Ertas U, Yaruz MS, Tozoglu S. Accidental third molar displacement into the lateral pharyngeal space. J Oral Maxillofac Surg. 2002; 60:1217-1219
Huang IY, Wu CW, Worthington P. The displaced lower third molar: a literature review and suggestions for management. J Oral Maxillofac Surg. 2007; 65:1186-1190
Nusrath MA, Banks RJ. Unrecognised displacement of mandibular molar root in to the submandibular space. Br Dent J. 2010; 209::279-280
Gay-Escoda C, Berini-Aytés L, Pinera-Penalva M. Accidental displacement of a lower third molar. Report of a case in the lateral cervical position. Oral Surg Oral Med Oral Pathol. 1993; 76:159-160
Hutchinson D. An unusual case of lingual displacement of a mandibular third molar root apex. Oral Surg Oral Med Oral Pathol. 1975; 39
Arasa LA, Figueiredo R, Escoda CG. Iatrogenic displacement of third molar roots in to the sublingual space: report of 6 cases. J Oral Maxillofac. 2012; 70:e107-e115
Howe GL. Tooth removed from the lingual pouch. Br Dent J. 1958; 104:283-284
Peterson LJ, Ellis E III, Hupp JR, Tucker MR. Contemporary Oral and Maxillofacial Surgery.St Louis: CV Mosby Co; 1988
Iwai T, Matsui Y, Hirota M, Tohnai I. Endoscopic removal of a maxillary third molar displaced into the maxillary sinus via the socket. J Craniofac Surg. 2012; 23
Ozalp B, Kuvat SV, Emekli U. Conservative treatment of displacement mandibular third molar. J Craniofac Surg. 2010; 21:1314-1316
Yeh CJ. A simple retrieval technique for accidentally displaced mandibular third molars. J Oral Maxillofac Surg. 2002; 60:836-837
Jolly SS, Rattan V, Rai SK. Intraoral management of displaced root into submandibular space under local anaesthesia – a case report and review of literature. Saudi Dent J. 2014; 26:181-184
Esen E, Aydoğan LB, Akcali MC. Accidental displacement of an impacted mandibular third molar into the lateral pharyngeal space. J Oral Maxillofac Surg. 2000; 58:96-97
Displacement of Lower Third Molar into the Parapharyngeal Space during Extraction Leah Finan Ahmed Jebril Anand Kumar Dilip Srinivasan Dental Update 2024 47:4, 707-709.
Authors
LeahFinan
BDentSc, MFD RCSI
Dental Core Trainee, Queen's Medical Centre, Nottingham University Hospitals NHS Trust
Lingual displacement of lower third molar teeth is a well-recognized complication of extraction. The purpose of this article is to report the case of a displaced lower third molar tooth into the parapharyngeal space during extraction. A 44-year-old man was referred to the Oral and Maxillofacial Department by his dentist immediately after the event. The case was managed intra-orally under general anaesthetic. Clinicians must be aware of the possibility of lower third molars being displaced during extraction. This article outlines how clinicians should plan the procedure appropriately, take steps to prevent displacements, and how to manage the situation should it arise.
CPD/Clinical Relevance: Displacement is a risk associated with extraction of lower third molar teeth. This risk can be minimized with proper planning and careful execution of the extraction. It is important that the clinician knows this and how to deal with a displaced tooth in practice.
Article
Leah Finan
Lingual displacement of lower third molar teeth, although rare, is a well-recognized complication of extraction.1,2 The most common sites for lower third molar tooth displacement are the sublingual, submandibular and pterygomandibular spaces.3,4 Displacement typically occurs in a lingual direction due to the thinness or absence of the inner cortical bone, as well as application of uncontrolled or excessive force, excessive manipulation, improper surgical planning, or poor clinical and/or radiological assessment.5,6
Case report
A 44-year-old man was referred to the Emergency Department of Queen's Medical Centre, Nottingham in June 2017 following a failed extraction by his General Dental Practitioner (GDP). During the surgical extraction of the lower left third molar (LL8), the patient's tooth was displaced lingually while being elevated. The GDP could not locate the molar tooth lingually and so contacted the maxillofacial team. The patient was brought immediately to the hospital. On examination, the extraction socket of the LL8 was open but no tooth fragment was visible or palpable.
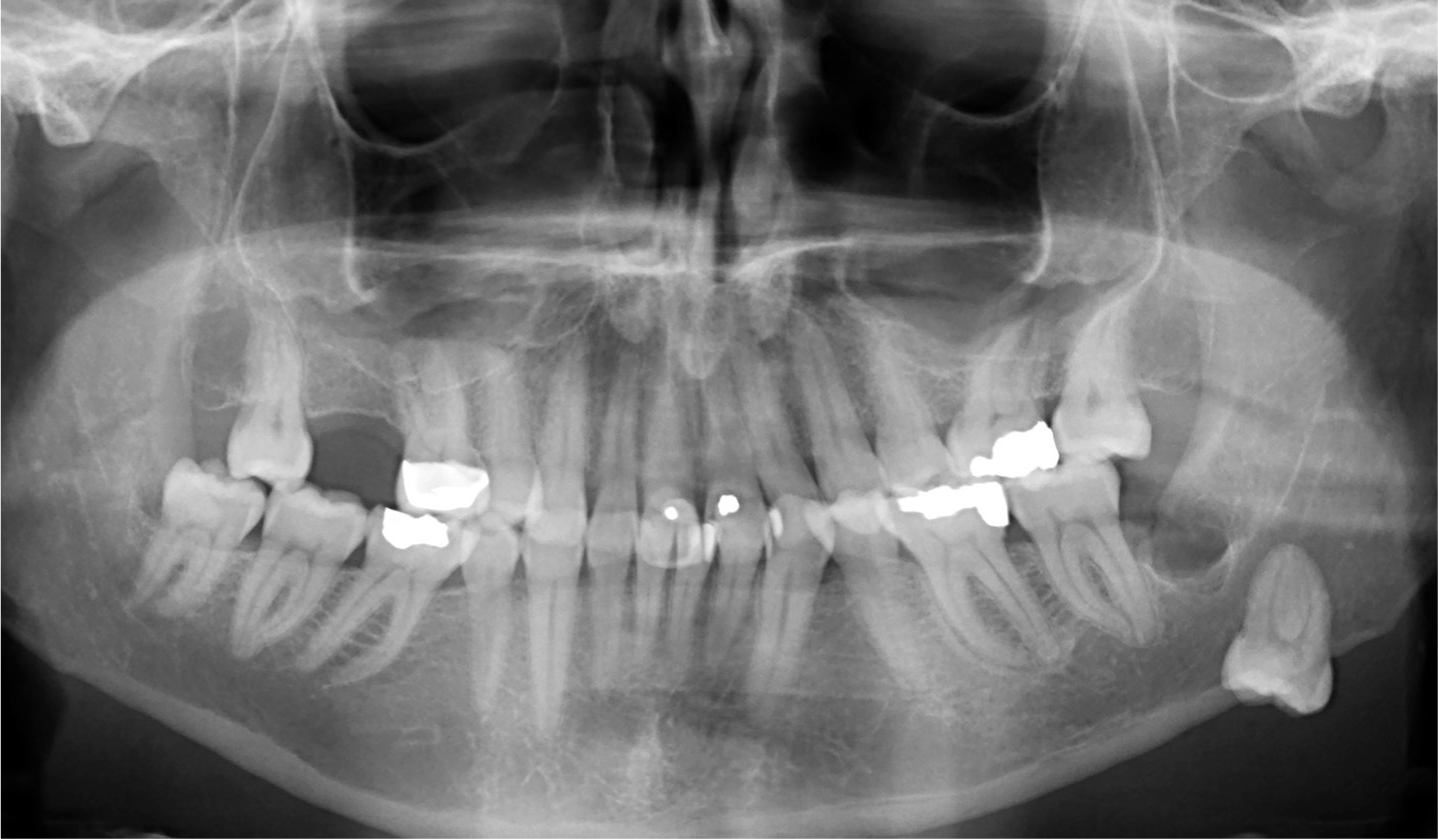
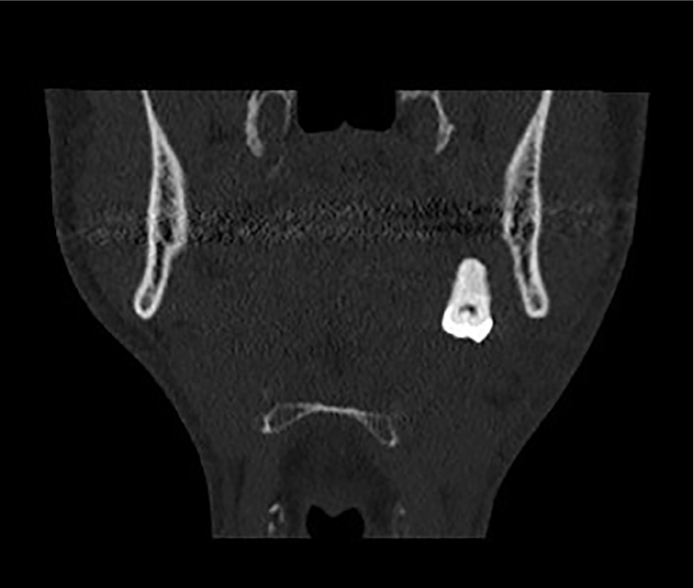
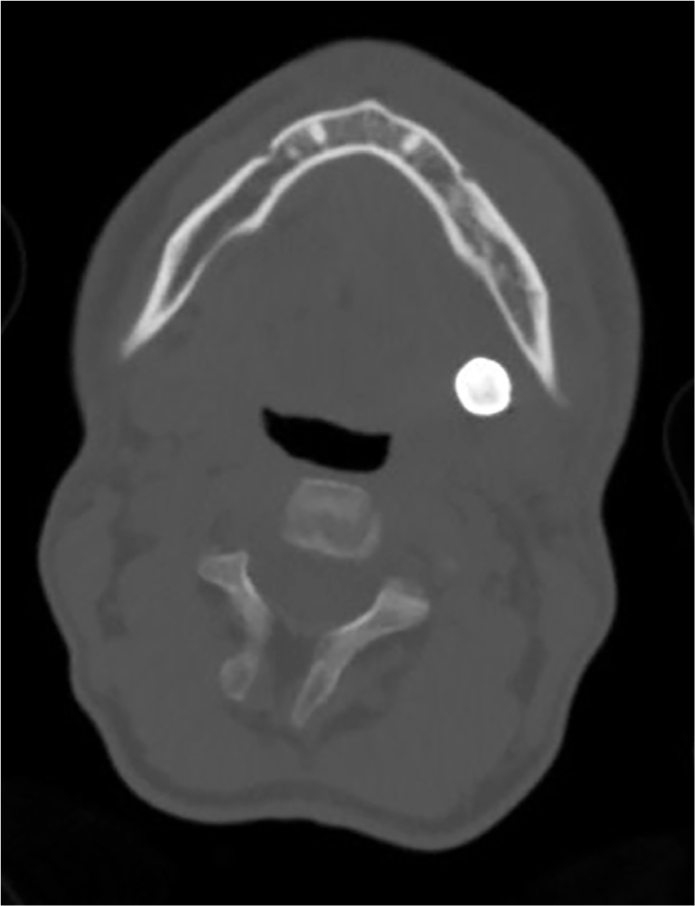
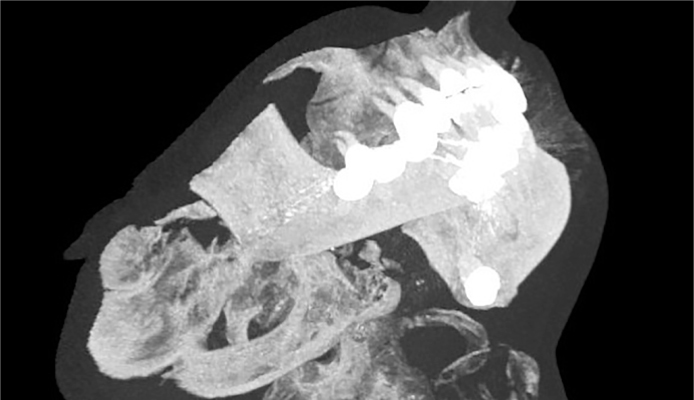
An orthopantomogram was taken to identify the tooth (Figure 1). Following this, a CT scan was taken to locate the LL8 accurately in the parapharyngeal space (Figures 2, 3 and 4).
Figure 1. Orthopantomogram of displaced LL8.Figure 2. CT head coronal view of displaced LL8 in parapharyngeal space.Figure 3. CT head axial view of displaced LL8 in parapharyngeal space.Figure 4. CT head 3D view of displaced LL8 in parapharyngeal space.
Following clinical and radiological examination it was decided to remove this tooth under general anaesthetic. Under general anaesthesia, the displaced LL8 tooth was located using manual palpation of the parapharyngeal space. Using digital pressure, the tooth was manoeuvred along the medial surface of the mandible towards the socket of the third molar. Whilst manoeuvring the tooth, digital pressure was used to ensure that the tooth was not displaced further posteriorly or inferiorly. The tooth was delivered through the socket uneventfully. The patient remained as an inpatient overnight in case any swelling developed and was discharged the following day with no complications.
Discussion
Howe presented the first case of removal of a displaced tooth from the submandibular space in 1958.7 Locating the displaced tooth or tooth fragments is often difficult due to limited space, haemorrhage, and poor visualization.8
Radiography techniques are widely used to locate the displaced tooth/fragment. CT scanning is especially useful as it can precisely identify its 3-dimensional position, as seen in this particular case.9
Differences in direction of displacement, the size of the fragment, delay in retrieval and tissue reactions mean that there is no uniform retrieval technique that can be used.2 Various approaches for the removal of the tooth/fragment have been described, depending on its location.
The conventional method involves a conservative attempt to remove the tooth. However, this technique is limited and surgical removal is often indicated. A lingual mucoperiosteal flap is often sufficient to retrieve a tooth located in the antero-inferior aspects of the pterygomandibular space. However, an extra-oral approach may provide better access if the tooth is displaced deeper into the medial pterygoid or inferiorly into the submandibular space.10,11
It is important that dentists who carry out lower third molar extractions recognize the risks involved and adopt a good surgical technique. Firstly, in the planning phase, dentists should identify from a radiograph the degree of impaction, position of the roots and the bone density surrounding the tooth. During the procedure, they should ensure that they have sufficient access for tooth removal, remove the appropriate amount of bone and avoid excessive force when using elevators. Finger guidance lingually can also be useful in preventing lingual dislocation.3
Should the tooth become dislodged lingually during the procedure, it has been recommended in the literature that the dentist avoids attempting retrieval unless the tooth/fragment is visible and easily accessible. Instead, the dentist should stop the procedure and contact the local oral and maxillofacial department as soon as possible. Relevant information, including pre-operative radiographs, the size of fragment and circumstances surrounding the extraction should be provided.2 It has been reported that a delay in removal of over 24 hours can result in an inflammatory reaction leading to increased pain, swelling, trismus, infection or migration of the root into deeper spaces.1,12,13 If the patient cannot be seen immediately by the oral and maxillofacial team, it is recommended that the dentist cleans the area, sutures the socket and provides the patient with antibiotics.2