The appropriate degree of reduction for coverage by direct composite has not been determined, as it is likely to be dependent on a number of variables considered previously. For example, if inter-occlusal space to overlay cusps in an unrestored tooth is created using a DCS, support for the restoration provided by a surface solely of enamel is likely to be much better than a previously heavily restored tooth, with a large, irregular volume of structure to replace and a preponderance of dentine to bond to.15 An in vitro study using a premolar model with a mesio-occluso-distal (MOD) preparation and missing cusp, compared restoration in composite with or without 1.5 mm reduction of the existing cusp. Overlaying the reduced cusp resulted in a much improved fracture resistance, but the mode of failure was slightly less favourable.30 In another laboratory study, direct composite onlay restoration following 2.5 mm cuspal reduction, showed a more favourable stress distribution than 1.5 mm reduction in premolar MOD cavity models.21 How cracks would modify these findings is unknown. Striking the optimal balance between modifying force distribution and maintaining tooth structure inevitably carries uncertainty, which makes translation to the clinical environment difficult. General advice would be to consider 1.5–2 mm of reduction (Figures 2b, 4c and 7 b–d).
If the remaining cusp is subsequently unsupported by dentine following reduction, consideration should be given to further reduction until it is supported. However, if this removal compromises the restorability of the tooth, it should not be performed.
Preparation optimization
Cavity preparation results in reduced fatigue resistance of dentine, and particle abrasion cut dentine fares better than bur cut dentine in this respect.31 Deeper dentine is more brittle, compounding the effect of structural compromise in deeper cavities.32 Finalizing cavity preparation with particle abrasion may therefore be beneficial to the compromised dentine, whilst also aiding bonding.33 Particle abrasion can also help to visualize retained crack remnants, facilitating complete removal, as even when a cracked portion of tooth splinters away during operative exploration, the crack is not always completely removed (Figures 8 a and b).
Restorative implications and choices
Resin-bonded restorations result in contraction stress at the interface with the cavity, as previously discussed.34 It is unclear how this might affect a dentine crack in terms of propagation, but it has been shown in vitro, that teeth with an occlusal cavity that are restored with various composite materials and techniques (bulk-fill composites topped with a conventional composite versus a layered approach with conventional composite) developed cracks in the overlying enamel where none existed beforehand, whilst also resulting in extension of pre-existing cracks.34 Bulk-fill composites developed less contraction stress at the restorative interface than a layered approach, but all tested materials varied. The teeth restored with bulk-fill composites all showed increased fracture resistance compared to those restored with a conventional layered composite.34 It is as yet unclear, however, how a more compromised tooth may behave over time, when restored with some of the flowable bulk-fill materials which have a reduced modulus of elasticity (rigidity),35 though more rigid, paste-like bulk-fill composites are available.36
The rigidity of direct composite is also lower than indirect composite, metal or ceramic, and some commentators would suggest that a more rigid material, mechanically or adhesively retained, is appropriate to prevent crack propagation.37 One study, however, showed comparable fatigue resistance of cusp replacement restorations of ceramic, direct and indirect composite in premolars.38 They might also justifiably consider that the interfacial contraction stress is reduced when placing indirect restorations,39 which may reduce the tendency to propagate a fracture. Conversely, it has been suggested that internal development of stress could contribute to the fracture resistance of cusp-replacing restorations,40 though the stress does reduce over time, primarily through hygroscopic expansion.41
Currently, there is no compelling clinical evidence to support the importance of these contentions, so direct composite can be recommended, based on all clinically relevant outcome parameters discussed, alongside the reduced clinical time required, the absence of need for a non-bonded temporary and the consequent economic benefit. However, that is not to say that bonded indirect onlay restorations are inappropriate, especially for a tooth with a stabilized crack.
Restorative procedure
Optimization of the bonding procedure is advisable, so a suggested protocol involves use of rubber dam,42 particle abrasion of the preparation,33 use of a three-step bonding system (4th generation bonding agent or 5th generation bonding agent with selective enamel etch procedure) to optimize bonding,43,44,45,46,47 which helps to resist bond breakdown long-term, especially with dentine margins,19,43 and use of a bulk-fill composite material in combination with a conventional composite34 (Figures 7 d–h).
Immediate management
Even if DCS bonding is not going to be used to gain inter-occlusal space, it can be performed as an immediate short-term temporary measure in an attempt to prevent propagation of a crack (for example whilst the patient awaits an appointment for definitive restoration). Alternative immediate management strategies include cementation of a copper ring or orthodontic band,26 to minimize separation of any cracks, or lowering of cusps and reduction of cuspal inclines to minimize lateral loading,48 again while the patient awaits an appointment for definitive restoration.
Conclusions
Evidence on the management of CTS is very limited. Direct and indirect bonded composite restorations overlaying affected cusps show good survival, success in resolving symptoms, and maintaining pulp vitality in CTS-affected teeth in the medium term.
While it is clear that a DCS is an excellent tool for diagnosing CTS, and bonding a DCS can be very successful, in many situations it is not appropriate (Table 1). It may unnecessarily complicate and prolong treatment for patients with heavily restored affected teeth and expose them to risks that they need not face. Each case should be assessed on its merits and managed appropriately, with input from the patient.
Crowning CTS-affected teeth leads to significant need for pulpectomy in the short term and should be avoided where possible.
Decision-making will always involve numerous variables, and sometimes the cost of sacrificing non-critical tissue with dubious structural integrity is a worthwhile price to pay for improved clinical predictability and patient-centred outcomes. Given that the orientation of a crack in restored teeth is generally unknown prior to restoration removal, the patient should be informed of the guarded prognosis prior to any operative intervention. The potential for persistent thermal sensitivity should also be discussed.