Lund VJ. Anatomy and physiology of the nasal cavity and paranasal sinuses. In: Raeburn D, Giembycz MA (eds). Basel: Birkhäuser; 1997
Pohunek P. Development, structure and function of the upper airways. Paediatr Respir Rev. 2004; 5:2-8
Luc H. Une nouvelle methode operatoire pour la cure radicale et rapide de l'empyeme chronique du sinus maxillaire. Arch Int Laryngol d'Otol Rhinol. 1897; 77-93
Caldwell GW. Diseases of the accessory sinuses of the nose, and an improved method for suppuration of the maxillary antrum. NY Med J. 1893; 58:526-528
Osashi Y, Nakai Y, Ikeoka H Effects of bacterial endotoxin on the ciliary activity in the in vitro eustachian tube. Arch Otorhinolaryngol. 1987; 224:88-90
Abou-Hamad W, Matar N, Elias M, Nasr M, Sarkis-Karam D, Hokayem N, Haddad A. Bacterial flora in normal adult maxillary sinuses. Am J Rhinol Allergy. 2009; 23:261-261
Rosenfeld RM, Piccirillo JF, Chandrasekar SS Clinical practice guideline (update): Adult sinusitis. Otolaryngol Head Neck Surg. 2015; 152:(2 Suppl)S1-S39
Clinical Knowledge Summaries: Sinusitis.: Public Health England; 2018
Graf P. Long-term use of oxy- and xylometazoline nasal sprays induces rebound swelling, tolerance, and nasal hyperreactivity. Rhinology. 1996; 34:9-13
Hildenbrand T, Weber R, Heubach C, Mösques R. Nasal douching in acute rhinosinusitis. Laryngorhinootologie. 2011; 90:346-351
Ahovuo-Saoranta A, Rautakorpi UM, Borisenko OV Antibiotics for acute maxillary sinusitis in adults. Cochrane Database Sys Rev. 2014; 11
Sinusitis (Acute): Antimicrobial Prescribing. (NG79).: Public Health England; 2017
Setzen G, Ferguson BJ, Han JK Clinical consensus statement: appropriate use of computed tomography for paranasal sinus disease. Otolaryngol Head Neck Surg. 2012; 147:808-816
Maniglia AJ, Goodwin WJ, Arnold JE Intracranial abscesses secondary to nasal, sinus, and orbital infections in adults and children. Arch Otolaryngol Head Neck Surg. 1989; 115:1424-1429
Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope. 1970; 80:1414-1428
Andrews AE, Bryson JM, Rowe-Jones JM. Site of origin of nasal polyps: relevance to pathogenesis and management. Rhinology. 2005; 43:180-184
Bell GW, Joshi BB, MacLeod RI. Maxillary sinus disease: diagnosis and treatment. Br Dent J. 2011; 210:113-118
DeConde AS, Soler ZM. Chronic rhinosinusitis: epidemiology and burden of disease. Am J Rhinol Allergy. 2016; 30:134-139
Kokkens WJ, Lund VJ, Mullol J European position paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl. 2012; 23:1-298
Jayawardena ADL, Chandra R. Headaches and facial pain in rhinology. Am J Rhinol Allergy. 2018; 32:12-15
Aqius AM, Sama A. Rhinogenic and nonrhinogenic headaches. Curr Opin Otolaryngol Head Neck Surg. 2015; 23:15-20
Godley FA, Casiano RR, Mehle M, McGeeney B, Gottschalk C. Update on the diagnostic considerations for neurogenic nasal and sinus symptoms: a current review suggests adding a possible diagnosis of migraine. Am J Otolaryngol. 2019; 40:306-311
Caten A, Johnson C, Jang D, Gurrola J, Kountakis S. Comorbidities in patients with all positive symptoms on sinonasal outcome test quality of life instrument. Laryngoscope. 2015; 125:2648-2652
Frieri M, Argyriou A. Is there a relationship between fibromyalgia and rhinitis?. Allergy Asthma Proc. 2012; 33:443-449
Baraniuk JN, Zheng Y. Relationships among rhinitis, fibromyalgia, and chronic fatigue. Allergy Asthma Proc. 2010; 31:169-178
Cox DR, Ashby S, DeConde AS Dyad of pain and depression in chronic rhinosinusitis. Int Forum Allergy Rhinol. 2016; 6:308-314
Chester AC. Symptoms of rhinosinusitis in patients with unexplained symptoms of chronic fatigue or bodily pain. Arch Int Med. 2003; 163:(15)1832-1836
Barham HP, Zhang AS, Christensen JM, Sacks R, Harvey RJ. Acute radiology rarely confirms disease in suspected recurrent acute rhinosinusitis. Int Forum Allergy Rhinol. 2017; 7:726-733
Chandra RK, Conley DB, Kern RC. Nasal polyposis.Ch14. In: Kennedy DW, Hwang PH (eds). New York: Thieme Medical Publishers; 2012
Loevner LA, Mikityansky I. Radiological imaging of the paranasal sinuses and skull base. Ch3. In: Kennedy DW, Hwang PH (eds). New York: Thieme Medical Publishers; 2012
Kenndey DW, Ramakrishnan VR. Functional endoscopic sinus surgery: concepts, surgical indications and techniques. Ch25. In: Kennedy DW, Hwang PH (eds). New York: Thieme Medical Publishers; 2012
West B, Jones NS. Endoscopy-negative, computed tomography – negative facial pain in a nasal clinic. Laryngoscope. 2001; 111:581-586
Fahy C, Jones NS. Nasal polyposis and facial pain. Clin Otolaryngol Allied Sci. 2001; 26:510-513
Wilson PS, Grocutt M. Mucosal thickening on sinus X-rays and its significance. J Laryngol Otol. 1990; 104:694-695
Lim CG, Spanger M. Incidental maxillary sinus findings in patients referred for head and neck CT angiography. Singapore Dent J. 2012; 33:1-4
Hirsch SD, Reiter ER, DiNardo LJ, Wan W, Schuman TA. Elimination of pain improves specificity of clinical diagnostic criteria for adult chronic rhinosinusitis. Laryngoscope. 2017; 127:1011-1016
Russell MB, Olesen J. Migrainous disorder and its relation to migraine without aura and migraine with aura. A genetic epidemiological study. Cephalgia. 1996; 16:431-435
Kelman L. Migraine pain location: a study of 1283 migraineurs. Headache. 2005; 45:1038-1047
Riesco N, Pérez-Alvarez AI, Verano L Prevalence of cranial autonomic parasympathetic symptoms in chronic migraine: usefulness of a new scale. Cephalalgia. 2016; 36:346-350
Kari E, Del Gaudio JM. Treatment of sinus headache as migraine: the diagnostic utility of triptans. Laryngoscope. 2008; 118:2235-2239
Lal D, Rounds A, Dodick DW. Comprehensive management of patients presenting to the Otolaryngologist for sinus pressure, pain, or headache. Laryngoscope. 2015; 125:303-310
Schiffman E Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache. 2014; 28:6-27
Peric A, Rasic D, Grguevic U. Surgical treatment of rhinogenic contact point headache: an experience from a tertiary care hospital. Int Arch Otorhinolaryngol. 2016; 20:166-171
Herzallah IR, Hamed MA, Salem SM, Suuma MV. Mucosal contact points and paranasal sinus pneumatisation: does radiology predict headache causality?. Laryngoscope. 2015; 125:2021-2026
The Maxillary Sinus: What the General Dental Team Need to Know Part 1: Paranasal Sinus Physiology, Infective Disease and Diagnosis of Pain Garmon W Bell Iain Macleod James C Darcey Collin Campbell Dental Update 2024 47:4, 707-709.
Authors
Garmon WBell
BDS, MSc, FDC RCS, FFD RCSI(OS)
Associate Specialist Oral and Maxillofacial Surgery, Dumfries and Galloway Royal Infirmary
This first paper of a four-part series guides the dental team through paranasal sinus physiology and how muco-ciliary clearance is interrupted in disease, particularly infection. The role of acute rhinosinal infection is discussed in relation to orofacial pain and headache. The broad differential diagnosis of what many patients regard as sinus-related pain is discussed, emphasizing the importance of the patient history and clinical examination to reach a correct diagnosis and to avoid inappropriate antibiotic prescription or unnecessary surgery.
CPD/Clinical Relevance: Many patients relate their chronic facial pain and headaches to disorders of their sinuses simply because the pain overlies the location of the paranasal sinuses. Following diagnostic criteria, and application of such to reach an accurate diagnosis, will improve patient care. Inter-specialty co-operation is essential in the management of chronic orofacial pain and headaches.
Article
Garmon W Bell Iain MacLeod James C Darcey Collin Campbell
The paranasal sinuses have a unique and multifunctional role in the upper respiratory tract and base of the skull,1 and it is the maxillary sinus that impacts most on the role of the General Dental Practitioner (GDP). The sinuses are thought to warm and humidify inhaled air, and reduce the weight of the facial skeleton. Increasingly, the paranasal sinuses are recognized for the role played in innate and adaptive immunity.1
In this first of four papers, paranasal sinus physiology will be discussed and how interruption of those physiological processes, as a result of infection, contribute to orofacial pain and very occasionally headaches.
Paranasal sinus development
The paranasal sinuses are named after the bones within which they lie develop as epithelial outgrowths from the nasal cavity. Named after the maxillary, ethmoid, sphenoid and frontal bones, the location and three-dimensional anatomy of the paranasal sinuses in the adult are best viewed in a colour atlas of cross-sectional anatomy.
In the young child, the paranasal sinuses are minimally developed. The maxillary and ethmoid sinuses begin development around the third month of intra-uterine life, are present at birth, and have reached almost full adult size by puberty, although continue to pneumatize the bones within which they lie throughout life. The sphenoid sinuses develop after birth, becoming pneumatized by the age of five and, although they also reach adult size by puberty, they continue to enlarge through life. The frontal sinuses are the last to develop as an out-budding from the epithelium of the anterior ethmoid air cells, only reaching full size by the late teenage period.2
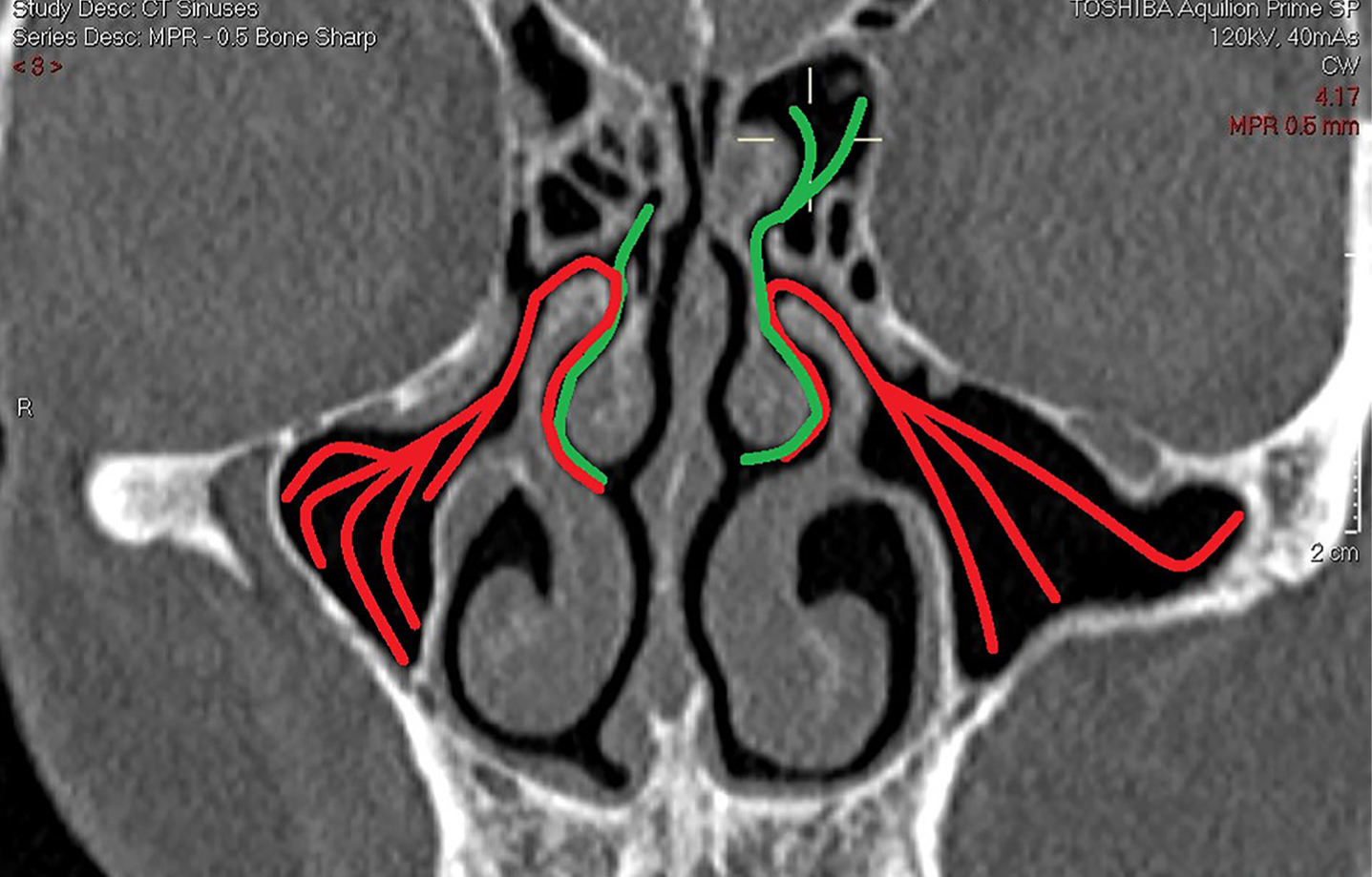
All of the sinuses drain into the nasal cavity through epithelized channels called ostia. The drainage of the maxillary sinus is complicated in that the ostium that opens into the nasal cavity is high up on the medial wall, close to the orbit, such that drainage has to occur against gravity. The ethmoid and maxillary sinuses drain into the middle meatus, below the middle turbinate. The location of this is often termed the osteo-meatal unit (Figure 1).
Figure 1. Coronal reconstruction of multi-slice computed tomographic image at location of osteo-meatal unit demonstrating direction and pattern of muco-cilary clearance from ethmoid (green) and maxillary sinuses (red).
Paranasal sinus physiology
Historically, the paranasal sinuses were thought to drain by gravity, and it was for this reason that early treatment for infection of the maxillary sinus in the pre-antibiotic era often involved creating an antrostomy as inferiorly as possible on the medial wall of the sinus, on the lateral wall of the nose below either the inferior or middle turbinates.3,4 Surgical drainage of maxillary sinus infection into the mouth through an extraction site was also performed.5 The development of electron microscopy increased understanding of cell function and immunology changed that concept.
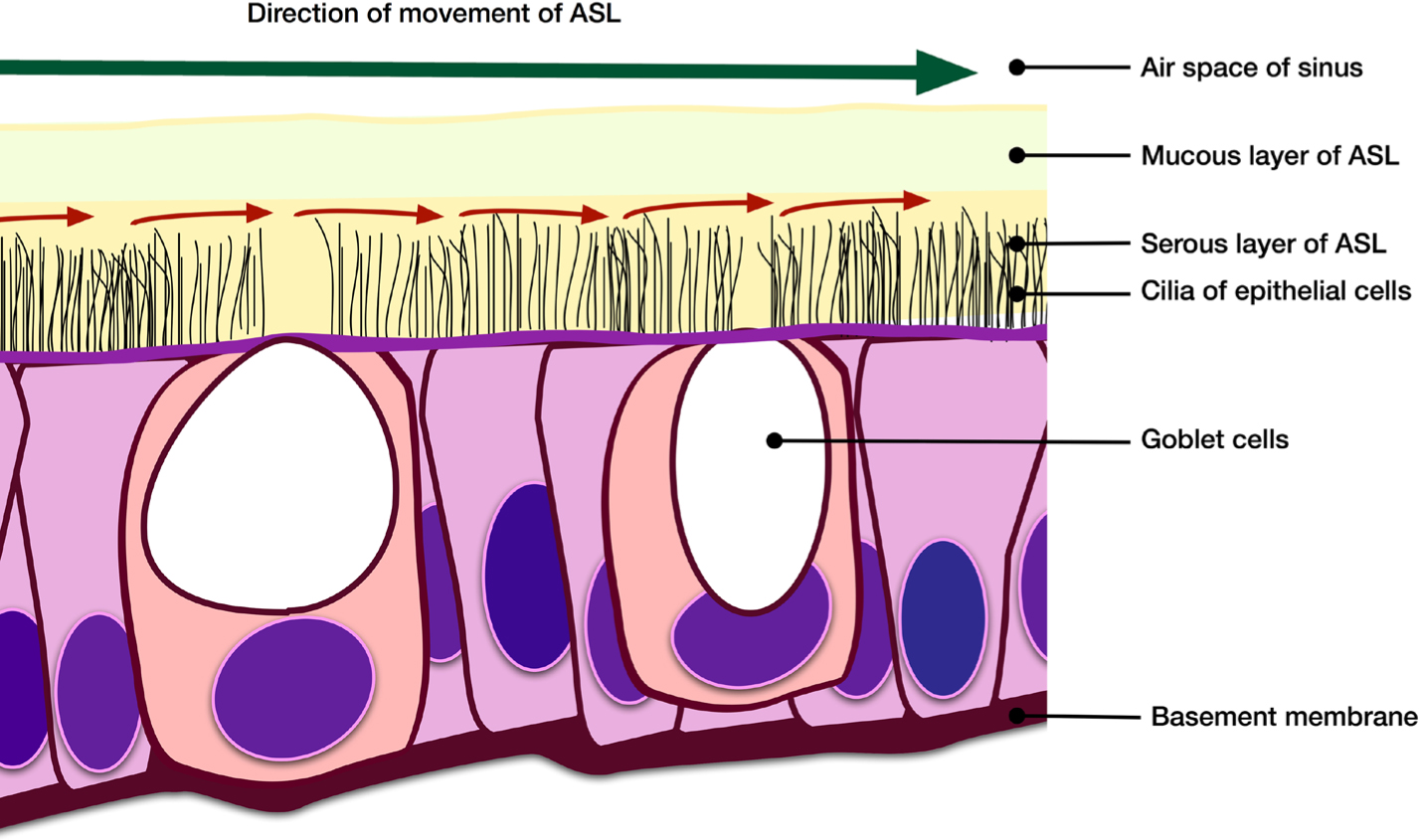
All paranasal sinuses, including the nasal cavity, are lined with pseudo-columnar ciliated epithelium, among which is interspersed goblet cells and a few sero-mucous salivary gland cells.6,7 It is the interactive role of the cilia and the secretions of the goblet cells that contributes to the special physiological environment within the paranasal sinuses8 (Figure 2)
Figure 2. Illustration demonstrating ciliary activity in conjunction with goblet cell secretions forming the airway surface layer (ASL) to achieve muco-ciliary clearance of debris from paranasal sinus surface.
The goblet cells secrete a complex blend of diverse glycoproteins (mucins), lysozymes and lactoferrins, alongside many other immune-modulating factors, including cytokines.6,7,8,9 The mucin layer sits on top of the liquid phase layer which has a specific acid-base balance in health for optimal function.10
Within the liquid phase layer lie the cilia. The cilia, approximately 6μm in length, have a unique internal structure of dynein fibrils that enable controlled movement.11 The cilia of the respiratory epithelium beat in a synchronized motion, usually at a rate of 10–20 times per second in health, reducing to 5 or less in the presence of infection or irritants.11
It is the combined action of the cilia and the liquid/gel phase of the airway surface layer that traps microbial organisms and foreign bodies, propelling them to the maxillary ostia for removal via muco-ciliary clearance (Figure 1). The descriptive term gel on water, or gel on a brush, has been used to describe the interaction of the cilia with the mucin and liquid phases of the airway surface layer, which in health moves at a rate of 10 mm per minute, often against gravity and not in the most direct route to the ostium.11 The rate is reduced in disease. Impaired muco-ciliary clearance contributes to stasis and infection, and may arise through ciliary dyskinesia or changes in mucous secretion.11 Primary ciliary dyskinesia occurs through deranged protein coding in the formation of the dynein fibrils, usually as a result of genetic disease.11 Secondary ciliary dyskinesia is caused by infection, or environmental influences.11 Diseases, such as cystic fibrosis, will produce a mucous layer that becomes dehydrated, shrinks and impinges on the underlying serous layer, thereby impairing normal ciliary movement.11,12 Excessive production of mucous with an increased viscosity in Chronic Obstructive Pulmonary Disease (COPD) and asthma, as a result of goblet cell metaplasia, also impedes normal ciliary movement.10,11,13
From the perspective of the Dental Team, impaired muco-ciliary clearance, as a result of secondary ciliary dyskinesia, arises when oral micro-organisms move into the maxillary sinus, or when dental materials are introduced. The endotoxins produced by bacteria impair normal ciliary activity.14 The impaired muco-ciliary function, with or without oral microbial contamination, will result in stasis and lead to infection, usually bacterial or fungal.11
Paranasal sinus infection
Paranasal sinus infection is classified as either acute or chronic and may arise as a result of viruses, bacteria and fungi. The paranasal sinuses are self-cleansing air-filled, humidified spaces, that in health have a limited and balanced microbial flora.15,16
Acute paranasal sinusitis, usually of viral aetiology, characteristically arises a few days after the patient is recovering from an acute upper respiratory tract infection, most often, the common cold. The characteristic biphasic presentation is that of an individual who has just started to feel better after 4–5 days of acute upper respiratory symptoms, to relapse with acute intense pain in the mid-face or frontal area.17 When the maxillary sinus is involved, patients may also complain of toothache.17
The acute sinusitis will usually settle in one week, with or without treatment. Guidelines recommend symptom control with nasal decongestants, topical steroids sprays and analgesia.17,18 Nasal decongestants should not be used regularly for prolonged periods as rebound mucosal oedema occurs when they are stopped.19 Nasal douching with saline can ease symptoms.20
Most cases of acute paranasal sinus infection are of viral origin.17 Approximately 2% are of bacterial origin.17 The acute viral sinusitis should resolve in 10 days. If not, consideration should then be given to the possibility of bacterial acute sinusitis as a secondary infection.17 If there is bacterial rhinosinal disease, the clinician would expect the patient to report nasal obstruction and purulent nasal discharge. Systemic antibiotics are rarely required unless the patient is pyrexic, or there are other signs of spreading infection.17 Clinical guidelines provide evidence-based recommendations relating to antibiotic prescription.17,18,21,22 The antibiotic of choice is co-amoxiclav. Second line antibiotics are macrolides and tetracyclines.21,22 Radiological investigation is not indicated unless there are signs of spreading infection.17,23
Acute bacterial rhinosinal disease in severe cases can present with orbital and intracranial extension and the clinical signs outlined in Table 1 would alert the practitioner to this.24,25 Patients presenting with infective complications, as outlined above, will be clinically very unwell and more inclined to contact their medical rather than dental practitioner. However, peri-orbital oedema from acute bacterial infections of the ethmoids and maxillary sinus can be similar to that arising from a maxillary canine or lateral incisor tooth, and for that reason patients may occasionally contact their dental rather than medical practitioner.
Reduced visual acuity
Proptosis
Ophthalmoplegia
Peri-orbital oedema
Diplopia
Intense frontal headache
Frontal bone swelling
Altered consciousness or behaviour
Focal neurological signs (of cranial nerves or hemiplegia)
Seizures
Chronic sinusitis is defined as a symptom of nasal obstruction, facial pressure or full purulent nasal discharge, and hyposmia and occasionally anosmia lasting for 12 or more weeks.17 It is usually of bacterial or fungal aetiology, although can also occur as a result of the immune system response to fungal spores (fungal allergy). Chronic rhinosinal disease is classified by either the absence or presence of polypoid tissue and there are specific treatment guidelines for each.17 Polypoid tissue arises because of the immunological response of the nasal mucosa to irritants. Most polyps arise in the ethmoid sinuses, with a smaller proportion, usually antro-choanal, arising in the maxillary sinus.26
Orofacial pain, including odontogenic pain and headache, is rarely a feature of chronic sinusitis except during rare acute exacerbations of chronic sinus infection.27
Recurrent acute rhinosinal disease
Recurrent acute rhinosinal disease is classified as four or more episodes of nasal obstruction, purulent nasal discharge, with facial pain or pressure-like symptoms per year.17 Recurrent acute sinusitis is generally regarded as being an exacerbation of chronic rhinosinal disease.
Recurrent acute rhinosinal infection can occur in the presence of disease-modifying factors, such as asthma, cystic fibrosis, ciliary dyskinesia, or immune deficiency states. A patient presenting with recurrent infection without an obvious predisposing cause should be investigated further.17
Recurrent acute rhinosinal disease presents as a significant healthcare burden in developed countries with multiple work days lost and repeat prescriptions of antibiotics given,28 hence multiple guidelines have been developed to assist the practitioner in making an accurate diagnosis.17,18,22,29 There is now increasing doubt as to the real prevalence of recurrent infective acute rhinosinal disease, as there is considerable overlap of symptoms with primary headache syndromes and orofacial pain.30,31,32 In addition, there is an increased prevalence of self-reported rhinosinal symptoms in patients presenting with generalized fatigue, chronic pain syndromes, non-specific gastrointestinal symptoms, and musculo-skeletal pain, suggestive that some cases of recurrent rhinosinal symptoms are of a functional rather than organic nature.33,34,35,36,37
Establishing an accurate diagnosis
With the aim of improving diagnosis, guidelines recommend that, in addition to the recognized descriptive criteria for rhinosinal disease outlined in Table 2, for a diagnosis of rhinosinal disease there should also be:
Direct anterior rhinological endoscopic examination of the middle meatus to determine if pus, inflammatory mucosal changes with or without polyps is identifiable;29 and/or
Cross-sectional imaging, usually computed tomography of the paranasal sinuses.29
Inflammation of nasal mucosa characterized by one or more symptoms which should be:
1. Nasal obstruction or congestion
2. Nasal discharge with either anterior or posterior nasal drip
Additional criteria may include:
1. Facial pain or pressure-like sensation
2. Partial or complete loss of smell
These specialist examinations should only be undertaken in a specialist setting by an Ear Nose and Throat (ENT) surgeon. Cross-sectional imaging, even in the specialist setting, is generally reserved for cases of unilateral chronic pain, or when there are symptoms or signs suggestive of a sinister disease process.17,38
Detailed description of clinical findings upon anterior rhinoscopy is beyond the scope of this paper, but is well outlined in ENT texts.39 Computed tomography of the paranasal sinuses is performed to determine the presence or absence of any signs of disease, including inflammation within the paranasal sinuses or adjacent tissues. Computed tomography is also used to determine the patency of the osteo-meatal complex, where both the ethmoid and maxillary sinuses drain into the nasal cavity40 (Figure 1).
The surgical management of chronic rhinosinal disease is also beyond the scope of this paper but interested readers are directed to ENT texts.41
Non rhinosinal causes for facial pain, headache and dental pain
Patients with acute or chronic rhinosinal disease do not necessarily have headache or orofacial pain. This is demonstrated by the following observations:
Over 80% of patients observed to have pus in the middle meatus upon anterior rhinoscopy have no symptoms of pain;42
Most patients with polyps in the middle meatus do not experience pain;43
A proportion of patients that undergo surgical procedures for chronic rhinosinal disease after failed medical management continue to experience pain post-operatively;42
Up to 50% of patients having facial radiographs taken for purposes other than investigation of rhinosinal disease demonstrated mucosal thickening without symptoms;44
Significant mucosal abnormalities of the paranasal sinuses are identified on CT and MR imaging performed for reasons other than investigation of rhinosinal disease in patients that have no symptoms.45
Therefore, even if criteria for a diagnosis of rhinosinal disease are fulfilled, it does not necessarily follow that their pain is solely attributable to paranasal sinus infection. It has been suggested that removing the symptom of pain or pressure-like symptoms from the diagnostic criteria allows for greater specificity and sensitivity when making a diagnosis of chronic rhinosinal disease.46
At this stage, the criteria on which a diagnosis of headache or orofacial pain was based needs to be re-considered, which in turn takes the clinician back to the history of patient symptoms and the wider differential diagnosis of orofacial pain and headaches.
Primary headaches: migraine with autonomic symptoms
The International Classification of Headache Disorders recognizes that rhinosinal disease and primary headaches can co-exist in the same patient and have variable contribution to patient symptoms.47 The International Headache Society also recognizes that secondary headaches as a result of acute rhinosinal disease are relatively rare.47
It is now acknowledged that many patients with unilateral facial pain or a headache that present in the area of the paranasal sinuses have migrainous type headaches which can occur with or without an aura.32,47,48 Migraine can occur as mid-facial pressure without headache, termed a typical aura without headache.32,47 The clinical picture is blurred even further when it is recognized that some migraine-type headaches can be bilateral.49 Parasympathetic stimulus to the sino-nasal mucosa during a migraine may cause oedema of nasal soft tissue, and increase nasal secretions, although the secretions would not be purulent.50 The parasympathetic stimulus will therefore mimic the symptoms stated by clinical guidelines as being indicative of rhinosinal disease. It would only be upon examination by an ENT surgeon that polypoid disease or purulent discharge in the middle meatus could be excluded.
There is therefore a risk that patients complaining of chronic or recurrent facial pain and headaches, with nasal discharge or congestion, may fulfil the criteria outlined for diagnosis of chronic or recurrent rhinosinal disease and be started on an incorrect treatment pathway when they have a primary headache disorder.
There is evidence that patients with facial pain or a headache without purulent nasal discharge respond well to triptan medication.51 However, the clinical picture is further blurred when it is recognized that some patients can also experience migraines at the same time as having symptoms related to chronic rhinosinal disease.47,52
The trigeminal autonomic cephalgias, recognized as primary headache syndromes by the International Headache Society, produce pain but, because of parasympathetic activity, also cause nasal congestion and nasal discharge, in addition to lacrimation, flushing of skin, conjunctival injection, eyelid oedema and ptosis.47 Recurrent attacks of facial pain and headaches, caused by any of the trigeminal autonomic cephalgias outlined in Table 3, can be mistakenly diagnosed as recurrent acute rhinosinal disease. It is not possible to discuss trigeminal autonomic cephalgias in detail in this paper but interested readers are referred to a further text.53
Cluster headache
Paroxysmal hemicrania
SUNCT (short lasting neuralgiform headaches with conjunctival injection and tearing)
SUNA (short lasting neuralgiform headaches with autonomic symptoms)
Hemicrania continua
Trigeminal neuralgia
Although it would be unusual for trigeminal neuralgia to be mistakenly diagnosed as recurrent rhinosinal disease, it has been reported.42 Trigeminal neuralgia has, on most occasions, a very characteristic unilateral presentation and is not usually associated with any autonomic symptoms that may cause nasal obstruction or discharge. However, the careful clinician would consider this as part of a broader possible diagnosis in cases where the clinical picture is not clear.54
Temporomandibular disorders: confusion with rhinosinal disease
The clinician may experience diagnostic difficulties when the patient describes unilateral or bilateral facial pain, with zygomatic/temporal or retro-orbital radiation, especially when the patient may describe many years of facial pain and headache attributable to sinus disease. The problem is even more challenging when other primary care practitioners have reinforced the incorrect diagnosis of rhinosinal disease by multiple antibiotic prescriptions.
The diagnostic criteria for acute or chronic rhinosinal disease do not overlap with the diagnostic criteria for temporomandibular disorder (TMD).55
Careful history-taking from a patient will determine whether or not there is a history of nasal congestion, nasal discharge, loss or reduction of smell. Careful examination, as outlined in the diagnostic criteria for the most common pain-related temporomandibular disorders, should guide the clinician towards an accurate diagnosis.55
Atypical facial pain or tension type headache
In the absence of any specific patient symptoms or clinical signs that would suggest a specific disease process, the diagnosis of atypical facial pain or tension type headache should be considered. Research has demonstrated that non-specific, mid-facial pain was caused by atypical facial pain, TMD and tension type headaches as frequently as migraines or trigeminal autonomic cephalgias.42
Contact point headaches
There are multiple contributions to the literature that aim to demonstrate that various points of contact between the medial and lateral nasal walls, including contact of some of the turbinates with either the medial or lateral nasal walls, will contribute to areas of mucosal pressure and cause headaches.56 Such contact points are observed on CT scanning.
While this topic has been explored with vigour in the literature, there is a paucity of reliable evidence to support this concept. Mucosal contact points have been demonstrated in patients with and without symptoms of pain.57 The concept risks exposing patients to unnecessary radiation, and also unnecessary surgery that will not provide long-term control of symptoms.
Acute maxillary sinus pain or odontogenic pain
The dental surgeon can be presented with a patient complaining of acute onset unilateral maxillary pain. As for chronic or recurrent facial pain and headache, the importance of a comprehensive history of symptoms cannot be under-estimated.
Clinical and radiological examination as outlined in Table 4 will guide the dental surgeon through the diagnostic process of symptoms and signs that are specific to acute infection of the maxillary sinus or specific to odontogenic disease. Some symptoms and signs will be shared. Accurate diagnosis will not be made on one sign or symptom but rather a combination of both.27
Specific Sinogenic
Shared Sinus and Odontogenic
Specific Odontogenic
Unilateral nasal obstruction
Increased pain with changes in atmospheric pressure (barodontalgia)
Increased pain upon thermal stimuli when eating or drinking
Unilateral nasal discharge
Unilateral maxillary pain
Obvious caries, or fracture of tooth
Concurrent or recent upper respiratory tract infection
Disturbed sleep
Buccal or palatal swelling directly adjacent to source of pain
Increased pain on change in vertical position of head
Facial swelling (Rare cases of acute ethmoid or frontal sinus infection)
Specific radiological signs
Pus in middle meatus (Specialist setting only)
Buccal sulcus swelling (Will occur when maxillary sinus very large with thin lateral wall)
Tooth mobility
Heavily restored tooth
Inflamed or polypoid tissue in middle meatus
Vertically fractured tooth
Polarized light transillumination
Pain upon biting upon a specific cusp
A periapical radiograph is the image of choice for diagnosis. A sectional dental panoramic tomogram (DPT) may be used if the patient cannot cope with a film holder. Radiological signs suggestive of apical periodontitis are; widening of periodontal ligament space, loss of lamina dura around apices, apical radioluency. Condensing apical periodontitis is a sign rarely observed in the posterior maxilla. Gross or extensive secondary caries are obvious signs suggestive of pulpal necrosis.
There is no role for the use of Cone Beam Computed Tomography as a first line radiographic investigation in the diagnosis of acute or chronic orofacial pain.17,27,58
In the same context that guidelines exist to enable accurate diagnosis of chronic or recurrent rhinosinal disease, in an effort to avoid unnecessary antibiotic prescription or surgery, an accurate diagnosis of unilateral maxillary alveolar or facial pain will hopefully avoid unnecessary dental treatment.
Summary
This paper has discussed the diagnostic criteria required for a diagnosis of either acute or chronic rhinosinal disease, to give the dental surgeon greater confidence in making a diagnosis. The potential for misdiagnosis of recurrent or chronic orofacial, mid-facial pain, with or without headaches, has been emphasized.
It is recommended that the dental surgeon who is unable to provide a reliable diagnosis for mid-facial pain or headache should refer to the patient's medical practitioner, or a secondary care oral medicine/oral surgery/maxillofacial surgery service.
The practice of prescribing antibiotics in the presence of pain but absence of specific signs of spreading infection or pyrexia is discouraged.
It has not been possible for this paper to provide an outline of all paranasal sinus disease with a broad pathogenic basis. This is covered in more detail in other texts.1,7,9,27,39,40
The following three papers will outline how dental care may impact on the health, function and ultimately disease of the maxillary sinus. In the next paper the removal of teeth that are closely related to the maxillary sinus, and the possible complications that may arise, will be discussed.