Patel J, Jablonski RY, Morrow LA. Complete dentures: an update on clinical assessment and management: Part 1. Br Dent J. 2018; 225:707-714
Atwood DA. Reduction of residual ridges: a major oral disease entity. J Prosthet Dent. 1971; 26:266-279
Cawood JI, Howell RA. A classification of the edentulous jaws. Int J Oral. 1988; 17:232-236
Meyer RA. Management of denture patients with sharp residual ridges. J Prosthet Dent. 1966; 16:431-437
Atwood DA. Clinical, cephalometric, and densitometric study of reduction of residual ridges. J Prosthet Dent. 1971; 26:280-295
Critchlow SB, Ellis JS, Field JC. Reducing the risk of failure in complete denture patients. Dent Update. 2012; 39:427-436
Gahan MJ, Walmsley AD. The neutral zone impression revisited. Br Dent J. 2005; 198:269-272
Friel T. The anatomically difficult denture case. Dent Update. 2014; 41:506-512
McCord JF, Grant AA. Impression making. Br Dent J. 2000; 188:484-492
Thomason JM. The McGill consensus statement on overdentures. Mandibular 2-implant overdentures as first choice standard of care for edentulous patients. Eur J Prosthodont Restor Dent. 2002; 10:95-96
The edentulous ridge classifications most commonly used have their limitations in treatment planning. They do not provide an indication of the complexities that may occur when constructing a new set of complete dentures. The new classification system suggested in this article helps with improved record-keeping, information exchange between colleagues, and communication between patient and clinician.
CPD/Clinical Relevance: The new edentulous ridge classification system links the various edentulous ridge shapes to possible complications that could arise during denture construction.
Article
Wouter Leyssen
The Standards for Clinical Examination and Record-Keeping (Faculty of General Dental Practitioners UK) provides guidance to clinicians on what should be documented during history-taking and a full examination. For patients seeking removable prosthodontic treatment, it is advised that an examination of the denture-bearing tissues is undertaken, noting presence of any tori, undercuts and any other bony or soft tissue lesions.1 This documented information should lead to a clearly recorded diagnosis, treatment option discussion and treatment plan agreed with the patient. This process aids clinicians in assessing the complexity of a case and predicting any challenges that they may encounter. For complete denture construction it will allow the patient to make an informed decision and reflect on whether he/she finds that the benefits of having new dentures outweigh any potential disadvantages.
The assessment for complete denture construction includes previous denture-wearing history, assessment of any available dentures, patient factors such as the ability to adapt to dentures, and an examination of the oral environment. In this regard, the clinician should examine the denture-bearing areas and note down a description of the shape of the residual ridge.2 This information is documented as part of the clinical records and will be part of the diagnosis as this will detail the degree of resorption that has taken place since the loss of the natural teeth. The resorption pattern assists in understanding the success of the final prosthesis. Although there is no proven direct relationship between ridge shape and success of dentures, the initial description of the ridge shape can be useful in discussions as to why previous dentures may not have been successful. The aim of this article is to describe a modified approach to describing edentulous ridge shapes with the objective of aiding in communication between colleagues, and as a tool to patients' anticipated challenges in constructing complete dentures, therefore managing expectations.
Current ridge classifications
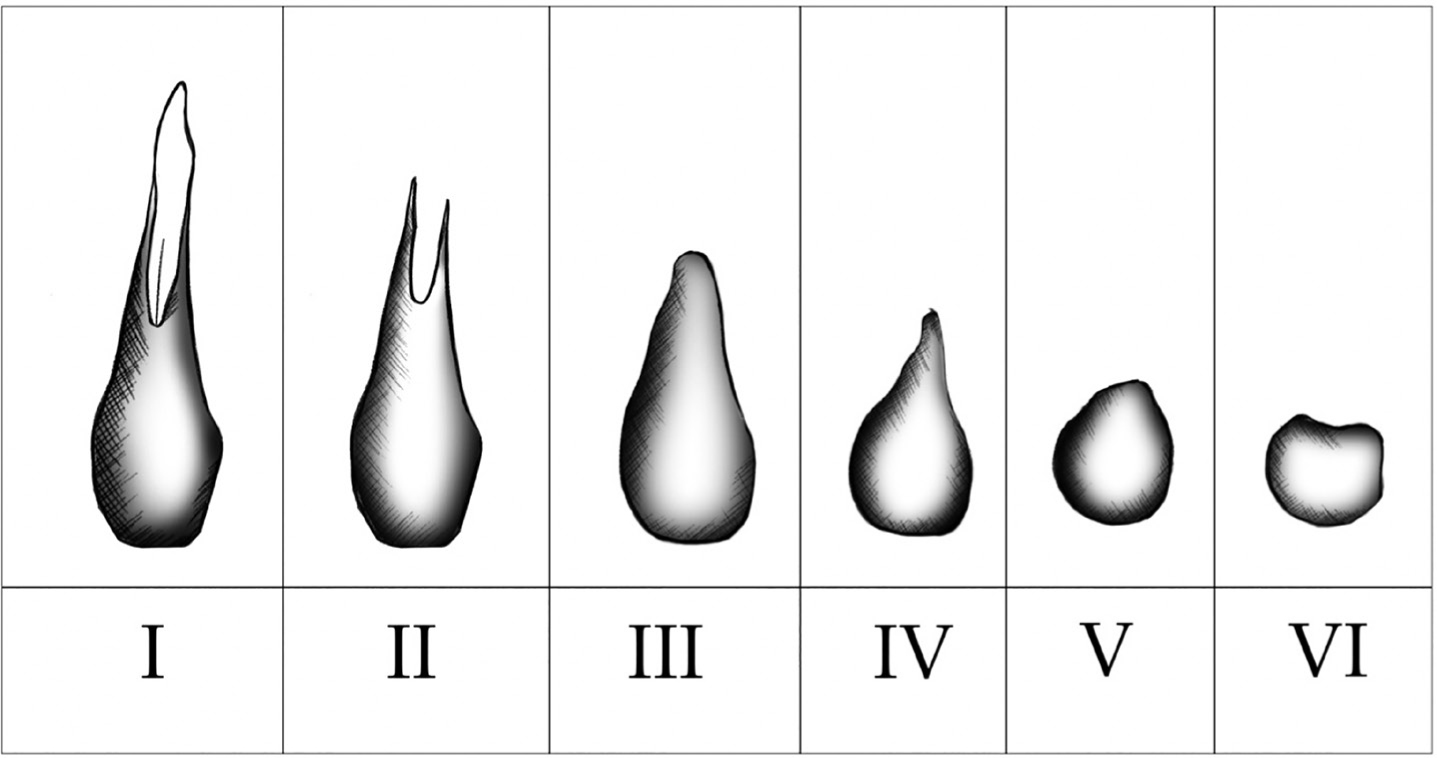
The ridge classifications proposed by Atwood3 (Figure 1) or the modified version of Cawood and Howell4 are intended to provide a quantitative assessment of the residual alveolar bone. However, it may be argued that they have their limitations in prosthodontic treatment planning. For example, they fail to differentiate between the bony support around teeth with an intact periodontium and that of a patient with a severe periodontally-compromised dentition. Both cases would fall under Atwood classification I. The treating clinician would encounter very different clinical challenges in each case where complete denture construction is required. An example includes clinical cases where a clearance due to carious lesions/tooth wear takes place, or where extractions are due to periodontal attachment loss. In such situations, very different ridge shapes may remain following healing. Similarly, Atwood classification II – a ridge immediately post extraction – might inform about the quality of the ridge but not about the quantity of bone nor the ridge shape.
Figure 1. Ridge classification according to Atwood.3
The Atwood, and Cawood and Howell classifications do not provide an indication of the complexities that may occur when constructing a new set of complete dentures. Atwood classification III describes a well-rounded ridge form, which is adequate in height and width. This could be interpreted as a favourable ridge anatomy. It does not take into account those clinical situations where minimal resorption has taken place. This lack of bone resorption may create a challenge in complete denture construction, as there will be limited inter-ridge clearance.
Atwood classification V is defined as a low well-rounded ridge. The clinical management of patients with Atwood ridge classification V and VI often involve similar treatment. The mandibular Atwood classification VI describes the ridge as having a depressed ridge form, with some basilar loss evident. This is not specific enough and requires more detail. Atwood classification VI represents a spectrum of ridge shapes from a small central depression with a bony buccal and lingual ridge to partial or complete loss of the lingual ridge. Extensive lingual resorption leads to a complex ridge anatomy that is difficult to treat, whereas a small central depression does not necessarily require a different clinical approach than that which is normally employed for a ridge classification V.
A new edentulous ridge classification providing an accurate description of the bony ridge shape applicable to denture construction therefore seems warranted. The ridge shape could then be linked to any potential problems which might be encountered during denture construction. The new classification described below could help in treatment planning for denture construction and potentially for the planning of placement of implants.
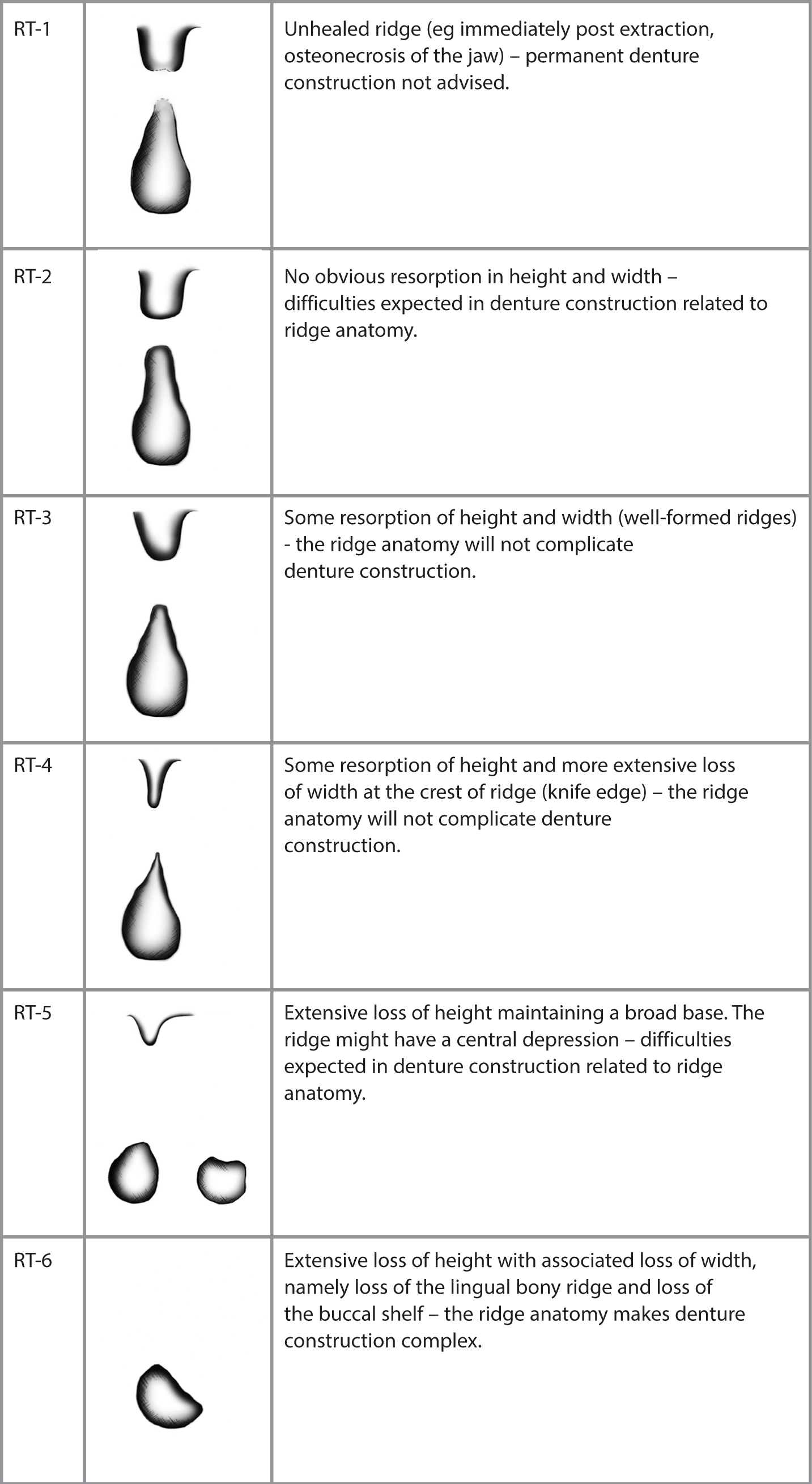
Figure 2. New ridge classification. RT Ridge Type.
Ridge Type 1
Definition: Unhealed ridge, the ridge shape will change in the near future. Definitive denture construction is not recommended. Examples include, but are not limited to, recent extraction sites, osteonecrosis (Figure 3) or prolapsed antrum (Figure 4).
Figure 3. Osteonecrosis. (Photo courtesy of Dr U Patel).Figure 4. Prolapsed antrum.
Ridge Type 2
Definition: No obvious resorption in height and width – high profile and rounded (Figures 5 and 6).
Figure 5. Ridge type 2 – Maxilla.Figure 6. Ridge Type 2 – Mandible.
Impression-taking will seem straightforward, however, the buccal sulcus width is narrow and sometimes more difficult to capture – especially with a spaced special tray prescribed to deal with the (posterior) bony undercuts. Impression material will need to be elastic, such as alginate.
Denture construction may be difficult due to the presence of bony undercuts which prevent close adaptation of the denture base in these deeper undercuts to the denture-bearing area. The spacing might break the seal and therefore lead to loss of retention.
Buccal flanges in the anterior segment will inevitably increase lip support. Some patients prefer dentures with a ridge-lapped design omitting the buccal flange. The height of the ridges limits the space available to construct dentures. There might be difficulties obtaining sufficient freeway space. The space available would need to allow for a sufficient thickness of the acrylic denture base and will limit the space available for the crown height of the acrylic teeth. This could lead to the need for setting up small/short acrylic teeth onto the denture.
The positioning of the anterior teeth might be another difficulty as they would need to be set up on the crest of the voluminous ridge. Failing this, in the maxillary arch, the nasolabial angle would be increased, affecting the facial profile.
Ridge Type 3
Definition: Some resorption of height and width – high profile and rounded (Figures 7 and 8).
Figure 7. Ridge Type 3 – Maxilla.Figure 8. Ridge Type 3 – Mandible.
Impression-taking is straightforward. Elastic and non-elastic impression materials can be used, depending on the presence of undercuts. There would not be any specific issues to take into consideration for denture construction related to ridge anatomy.
Ridge Type 4
Definition: Some resorption of height and more extensive loss of width at the crest of the ridge - high profile knife edge (Figures 9 and 10).
Figure 9. Ridge Type 4 – Maxilla.Figure 10. Ridge Type 4 – Mandible.
Impression-taking is generally uncomplicated and elastic or non-elastic impression materials can be used. A permanent resilient liner might be indicated on the fit surface. Alternatively, the laboratory could apply a tinfoil spacer on the crest of the ridge on the master cast before processing the denture (base). Retention of the lower denture with this ridge type may be inferior to Type 3 ridges.
This shape of ridge may mainly be found in the anterior ridge of the mandible and for patients who have worn dentures for long periods of time.5,6 A subdivision is suggested in the saw-tooth ridge, the razor-like ridge and the ridge with discrete large spiny projections. These subdivisions are made on the radiographic image of the ridge as they are often covered by flabby soft tissue. As the radiographic image of edentulous ridges is not always available and X-ray imaging would not be justified just on the basis of providing a more precise classification, no subdivision of ridge shape is suggested.
This ridge shape often leads to complaints of pain, which presents as either chronic or persistent soreness under the denture, particularly during mastication. Creating tin foil relief areas in the laboratory over the painful regions will help to distribute load over the denture-bearing area. However, over time the soft tissues will adapt and fill the relief space. The tissues will then become traumatized as they are trapped between the denture and sharp bone. The patient should be warned that such trauma could re-occur.5
Ridge Type 5a
Definition: Extensive loss of height maintaining a broad base – low profile and flat appearance (Figures 11 and 12) Impression-taking will be more technique sensitive. The use of a viscous impression material for primary impressions is recommended (eg heavy body silicone or compound). Although there is no evidence for the use of special trays, their use is considered to be good practice.7 In the situation of a poor ridge form, they are thought to decrease the risk of over extension from occurring. Special trays can more clearly indicate to the lab the functional width and depth of the sulcus. Impression material for the master impression may be elastic (eg medium/light body silicone) or non-elastic (eg zinc oxide eugenol).
Figure 11. Ridge Type 5 – Maxilla.Figure 12. Ridge Type 5a – Mandible (flat with string of soft tissue).
Another difficulty might be that temporary bases used during jaw registration are more likely to be displaced during manipulation. In some cases, better results can be achieved when heat-cured acrylic bases are used.8,9
Ridge Type 5b (only for mandible)
Definition: Extensive loss of height maintaining a broad base with a buccal and lingual bony ridge and a central depression – low profile and a central depression (Figure 13).
Figure 13. Ridge Type 5b – Mandible - central depression palpable in posterior areas but not clearly visible.
For denture construction similar principles apply as for classification 5a. The clinical presentation is slightly different as there is a central depression. This does not affect the technique of denture construction.
Ridge Type 6 (only for mandible)
Definition: Extensive loss of height with associated loss of the lingual bony ridge and loss of the buccal shelf – low profile and narrow base (Figures 14 and 15).
Figure 14. Ridge Type 6 – Mandible.Figure 15. Ridge Type 6 – Mandible – tongue raised.
Impression-taking is difficult as there is only a narrow strip of keratinized mucosa present. Primary impressions are always over extended and the use of viscous impression material is essential to capture the mucosa covering the remaining bony ridge. The soft tissues of the floor of the mouth and the cheeks tend to cover the denture-bearing area. Special trays have a distinct shape and ordinary impression materials could fail to capture sufficient detail. Admix is one of the few materials described for taking impressions of this type of ridge (Figure 16). Admix consists of 3 parts by weight of (red) impression compound to 7 parts by weight of greenstick. The constituents are placed into hot water and mixed together by kneading with vaselined, gloved fingers. Using a standard impression technique, the lower impression is recorded. The working time of this admix before it cools down is 1–2 minutes.10 Most bases have some over-extension. Some patients manage as they have been denture-wearers for a long time and they have adapted to the present situation. Other patients will benefit from implant placement to retain and/or support the lower acrylic denture.11
Figure 16. Admix impression.
Similar to classification 5, the jaw registration might be more difficult to complete due to unstable bases. The lower dentures are often painful – even when a permanent resilient lining is used – and multiple review appointments are generally needed to make the dentures comfortable. This is no surprise as the only bony support is provided by a sharp ridge surrounded by high muscle attachments. This situation is very unfavourable for conventional denture construction.
Conclusion
It is sometimes difficult to describe ridge anatomy accurately using the most common ridge classifications available. They have their limitations for treatment planning and communication between colleagues. The suggested new Ridge Type classification not only clearly represents the various edentulous ridge shapes encountered during clinical practice, it also relates them to possible complications that could arise during denture construction. To facilitate the transition to the new classification system Ridge Type 3 and Ridge Type 4 match the old classification systems. Ridge Type 1 and 2 are not commonly used in the previous classification and 5a, 5b and 6 are new additions which would make the clinician alert to the new classification system being used. The improved record-keeping would facilitate information exchange between colleagues and communication between patient and clinician and therefore dental universities should consider adopting this classification into their curriculum. The new classification will be introduced at Birmingham Dental Hospital during the academic year 2019/2020 and data collection regarding the use of the new classification will be undertaken subsequently.