Morse J, Bonsor SJ. Two Eyes, Two Fingers, Two Minutes: Making it Easier to Recognize and Manage Medical Emergencies in Dental Practice Part 1: The Modified Dental Early Warning Score (M-DEWS2). Dent Update. 2020; 47:360-373
Why asthma still kills: The national review of asthma deaths (NRAD) confidential enquiry report.London: RCP; 2014
O'Driscoll BR, Howard LS, Earis J, Mak V. British Thoracic Society Guideline for Oxygen use in Adults in Healthcare and Emergency Settings. BMJ Open Respir Res. 2017; 4 https://doi.org/10.1136/bmjresp-2016-000170
Nikolaou NI, Arntz HR, Bellou A European Resuscitation Council Guidelines for Resuscitation 2015 section 8. Initial Management of Acute Coronary Syndromes. Resuscitation. 2015; 95:264-277 https://doi.org/10.1016/j.resuscitation.2015.07.030
O'Driscoll BR, Howard LS, Earis J, Mak V. British Thoracic Society Emergency Oxygen Guideline Group, BTS Emergency Oxygen Guideline Development Group. BTS guideline for oxygen use in adults in healthcare and emergency settings. Thorax. 2017; 72:ii1-ii90 https://doi.org/10.1136/thoraxjnl-2016-209729
Truhlář A, Deakin CD, Soar J European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. 2015;
Two Eyes, Two Fingers, Two Minutes: Making It Easier to Recognize and Manage Medical Emergencies in Dental Practice Part 2: Algorithms to Guide Treatment using the M-DEWS2 Tool
Two Eyes, Two Fingers, Two Minutes: Making It Easier to Recognize and Manage Medical Emergencies in Dental Practice Part 2: Algorithms to Guide Treatment using the M-DEWS2 Tool Jerry Morse Stephen J. Bonsor Dental Update 2024 47:5, 707-709.
Authors
JerryMorse
ProfD, FAcadMEd
Manager of Clinical Skills and Lead for Simulation, Institute of Education for Medical and Dental Sciences, University of Aberdeen
BDS(Hons), MSc, FHEA, FDS RCPS(Glasg), MDTFEd, GDP
The Dental Practice, 21 Rubislaw Terrace, Aberdeen; Hon Senior Clinical Lecturer, Institute of Dentistry, University of Aberdeen; Online Tutor/Clinical Lecturer, University of Edinburgh, Edinburgh, UK
In the second of two papers on the recognition and management of potential medical emergencies that may occur in the dental clinic setting, the development of new algorithms to assist in making it easier for members of the dental team to recognize and treat such situations will be discussed. Used in conjunction with the M-DEWS2 scoring sheet as discussed in the first paper, these algorithms cover the eight common medical emergencies that may occur in dental practice.
CPD/Clinical Relevance: All members of the dental team require the appropriate skills and knowledge to manage medical emergencies should they occur.
Article
Jerry Morse
A medical emergency may occur in any dental clinic at any time whether the patient has received treatment or not. The first paper in this series of two described the M-DEWS2 assessment tool to aid the early management of the medically deteriorating patient and to facilitate his/her subsequent acute management.1 The eight common medical emergencies which may be seen in the dental care setting are asthma, angina, acute myocardial infarction (heart attack in layman's terms), vasovagal syncope, hypoglycaemia, anaphylaxis, cerebrovascular accident (‘stroke/brain attack’) and seizures. This present paper describes algorithms which may be used to manage and treat these common medical emergencies in conjunction with the M-DEWS2 tool. The diagnosis and management of these conditions are now discussed.
Asthma
In the UK, over 8 million people, or approximately 12% of the population, have been diagnosed with asthma with approximately 160,000 people being newly diagnosed each year.2 Asthma is a chronic respiratory condition associated with airway inflammation and hyper-responsiveness. An acute exacerbation may be triggered by such things as exposure to an environmental stimulant (such as cold air, warm or moist air, exercise or exertion, or emotional stress) or allergen (for example, air-freshener or pollen). The bronchi swell and narrow the airways, creating breathing difficulties that may range from mild to life-threatening. This makes breathing for the patient very difficult, especially when breathing out, and can be extremely frightening in a severe episode. The disease is heterogeneous, with different underlying disease processes and variations in severity, clinical course, and response to treatment.
Asthma attacks can be greatly underestimated by both patients and healthcare professionals, with three people dying each day in the UK from severe attacks.3 Furthermore, a report by the Royal College of Physicians suggested that 45% of those who died from asthma did not realize its severity or seek assistance.4 Therefore, members of the dental team should be equipped to assist if required. It is equally possible that both adults and children may suffer an asthma attack whilst in the dental surgery. The clinical features of acute severe asthma in adults are listed in Table 1. However, if an acute asthma episode is untreated, then the patient may quickly deteriorate into a life-threatening condition. Clinical features of life-threatening asthma in adults include:
Cyanosis and a decreased respiratory rate of less than 8 breaths per minute;
Bradycardia (heart rate less than 50 beats per minute);
Exhaustion, confusion and a decreased level of consciousness.
▪ An inability to complete sentences in one breath. To assess this quickly, patients should be asked to count from 1 to 10 to ascertain how many numbers they can complete in one breath;
▪ Possible audible wheeze (audible sound on exhalation);
▪ Tachypnoea (an increased respiratory rate of more than 22 breaths per minute);
▪ Tachycardia (heart rate of more than 100 beats per minute).
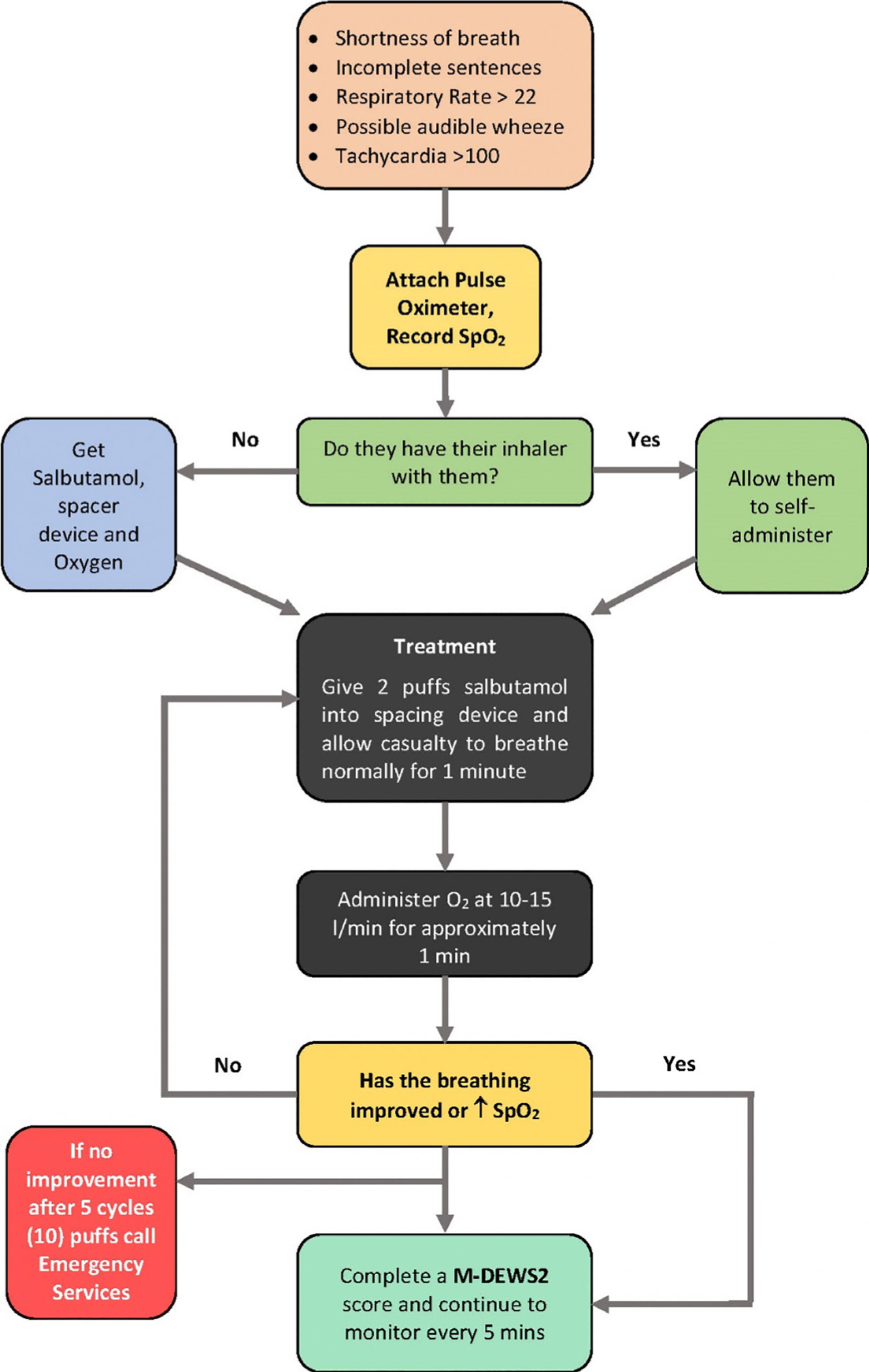
An algorithm which may be used if a patient is suspected of suffering from asthma is shown in Figure 1.
Figure 1. An algorithm which may be used if a patient is suspected of suffering from asthma.
The treatment of acute asthma is set out below:
If it is known that the patient suffers from asthma then they may have their inhaler with them. It is important to be aware that many asthmatic patients do not routinely carry their inhalers. It is wise therefore to check prior to commencing treatment that any necessary inhaler is to hand. The patient should be placed in a comfortable position which is usually sitting upright and slightly forward.
A pulse oximeter should be attached to the patient to obtain a baseline observation and this recorded on the M-DEWS2 sheet.
A salbutamol inhaler should be used in conjunction with a spacing device. Two puffs of salbutamol should be expressed into the spacing device and the patient allowed to breathe as normally as possible for approximately 1 minute.
Oxygen should then be administered at 15 l/min for approximately 1 minute in a non-rebreather mask.
The patient should then be reassessed. If there is no improvement in their breathing or the oxygen saturation level (SpO2) remains the same or is decreased, then an additional 2 puffs of salbutamol in conjunction with oxygen should be administered as described in 3 above.
If there is no improvement after 5 of these cycles (ie 10 puffs of salbutamol in total), then the emergency services should be called as more definitive help may be required. As asthma is a potentially life-threatening condition, if there is any doubt or concern about the patient, it is prudent to call for help sooner rather than later.
Angina
Angina is caused by an insufficient blood supply to the myocardium, usually as a result of atherosclerotic plaques forming on the internal walls of the coronary arteries leading to a progressive narrowing of the lumen. Symptoms of angina occur when the blood flow does not provide adequate amounts of oxygen to the myocardium at times when oxygen demand increases, for example, during exercise. Pain (or constricting discomfort) in the chest, in the neck, shoulders, jaw, or arms is experienced by the patient, but this pain is transient and is normally reduced or relieved by rest and/or the patient's prescribed medication. There are two main types of angina: stable angina and unstable angina.
Stable angina
In patients with stable angina the symptoms usually develop gradually over time and follow a set pattern. For example, patients may only experience symptoms when climbing stairs or if they are under a lot of stress. The symptoms of stable angina usually only last for a few minutes and can be improved by resting and/or taking medication, such as glycerine trinitrate (GTN) which is presented in spray or tablet form and administered sub-lingually. Although stable angina may not be life threatening on its own, it is a sign that the coronally arteries are compromised with an increased risk of myocardial infarction (MI).
Unstable angina
While patients with a history of stable angina may develop and experience symptoms of unstable angina, it is possible that unstable angina may also present in people who have previously been symptomatic. For those patients known to have unstable angina, symptoms can develop rapidly and can persist, even when the patient is at rest. The symptoms may continue for some time and, in some cases, do not respond to treatment with GTN. Unstable angina should be regarded as a medical emergency as it is a sign that the blood supply to the myocardium (heart muscle) is being compromised, so decreasing the ability of the heart to function and increasing the risk of MI. Table 2 sets out the clinical features of angina in adults. The treatment for angina is as follows:
The patient should be placed in a position which they find comfortable (this is usually sitting up) and reassured;
If the patient normally takes medication for angina, such as GTN, then they should self-administer;
The patient should be allowed to rest and the symptoms should settle within 10 to 15 minutes or quicker in response to the GTN;
Although GTN can be repeated after 5 to 10 minutes if required, this could indicate that the angina is worsening or potentially developing into an acute MI. The emergency services should be called and an M-DEWS2 score completed, as described in the previous paper.1
▪ A gripping chest pain often spreading to the left side of the jaw or left arm. This is sometimes accompanied by pain or tingling in the hand. The pain is often brought on by exercise and/or exertion but is relieved with rest and/or medication;
▪ Shortness of breath (SOB);
▪ A weakness that is often sudden or extreme.
Myocardial infarction
An acute myocardial infarction is a serious medical emergency in which the supply of blood to the myocardium is suddenly greatly reduced. Any lack of blood to the myocardium can cause serious damage and may be life-threatening. The severity of the damage to the myocardium is usually determined by which of the coronary arteries has been affected. The clinical features of acute MI can be seen in Table 3. It is important to stress that not every patient having a myocardial infarction experiences severe chest pain as the pain can often be mild and mistaken for indigestion. It is the combination of symptoms that is important in determining whether a person is having a MI and not the severity of chest pain.
▪ Classically a central crushing chest pain which feels like the chest is being pressed or squeezed by a heavy object. The pain can radiate from the chest to the mandible, neck, arms and back;
▪ Shortness of breath (SOB);
▪ Pale or ashen face often with diaphoresis (cold sweats) and the patient feels clammy to the touch;
▪ Feeling weak and/or light-headed;
▪ Nausea and/or indigestion;
▪ Overwhelming feeling of anxiety;
▪ The feeling of needing to defecate.
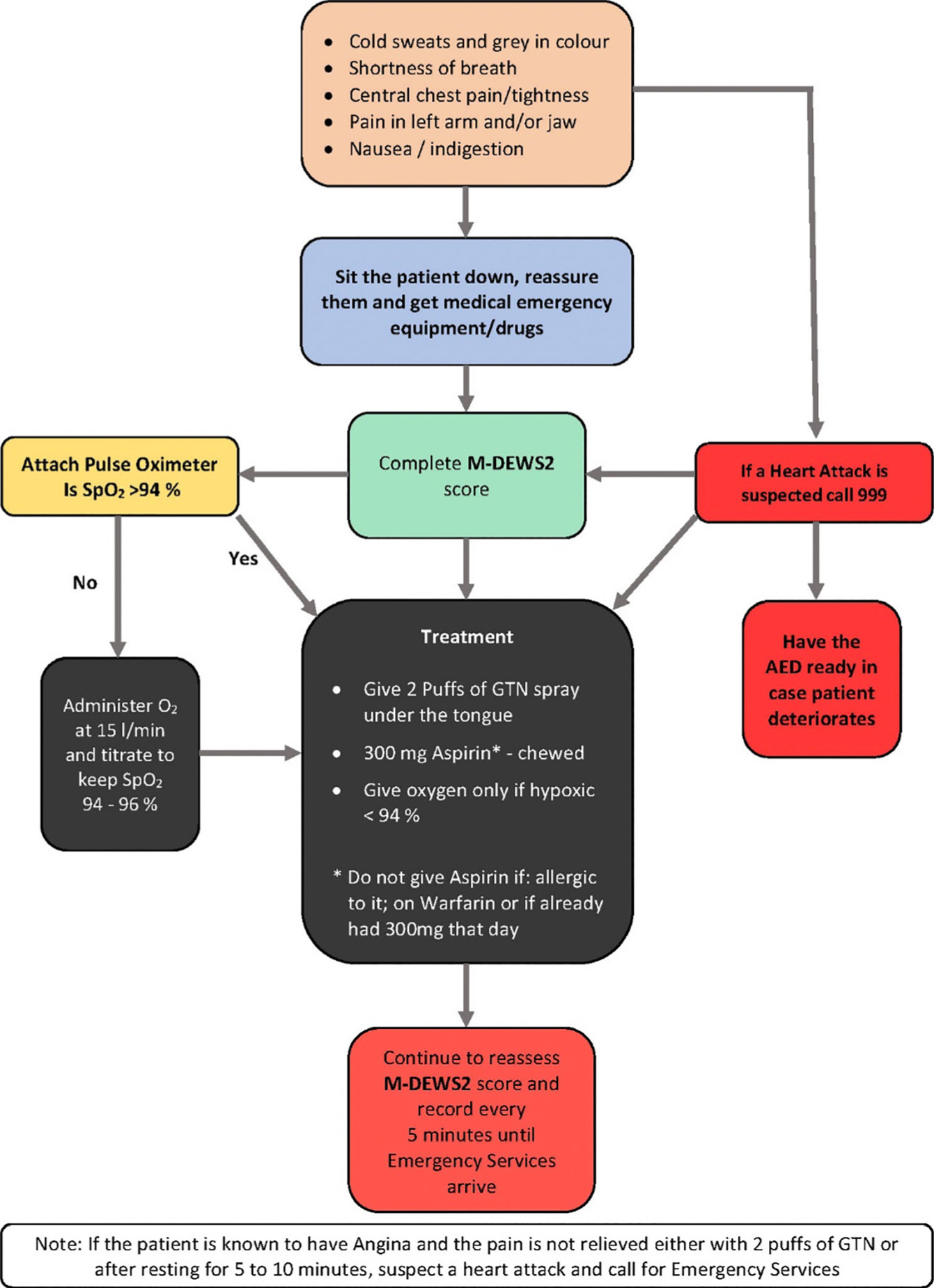
The treatment algorithm for acute myocardial infarction is shown in Figure 2 and described below:
If a MI is suspected, the escalation protocol should immediately be used and the emergency services called by dialling 999 in the UK, 112 in the European Union or 911 in the USA.
Patients should be made comfortable in whatever position they find best, which is usually sitting up.
Patients should be reassured and an M-DEWS2 score completed and documented.
If patients have their own GTN spray, then they should administer 2 puffs under the tongue. Should patients not have their GTN to hand, it should be retrieved from the medical emergency drugs box and given to patients to self-administer. A further dose of GTN can be repeated after 5–10 minutes.
Aspirin 300 mg may be given at this point in crushed or chewed form. However, it should not be given if the patient has a hypersensitivity to it; is on warfarin or other anticoagulants; or has already had 300 mg of aspirin that day. It is important to inform the paramedics and/or other medical colleagues if aspirin has been given.
Recent research has shown that the use of high concentration oxygen may actually increase the size of the infarct and is therefore detrimental to patients with an uncomplicated myocardial infarction.5,6,7 As most patients with acute coronary syndromes are not hypoxaemic, oxygen should only be given if the patient's SpO2 is below 94% and then titrated to maintain it above 94%.7
An Automated External Defibrillator (AED) should be readily accessible in case the patient suffers a cardiac arrest.
Figure 2. An algorithm which may be used if a patient is suspected of suffering from an acute myocardial infarction.
Vasovagal syncope
Vasovagal syncope is a temporary loss of consciousness usually related to a short-lived insufficient blood flow to the brain, commonly known as a faint, fainting spell or fainting attack. It may be caused by many different factors, including emotional stress, pooling of blood in the legs due to sudden changes in body position or heavy sweating.
In the dental setting, one of the most common reasons for patients feeling faint is hypoglycaemia, which historically arose as patients were fasted prior to dental treatment as they would be receiving a general anaesthetic to facilitate their care. These days it is most common when patients have not had anything of any note to eat prior to their attendance at the clinic, especially breakfast, when they are especially hypoglycaemic from overnight fasting. However, it should not be assumed that all faints in the dental practice are due to a low blood sugar level. Patients should therefore not be given sugar routinely before their blood glucose level has been checked. The clinical features of syncope are presented in Table 4. There may be occasions when an extreme tachycardia (over 180 beats per minute) may also cause the blood pressure to drop, leading to a decreasing level of consciousness.
▪ The patient feels faint, dizzy or light-headed;
▪ Bradycardia;
▪ Hypotension;
▪ Pallor and sweating;
▪ Nausea and vomiting;
▪ Sudden loss of consciousness.
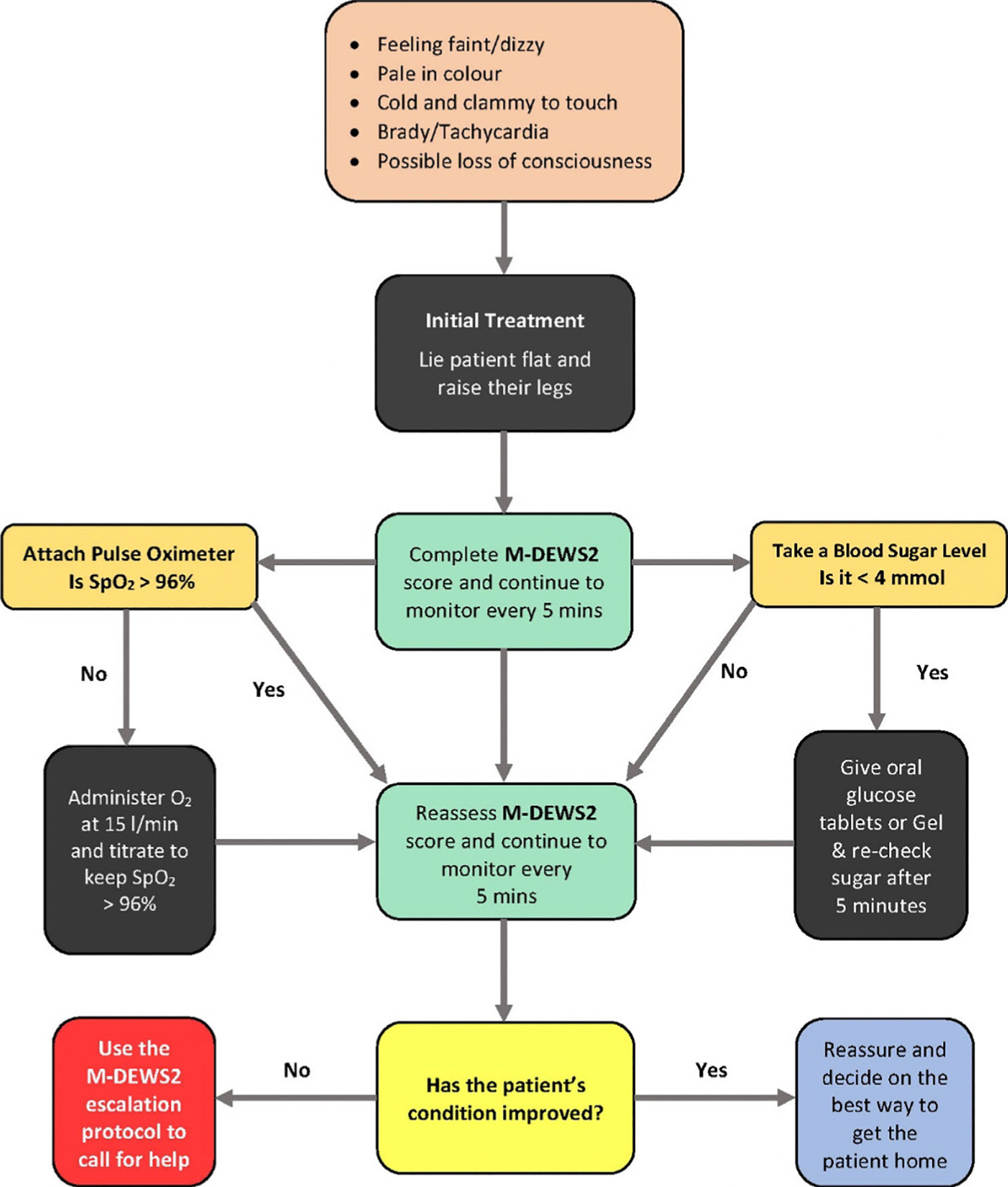
An algorithm which may be used if a patient is suspected of suffering from vasovagal syncope is shown in Figure 3 and its management is outlined below:
The patient should be laid flat as soon as possible and their legs raised to improve venous return. A pregnant woman should be rolled on her left side to relieve the pressure of the weight of the foetus pressing on the inferior vena cava impeding venous return.
Any tight clothing should be loosened, especially around the neck.
An M-DEWS2 score should be completed.
A pulse oximeter should be attached to the patient to measure the SpO2.
Oxygen should be administered at 10–15 l/min via a non-re-breather mask and titrated to maintain oxygen saturation levels at above 96%.
The blood glucose level should be checked and the hypoglycaemia protocol (Figure 4) followed if it is below 4 mmol.
After 5 minutes the patient should be reassessed and by completing a second M-DEWS2 score.
If no improvement is seen then escalation should be considered as per the protocol.1
If the condition of the patient has improved and M-DEWS2 score has decreased to normal, the patient should be reassured and appropriate measures arranged to transport them home safely.
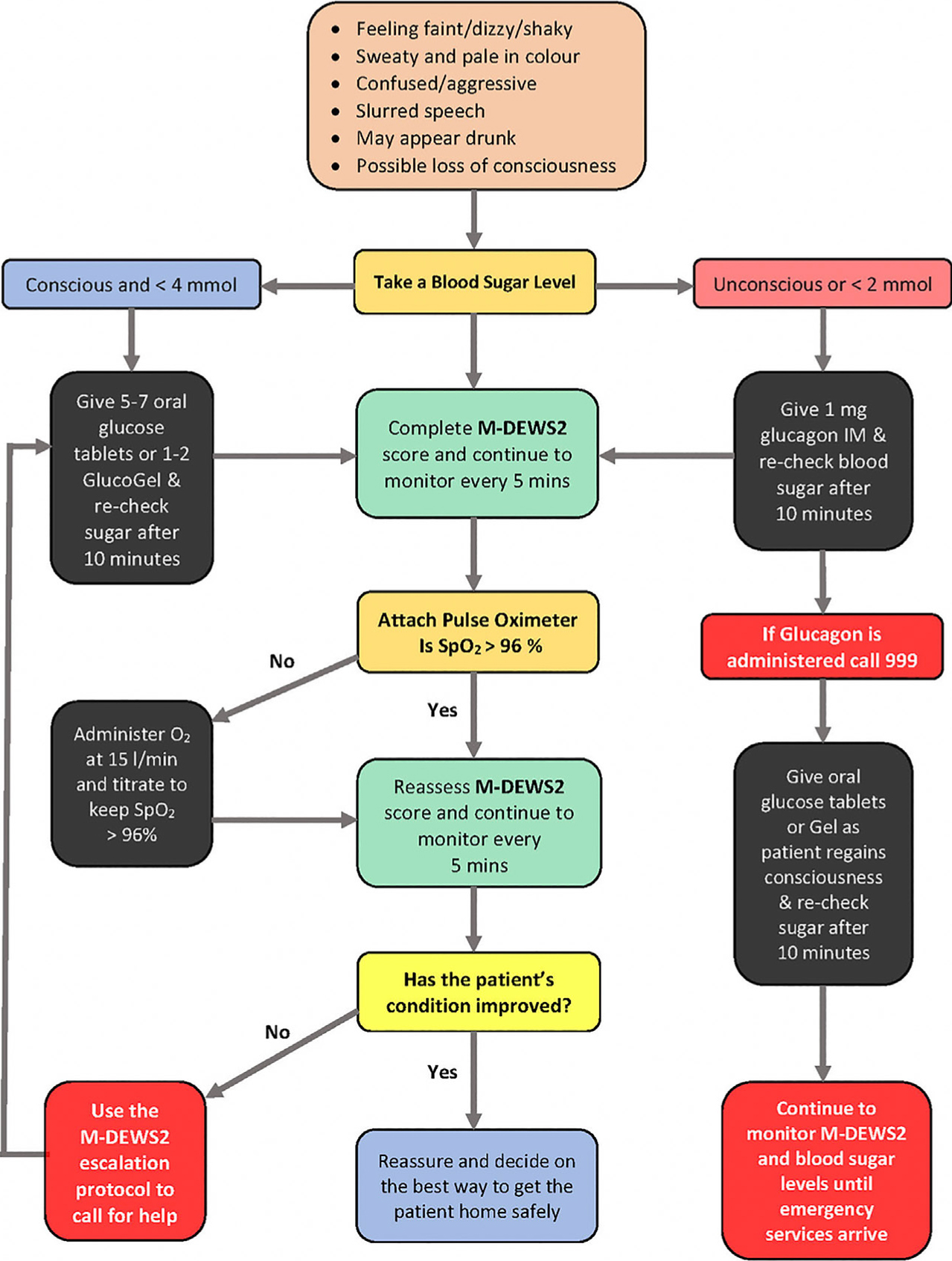
Figure 3. An algorithm which may be used if a patient is suspected of suffering from vasovagal syncope.Figure 4. An algorithm which may be used if a patient is suspected of suffering from hypoglycaemia.
Hypoglycaemia
When the blood glucose level falls below the normal ranges of 4–6 mmol, the function of the brain can become rapidly compromised. If not recognized and treated promptly the patient will deteriorate and, in extreme cases, become unconscious. It is therefore important that the signs and symptoms of hypoglycaemia are identified and treated as quickly as possible. The clinical features of hypoglycaemia are listed in Table 5.
▪ Shaking and trembling;
▪ Sweating;
▪ Headache;
▪ Difficulty in concentrating and or a vagueness;
▪ Slurring of speech;
▪ Aggression and/or confusion;
▪ Possible unconsciousness if untreated.
The management algorithm for hypoglycaemia can be seen in Figure 4.8 Treatment is set out below and should start with confirmation of the diagnosis by measuring the blood glucose level, completion and recording of an M-DEWS2 score. In the early stages or where the blood glucose level is between 2.1 and 4 mmol:
The conscious and co-operative patient with an intact gag reflex should be given oral glucose or sugar solution, glucose tablets, 4 Jelly Babies® (Maynards Bassetts, Sheffield, UK) or glucose gel.
The blood glucose test should be repeated after 10 minutes along with another M-DEWS2 score.
Further glucose can be given after 10–15 mins should no improvement be seen to the blood sugar levels.
In more severe cases, where blood glucose is below 2 mmol, the patient is likely to have an impaired conscious level and perhaps be unco-operative or be unable to swallow. In which case, intramuscular glucagon should be administered (usually into the upper arm), the doses being 1 mg for an adult and 0.5 mg for a child under 8 years of age. The blood glucose level should be rechecked after 10 minutes as per M-DEWS2 to monitor and manage further, if need be. It is important to note that, if glucagon has been administered, then emergency services should have been called, as the patient will need further assessment by medical professionals due to its short half-life. When the patient regains consciousness, further supplemental glucose should be given, together with oral carbohydrate, to restore the liver glycogen and prevent relapse of hypoglycaemia. The patient will normally respond within 10–15 minutes after the administration of intramuscular glucagon, however, glucagon will not be effective in patients whose liver glycogen is depleted. For that reason, glucagon has little or no effect when the patient has been fasting for a prolonged period, or is suffering from adrenal insufficiency, chronic hypoglycaemia or alcohol-induced hypoglycaemia.9
Anaphylaxis
An anaphylactic reaction (or anaphylaxis) is a potentially life-threatening condition in which an extreme and exaggerated allergic response to an antigen that has entered the body occurs in a previously sensitized individual. It is characterized by rapid onset affecting many body systems, such as airway and/or breathing and/or circulation problems, usually associated with skin and mucosal changes. It is due to the release of inflammatory mediators and cytokines from mast cells and basophils (such as histamine), typically due to an immunological reaction, but sometimes non-immunological mechanism. The causes of anaphylactic reactions are listed in Table 6, with the clinical features of anaphylaxis shown in Table 7. Anaphylaxis can occur at any age, at any time and its management must be immediate and aggressive, as death of the patient may occur within minutes.
▪ Drugs, eg vaccines and antimicrobials such as penicillin. Anaphylaxis due to local anaesthetic drugs is extremely rare;
▪ Foodstuffs, eg shellfish and nuts such as peanuts;
▪ Insect bites and stings, eg bees and wasps;
▪ Miscellaneous agents, eg latex gloves and hair-dyes.
▪ Urticaria;
▪ Rhinitis;
▪ Abdominal pain and vomiting;
▪ Flushing is common but the patient may remain pale in colour;
▪ Angioedema (swelling of the face and/or tongue);
▪ Complaining of difficulty in swallowing;
▪ Marked upper airway (laryngeal) oedema and bronchospasm;
▪ Audible wheeze (noise on expiration) and stridor (noise on inspiration);
▪ Vasodilation causing relative hypovolaemia, leading to hypotension and collapse;
▪ Sense of ‘impending doom’;
▪ Respiratory arrest leading to cardiac arrest.
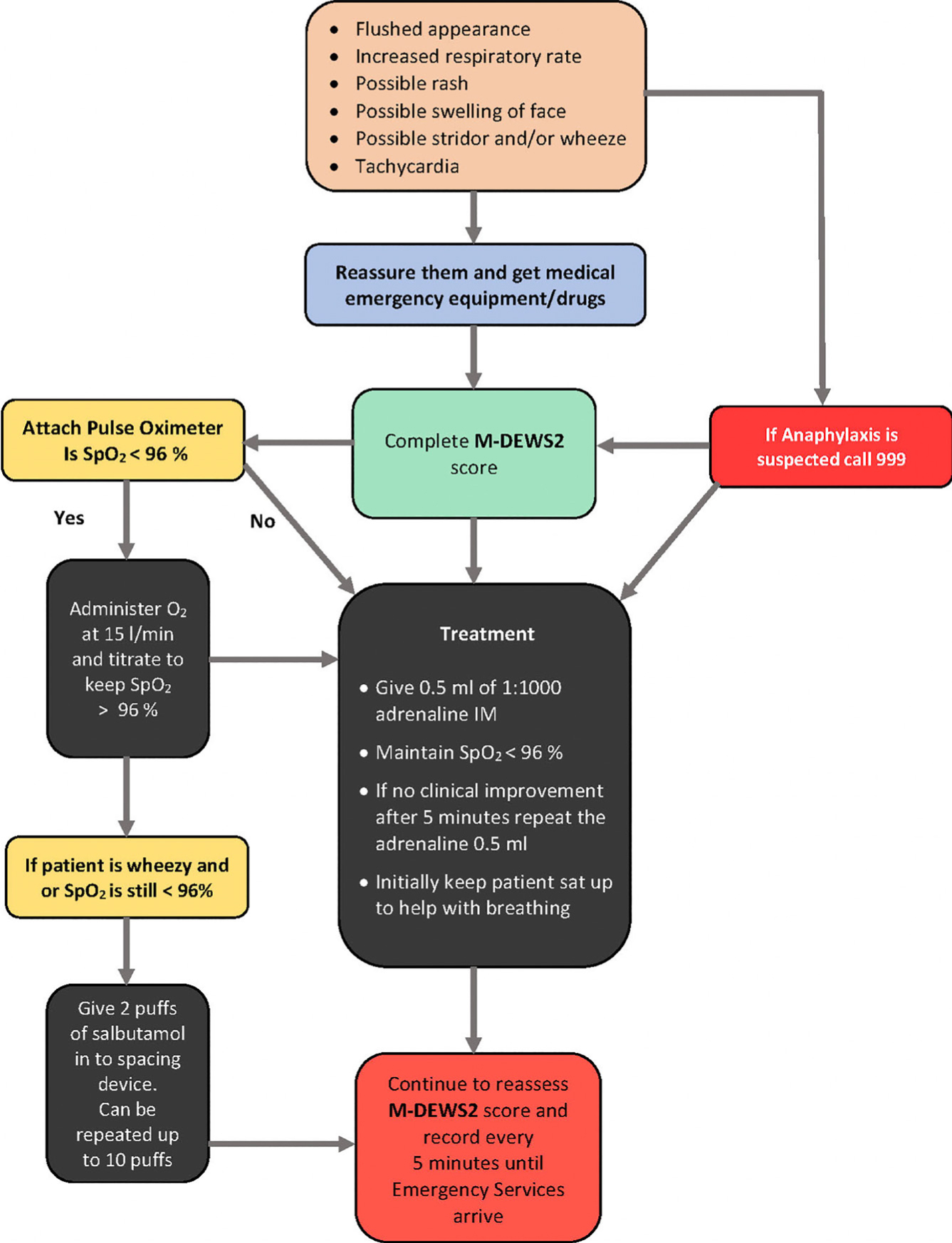
The treatment for anaphylaxis is listed below and also in Figure 5:
If anaphylaxis is suspected then urgent medical assistance is required and an ambulance should be called.
0.5 ml (500 mcg) of 1:1000 adrenaline should be administered intramuscularly for adults and this may be repeated after 5 minutes if no clinical improvement is seen. This dosage for children aged 6–12 years is slightly smaller at 0.3 ml of 1:1000 (300 mcg) adrenaline.
The pulse oximeter should be attached to the patient and high flow oxygen administered at 10–15 l/min titrated to maintain oxygen saturation levels at above 96%.
The ABCDE assessment should be completed and its observations recorded on the M-DEWS2 sheet.
If wheezing is present, or if the patient has difficulty in breathing with oxygen saturation levels at below 96%, then salbutamol should be administered via an inhaler and spacing device, as described in the asthma algorithm (Figure 1).
If the patient has breathing difficulties, then lying the patient supine may not be beneficial initially. However, if there are signs of deterioration and decreased levels of consciousness, then the patient should be laid supine and legs raised.
Patients should continue to be monitored for any signs of deterioration every 5 minutes as per M-DEWS2. If they become unresponsive their vital signs and breathing should be examined. If no vital signs are present, then CPR 10 should be commenced whilst waiting for medical assistance to arrive.
Figure 5. An algorithm which may be used if a patient is suspected of suffering from anaphylactic shock.
Cerebrovascular accident (CVA)
According to the UK Stroke Association, one person every five minutes in the UK suffers a cerebrovascular accident (CVA), otherwise known as a stroke or brain attack. This equates to 150,000 people affected each year and there are a quarter of a million individuals living with long-term disabilities as a result of their stroke. It is the third most common cause of death.11
A CVA occurs when the blood supply to the brain is disrupted. The most common type of stroke (in approximately 85% of cases) is caused by a blockage in an artery which supplies blood to the brain. Such an ischaemic stroke, as with a myocardial infarction, can be due to a clot in the vessel or severe spasm in the vessel. The second type of stroke (haemorrhagic stroke) is caused when a blood vessel in the brain ruptures causing extravasation of blood and necrosis of brain matter.
A transient ischaemic attack (TIA), or ‘mini stroke’ as it is often called, is similar to a ischaemic stroke but symptoms may only last a few minutes and will have completely gone within 24 hours. In a TIA, the blood supply of the brain is interrupted for a short period of time but major infarction of brain tissue does not occur. A TIA should be treated as an emergency as patients who have these episodes are at risk as it may be a precursor to a full CVA. Table 8 lists the clinical features of a CVA/TIA.
▪ Sudden weakness or numbness of the face, arm or leg on one side of the body;
▪ Sudden loss or blurring of vision in one or both eyes;
▪ Sudden difficulty speaking or understanding spoken language;
▪ Sudden confusion;
▪ Sudden or severe headache with no apparent cause;
▪ Dizziness, unsteadiness or a sudden fall, especially with any of the other signs.
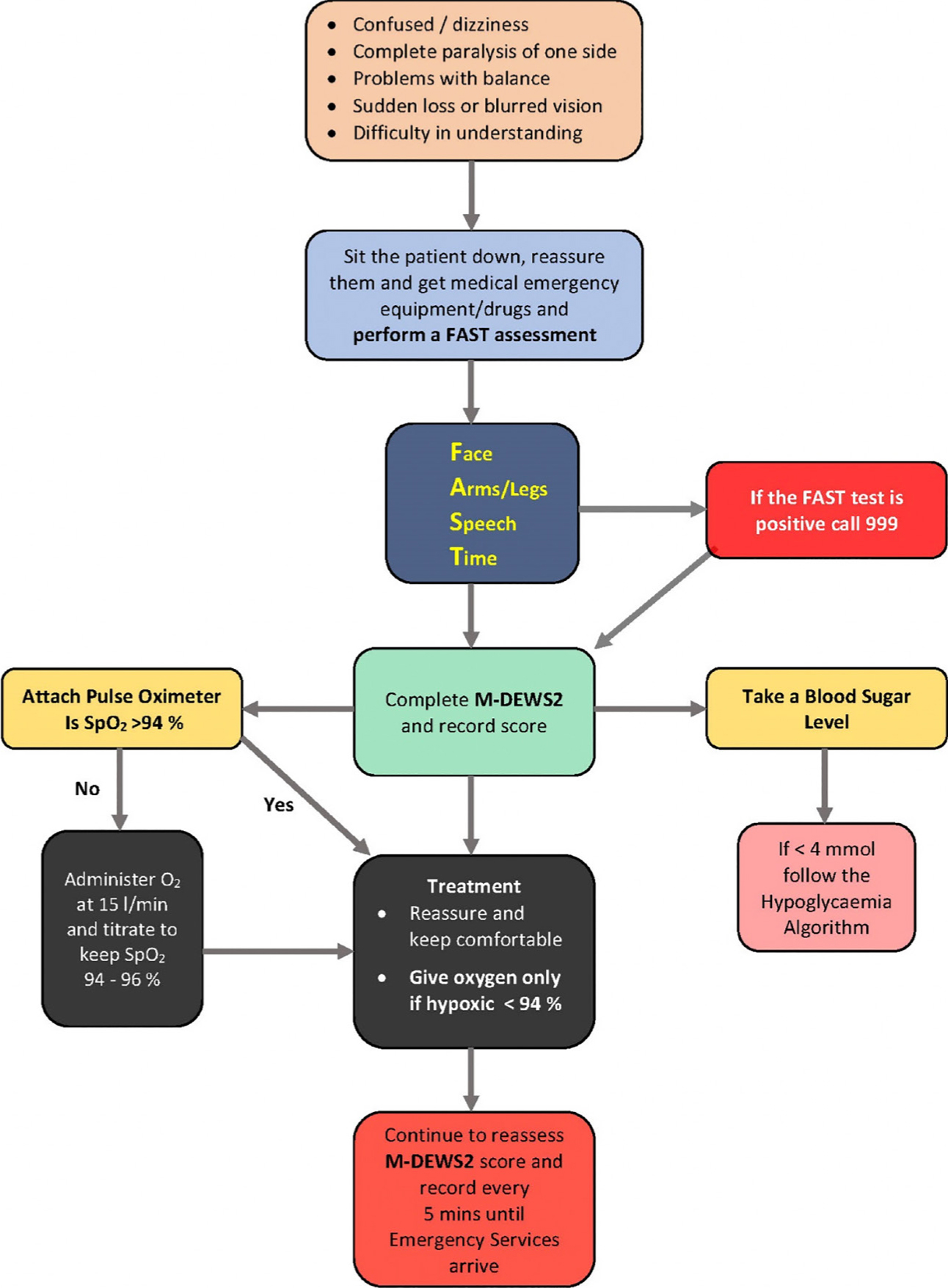
The algorithm for a patient having a CVA is shown in Figure 6. The treatment of a patient having a suspected CVA is as follows:
The patient should be seated and reassured.
A ‘FAST’ assessment should be performed and the emergency services called if the patient is ‘FAST’ positive.
A pulse oximeter should be attached and oxygen administered ONLY if the patient is hypoxic with an oxygen saturation level below 94%.5,7 Most patients having a CVA are not hypoxaemic and, as such, oxygen may be harmful for non-hypoxaemic patients with mild/moderate strokes.
Blood glucose level should be ascertained as, in certain cases, hypoglycaemia can mimic a CVA and, if the blood glucose level is less than 4 mmol, the hypoglycaemia algorithm in Figure 4 should be followed.
The patient should continue to be monitored and a M-DEWS2 score completed every 5 minutes.
The patient should be reassured whilst waiting for the emergency services to attend.
Figure 6. An algorithm which may be used if a patient is suspected of suffering from a cerebrovascular accident.
As with all medical emergencies, early recognition and appropriate referral to hospital ensures that individuals can quickly receive the early treatment that they require. Prompt action in recognizing the features of a stroke can prevent further damage to the brain and assist in the casualty making a full recovery. Any delay in recognition and seeking appropriate care can result in major long-term disabilities, such as communication problems, severe memory loss and paralysis.
Seizures
Seizures are actually quite common and are thought to affect approximately 30,000 people a year in the UK.12 They may occur at any age but are more common before the age of 20. There are a number of reasons that may cause a seizure, with the common ones listed in Table 9. It is, however, important to remember that the casualty having a seizure may not be epileptic. While dental practices in the UK currently contain buccal midazolam in the medical emergency kit, according to the manufacturers of the drug it is only licensed for use in those under the age of 18 and who have previously been diagnosed with epilepsy.13,14Table 10 sets out the clinical features of a seizure.
▪ Febrile convulsions;
▪ CVA;
▪ Head injury;
▪ Meningitis;
▪ Space Occupying Lesion (SOL);
▪ Hypoxia;
▪ Electrolyte abnormalities/imbalance;
▪ Hypoglycaemia;
▪ Drug withdrawal;
▪ Pre-eclampsia;
▪ Drug toxicity and poisoning;
▪ Recreational drugs.
▪ The patient may experience a brief warning or ‘aura’;
▪ Breathing may cease with the lips becoming cyanosed (blue tinge);
▪ The jaws may be clenched;
▪ Stridor;
▪ Incontinence (both urinary and faecal);
▪ May have clonic movements (jerking) of all limbs and head;
▪ Convulsions may be followed by a deep sleep.
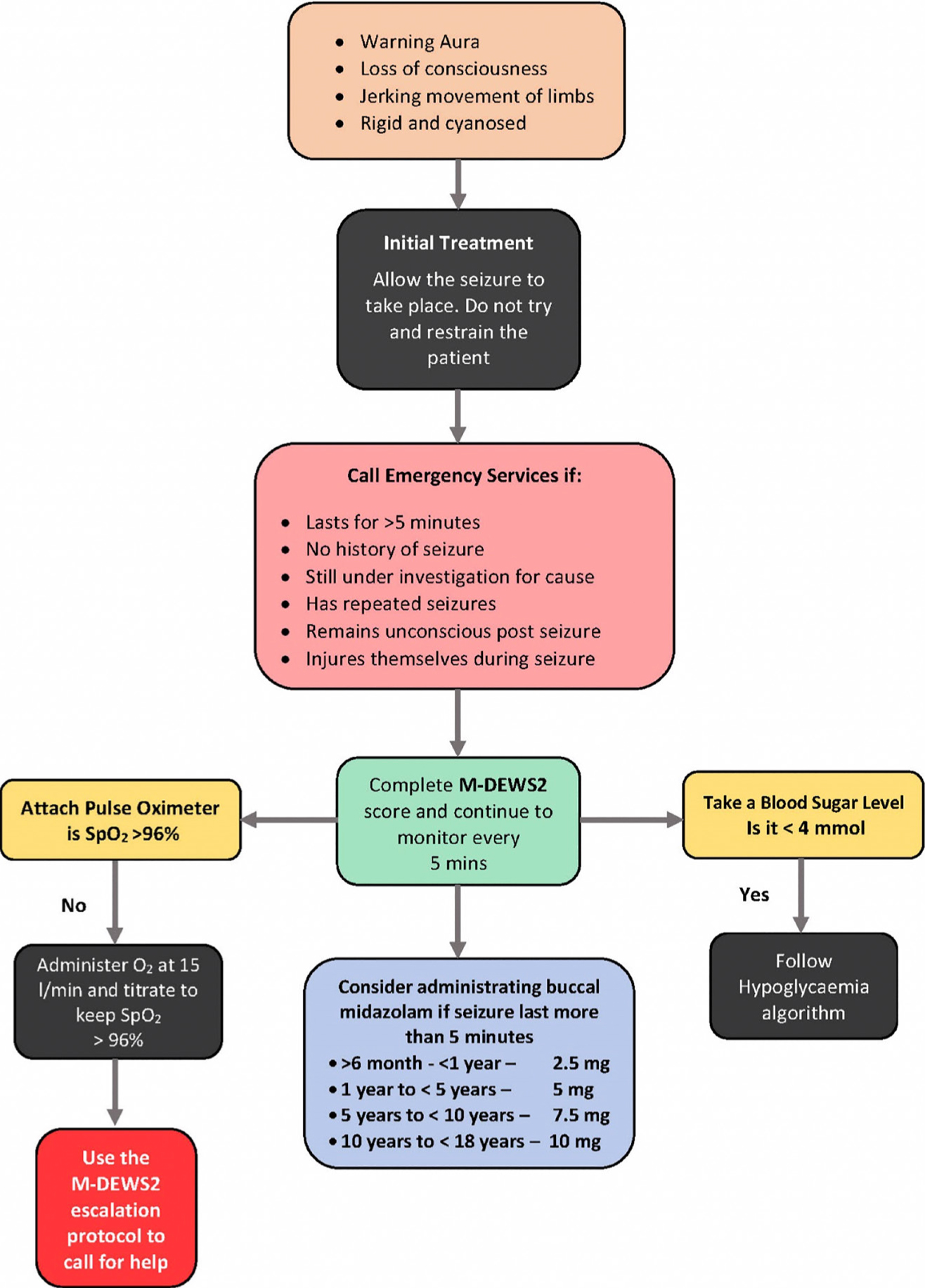
The algorithm for a patient having a seizure is shown in Figure 7 with its treatment set out as follows:
Nothing should be put in the mouth or between the teeth during a convulsion.
Any imminent dangers should be removed from the area around the casualty. Space should be cleared if necessary.
Any clothing around the neck should be loosened.
The time at which the seizure began should be recorded.
The head of the casualty should be supported and protected if required.
The patient should be placed in the recovery position when the convulsion has ceased.
A further assessment should be done and a M-DEWS2 score completed.
High flow oxygen of 10–15 l/min should be administered and titrated to keep SpO2 at above 96%.
Blood sugar level requires to be measured in case of hypoglycaemia.
Figure 7. An algorithm which may be used if a patient is suspected of suffering from seizures.
The services of an ambulance should be requested if:
The casualty has had no previous history of seizures;
If the patient has had a seizure previously and is still being investigated as to its cause;
The seizure lasts more than 5 minutes;
The casualty remains unconscious for more than 10 minutes;
The patient has repeated seizures;
The casualty has sustained an injury during the seizure.
Conclusion
Although the incidence of medical emergencies occurring in the primary dental care environment remains relatively low, they do happen and at any time. Dental care professionals should be competent to assess and provide appropriate treatment, with early diagnosis accepted as being the most critical factor. The use of the M-DEWS2 sheet to assess and recognize the patient who is unwell, combined with the seven algorithms for common medical emergencies, are tools that can assist the dental professional should the need arise.