Knowledge of structures of the head and neck is an important aspect of safe and effective daily clinical practice. This article will review the relevant anatomy for the assessment of the temporomandibular joints (TMJs) and associated structures, delivery of local anaesthesia, understanding routes of spread of odontogenic infections and avoidance of anatomical complications in dento-alveolar surgery.
CPD/Clinical Relevance: To recap key clinically relevant basics of head and neck anatomy.
Article
Rana Wali
The Temporomandibular Joint (TMJ)
The TMJ is the articulation between the squamous portion of the temporal bone and the mandibular condyle. The articular surfaces of the temporal bone and the condyle are completely enclosed within a dense fibrous capsule. Interposed between the articular surfaces of the temporal bone and mandibular condyle, and contained within the capsule is an intra-articular disc. The capsule attaches to the articular eminence, the circumference of the articular disc and to the neck of the condyle. It has various sensory receptors including nociceptors, and blends with the temporomandibular (lateral) ligament. The articular disc divides the TMJ into superior and inferior compartments (Figure 1). The surfaces of these compartments contain a lining which produces a synovial fluid, thus making the TMJ a synovial joint.
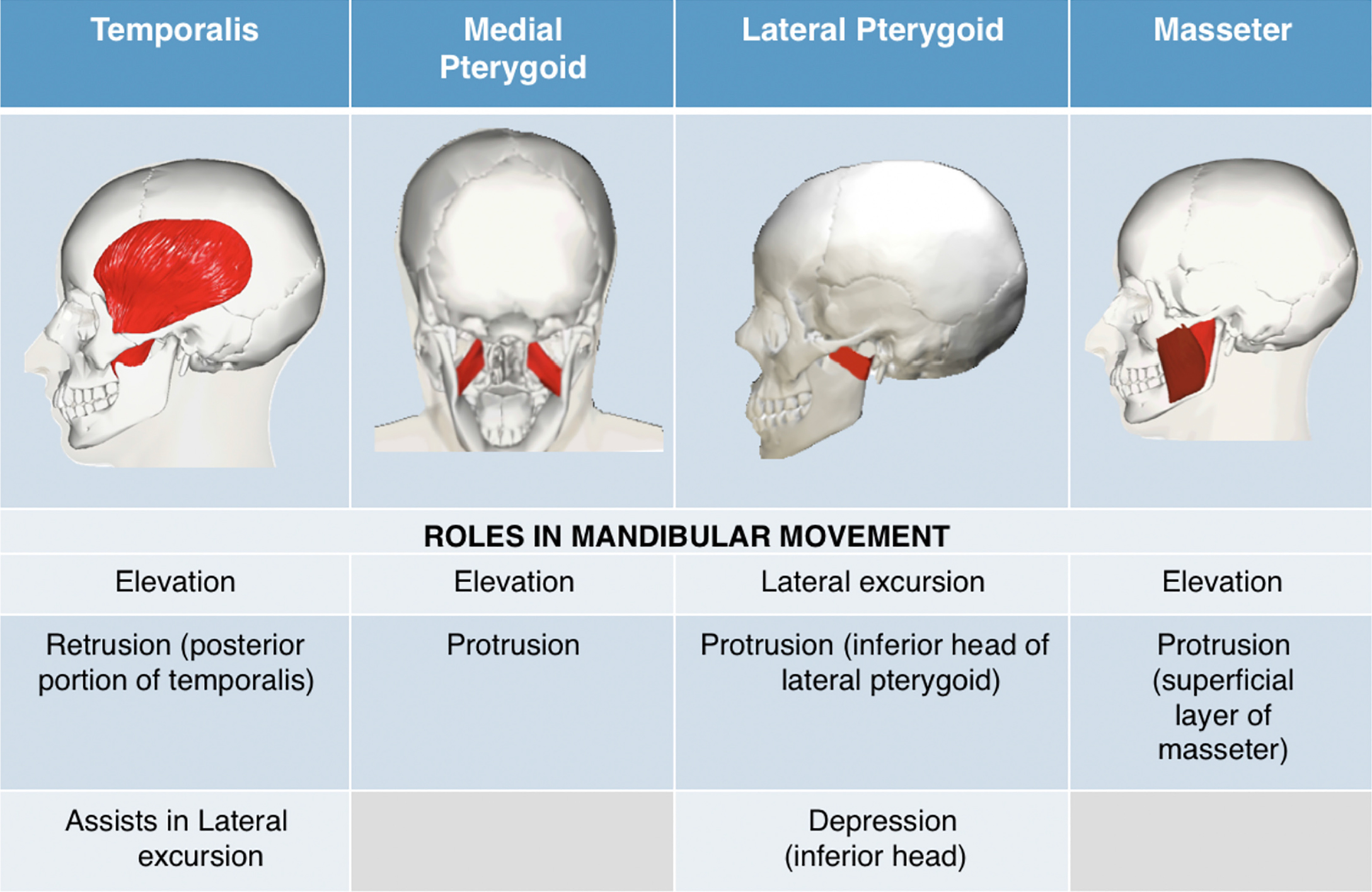
Figure 1 Primary muscles of mastication and their roles in mandibular movement.
Pain on palpation of the immediate pre-auricular area suggests inflammation of the capsule (capsulitis). This may be due to several reasons, such as major trauma eg assault, or minor trauma eg parafunction. A thorough patient history will aid in identification of the relevant cause and guide management.
The superior compartment provides the translational movement of the TMJ whilst the inferior compartment provides rotational movement. The first 20 mm of opening is pure rotational movement; further opening is achieved by translational movement where the articular disc and condyle complex slide inferiorly on the articular eminence.
The articular disc has muscle attachments anteriorly but only elastic fibres posteriorly. This is why anterior disc displacement is common; spasming of the lateral pterygoid muscle pulls the articular disc forward, with no posterior muscles to counteract this movement.
There are 12 different muscles involved in mandibular movement. They are classified as primary and secondary/accessory. The four primary muscles associated with mandibular movement, and their roles in mastication are presented in Figure 1. The secondary muscles are anatomically classified as infra-hyoid and supra-hyoid muscles; they are beyond the scope of this article and are not discussed here.
Examination of the primary muscles of mastication is helpful in guiding diagnosis and management. The lateral pterygoid muscle is the only muscle in intimate contact with the articular disc; however, it is not accessible to manual palpation. The resistance-response test is a more reliable means of testing this muscle and is performed by the clinician by placing a hand under the patient's chin and asking the patient to open his/her mouth, and to make jaw movements against resistance.1 Pain will be felt in the ear of the affected side due to inflammation of the pterygoid muscle. The masseter muscle is often tender in patients who clench their teeth, whilst the temporalis muscle is more commonly tender in patients with bruxism.
An understanding of the anatomy not only aids clinical examination and diagnosis, but plays an important role in communicating conditions such as Temporomandibular Disorder (TMD) to patients. In some cases, TMD may occur as a chronic condition, whereby achieving patient understanding is key to management. The use of skull models and a jargon-free description of the anatomy can be helpful in explaining the condition.
Local anaesthesia
Successful delivery of local anaesthesia is essential to provide pain-free treatment to patients. An understanding of the different techniques available relies on knowledge of local anatomy.
Mandibular anaesthesia
Inferior Alveolar Nerve Block (IANB) and lingual nerve block
The purpose of an IANB is to anaesthetize:
All the mandibular dentition;
The epithelium of the anterior two-thirds of the tongue (lingual nerve);
All of the lingual gingiva and mucosa (lingual nerve);
All of the buccal gingiva, and mucosa from the premolar region to the midline (mental nerve);
The skin of the lower lip (mental nerve).
Anaesthetic solution is deposited into the pterygomandibular space at the region of the mandibular foramen. Adequate anaesthesia of the inferior alveolar nerve (as well as its mental and incisive branches) and the ingual nerve requires accurate needle angulation and penetration into the pterygomandibular space.
Method
The mandibular foramen is located approximately midway between the anterior and posterior border of the ramus. These landmarks can be palpated intra-orally and extra-orally.
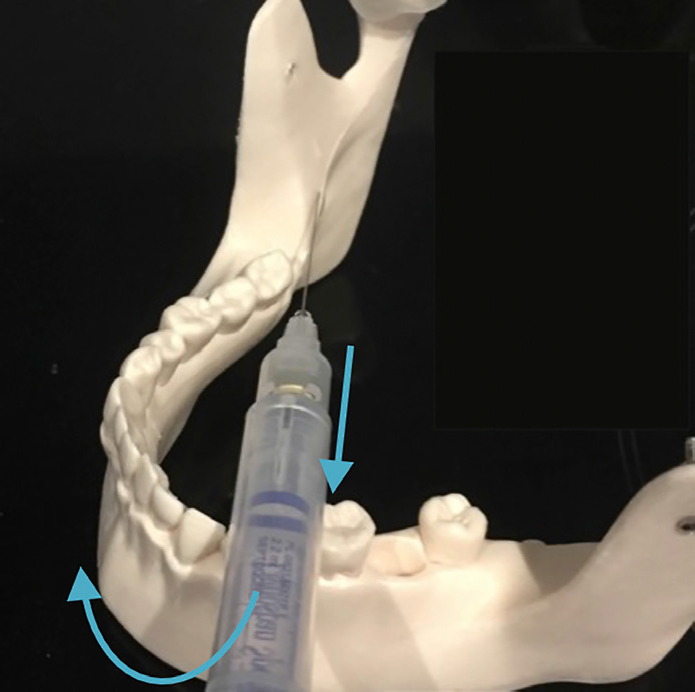
The needle is oriented from the contralateral premolars and inserted between the coronoid notch and the pterygomandibular raphe (Figure 2).
Figure 2. Needle positioning for delivery of an IANB.
Contact with bone is usually achieved after inserting the needle to approximately 20–25 mm.2 If contact is immediate, the needle should be re-oriented posteriorly. The needle should be retracted and redirected medially until parallel with the line of the arch.
Aspiration should be performed to determine if the needle is within a blood vessel and only after a negative result (no blood in the syringe), should the anaesthetic solution be deposited.
Considerations
If the needle is not advanced far enough into the pterygomandibular space, adequate anaesthesia will not be achieved.
If advanced too far, the parotid capsule may be pierced by the needle and local anaesthetic will enter the parotid gland, spreading to the branches of the facial nerve. This can result in transient facial palsy.
Variations of the IANB3
Gow-Gates Block
This is useful for multiple procedures of the mandibular teeth and the buccal soft tissues. It involves contact of the needle with the neck of the mandibular condyle, providing anaesthesia to the regions innervated by:
IAN and its branches;
Mylohyoid nerve;
Lingual nerve;
Long buccal nerve;
Auriculo-temporal nerve.
The mouth is opened as wide as possible and the needle is inserted into the buccal mucosa at the level of the second maxillary molar. The needle is advanced from the corner of the mouth and directed towards the inter-tragal notch until the needle contacts the neck of the condyle (Figure 3).
Figure 3. Gow-Gates block.
Akinosi Block
This technique is used for patients with limited mouth opening where the standard IANB technique is challenging. It uses a closed mouth approach, anaesthetizing the:
IAN and its branches;
Mylohyoid nerve;
Lingual nerve.
With the mouth closed, the needle is inserted into the mucosa between the medial border of the ramus and the maxillary tuberosity. The needle is advanced parallel to the maxillary occlusal plane at a distance of 23–25 mm. No bone will be contacted and the needle will be inserted into the pterygomandibular space (Figure 4).
Figure 4. Akinosi block; a closed mouth approach.
Mental nerve block
A mental nerve block provides anaesthesia of the buccal gingiva and mucosa from the premolar region to the midline, and to the skin of the lower lip.
Radiographic imaging and intra-oral palpation can help locate the mental foramen.
The needle is inserted a short distance into the mucobuccal fold between the first and second premolars (Figure 5).
Figure 5. Mental nerve block.
Long buccal nerve block
The long buccal nerve is a branch of the anterior division of the mandibular nerve. A long buccal nerve block is performed to anaesthetize all buccal gingivae adjacent to the mandibular molars. The needle is inserted at a distance of about 2 mm into the mucosa posterior to the last molar in the arch (Figure 6).
Figure 6. Long buccal nerve block.
Maxillary anaesthesia
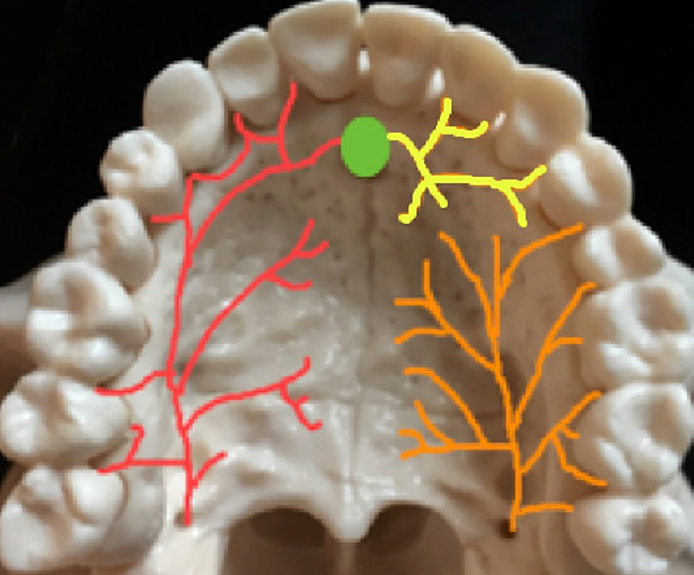
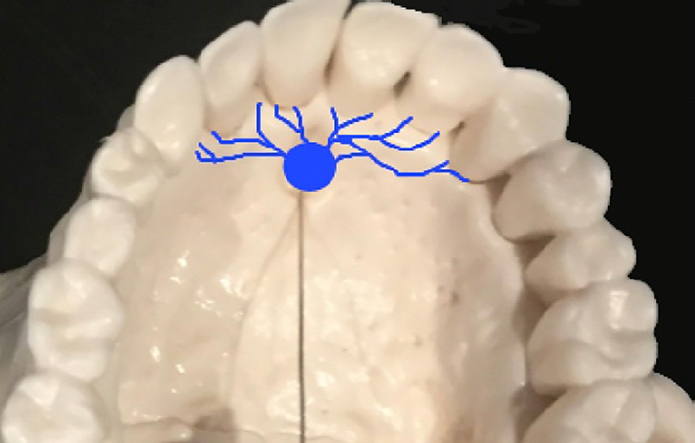
The hard palate and palatal aspect of the maxillary dentition are supplied by the nasopalatine and greater palatine nerves (Figure 7).
This can be particularly painful for patients as the mucosa is tightly adhered to the hard palate. It achieves anaesthesia of the palatal region between the maxillary canines. The needle is inserted lateral to the incisive papilla, then advanced until it contacts bone (Figure 8). Pressure applied to the area, eg with a cotton swab, or using the handle of the dental mirror, can help reduce the pain. Deposition of a small amount of the anaesthetic on initial penetration of the mucosa can also reduce the pain felt during advancement of the needle to the hard palate.
Figure 8. Nasopalatine nerve block.
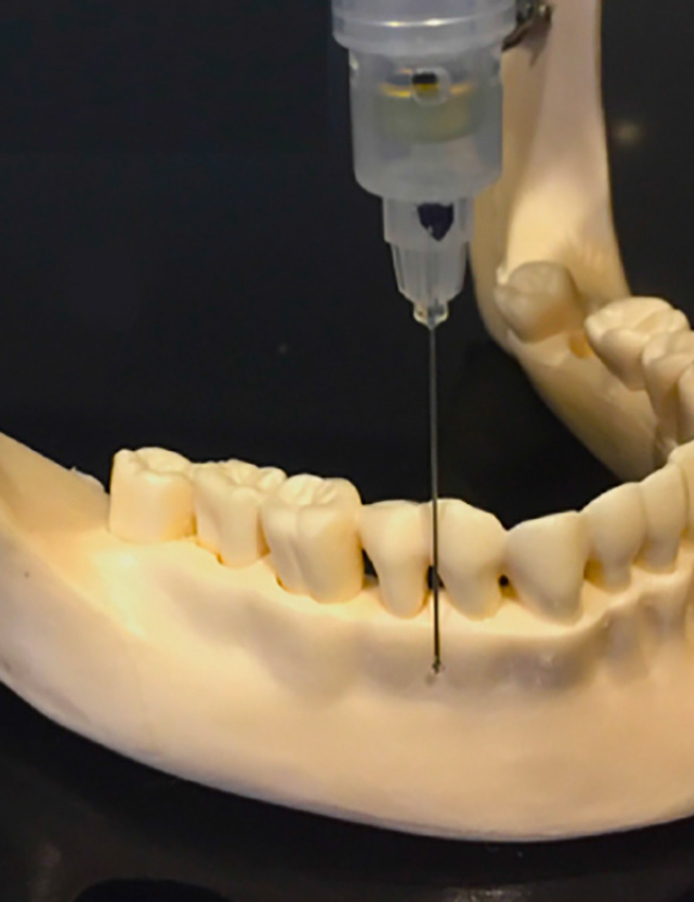
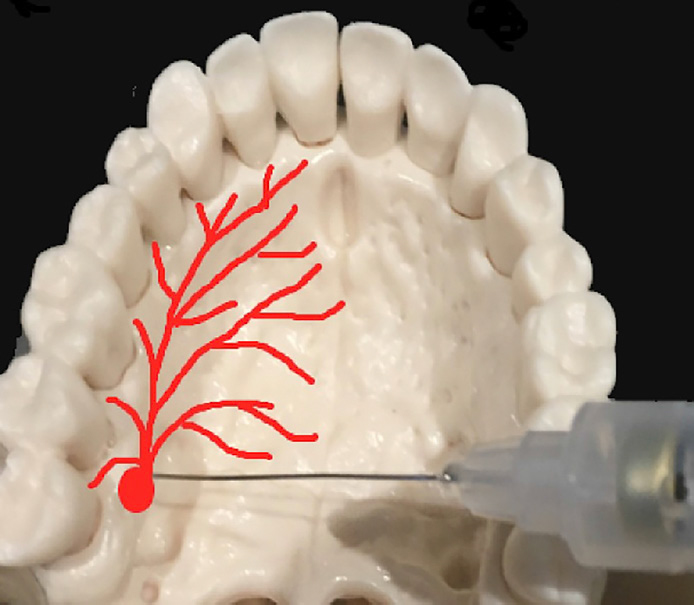
Greater palatine nerve block
This provides anaesthesia to the palatal mucosa from the first premolar to the posterior hard palate. The needle is inserted posterior to the second maxillary molar into the more spongy mucosa. This is often the landmark for the greater palatine foramen (Figure 9). A small amount of anaesthetic solution is deposited before advancing the needle until it contacts the bone. Failure to feel the underlying bone suggests that the needle may be positioned too far posteriorly in the soft palate.
Figure 9. Greater palatine nerve block.
Superior alveolar nerve block
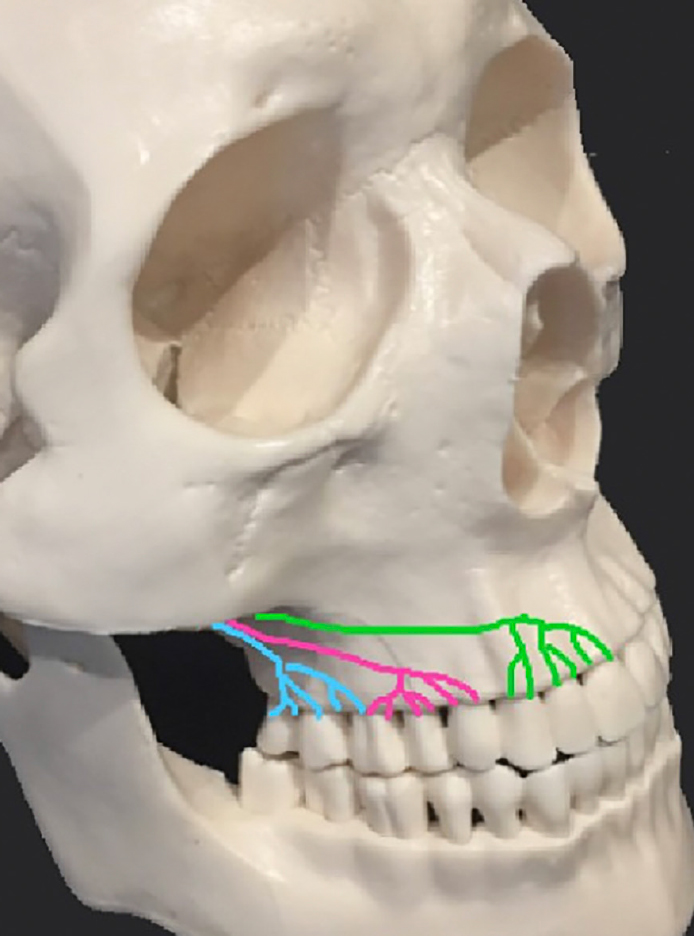
The buccal aspect of the maxillary dentition is supplied by the anterior, middle and posterior superior alveolar nerves (Figure 10).
Figure 10. Posterior superior alveolar nerve (blue); middle superior alveolar nerve (pink); anterior superior alveolar nerve (green).
Posterior superior alveolar nerve block
This block anaesthetizes all the maxillary buccal gingivae and maxillary molars, except the mesiobuccal root of the first maxillary molar. The needle is inserted into the mucosa at the muco-buccal fold, superior to the maxillary second molar and aiming at the infratemporal fossa. This requires advancement of the needle approximately 15 mm along the posterior surface of the maxilla. Short needles are safer to avoid the risk of haematoma.
Middle superior alveolar nerve block
This nerve is reported to be present in up to 72% of patients.3,4 This type of block provides anaesthesia to the maxillary premolars and the mesiobuccal root of the first maxillary molar, as well as the buccal gingivae of these teeth. The needle is placed into the mucobuccal fold superior to the maxillary second premolar and the tip is aimed just superior to the apex of this tooth. The benefit of this form of block is the relative avascular nature of the region, reducing the likelihood of haematoma formation compared to a local infiltration.
Anterior superior alveolar nerve block/infra-orbital block
This block is used to anaesthetize the ipsilateral maxillary canine, lateral and central incisors, as well as the alveolus and buccal gingivae. The patient should be warned that the lower eyelid, lateral aspect of the nasal skin tissue and infra-orbital skin region will also be anaesthetized. The infra-orbital foramen is palpated extra-orally and the needle is inserted into the muco-buccal fold above the apex of the maxillary canine. Bone should be contacted at the region of the infra-orbital foramen.
Summary of local anaesthetic considerations
It is important to remember that there are many anatomical variations amongst patients. Visualization and palpation of landmarks is important to help increase the reliability of delivery of local anaeshetic.
Odontogenic infections
Orofacial tissue spaces are potential spaces between fascial layers that offer anatomical routes for infections to spread from superficial to deep planes. Infections spread via the path of least resistance and into the fascial spaces.
Mandibular spread of infection
The potential primary routes of spread of infection from a mandibular molar are determined by the local anatomy and muscle attachments.
Mylohyoid muscle
If the infection drains above the origin of mylohyoid muscle, the infection is in the sublingual space;
If the infection drains below the origin of the mylohyoid muscle, the infection is in the submandibular space.
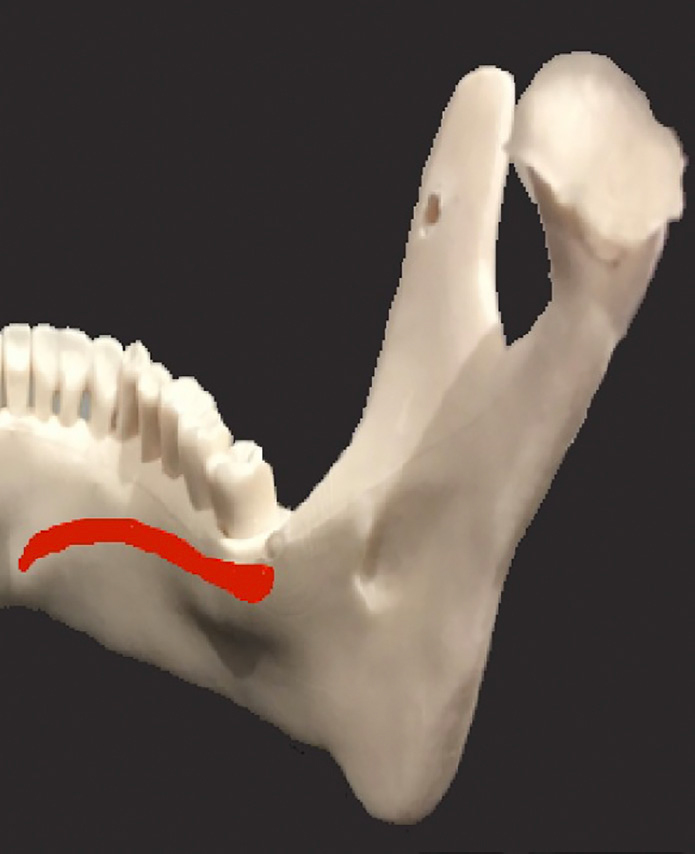
Figure 11 shows how the attachment of the mylohyoid muscle slopes downwards as it passes medially. Therefore, an abscess from a posterior tooth that drains apically is more likely to spread below the attachment of the mylohyoid muscle, and into the submandibular space. Further anteriorly, in the premolar region, infections are more likely to drain above the attachment of the mylohyoid muscle and therefore drain into the sublingual space.
Figure 11. Attachment of the mylohyoid muscle.
It is important to note that since muscle fibres are permeable, infection can spread between the spaces, especially in the case of highly virulent infections.
Buccinator muscle
If the infection drains above the origin of the buccinator muscle, the infection will present in the buccal sulcus;
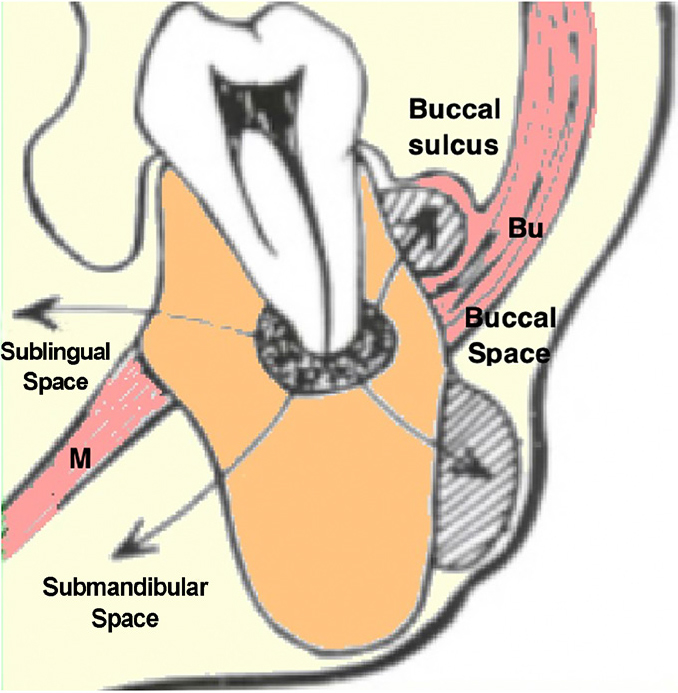
If the infection drains below the origin of the buccinator muscle, the swelling will occur in the buccal space and appears as a facial swelling (Figure 12).
Figure 12. Spread of infection from a lower molar, M = Mylohyoid muscle, Bu = Buccinator muscle.
Mentalis muscle
Infection draining below the origin of the mentalis muscle can appear as an extra-oral sinus or fistula on the chin. This recurs if the cause has not been established and treated. It is important to consider a dental origin when a patient presents with a recurrent draining sinus on the chin.
Superior constrictor muscle
Infection in the plane between the superior constrictor muscle and the submucosa of the pharyngeal wall is peri-tonsillar. If the infection drains external to the superior constrictor muscle, it will present in the parapharyngeal space.
Infection in these spaces will cause difficulty swallowing or breathing. Examination of the uvula is an important aid to airway assessment and deviation may indicate a compromised airway and prompt efficient management.
Medial pterygoid and masseter muscles
Infection present in the plane between the medial pterygoid muscle and the mandibular ramus is, by definition, in the pterygomandibular space. Infection in the plane between the masseter muscle and the ramus is said to be in the submasseteric space. Infection in either the pterygomandibular or submasseteric spaces will manifest as trismus. Often, these patients will not present with an extra-oral swelling and therefore thorough clinical examination is crucial for diagnosis and appropriate emergency management.
Within the neck, there are no horizontal barriers and therefore there is potential for infection to spread down into the neck. Fascial planes and gravity can facilitate spread of infection into neck spaces, which is increased among immunocompromised patients.
Maxillary spread of infection
Infections of the canine can spread in an upward direction due to the local muscles funnelling the infection upwards and towards the eye. The cavernous sinus is a cavity at the base of the brain which drains deoxygenated (venous) blood from the brain. Cavernous sinus thrombosis (CST) is a life-threatening complication that may result from infection spreading from the maxillary anterior dentition. Gross oedema of the eyelid, limited eye movements and exophthalmos are clinical signs of this condition and should be treated as an emergency with vigorous and early use of IV antibiotics, drainage and elimination of the source of the infection.
Infection in the maxillary arch that drains:
Above the buccinator muscle, causes swelling in the buccal space;
Below the origin of the bucccinator, causes swelling in the buccal sulcus.
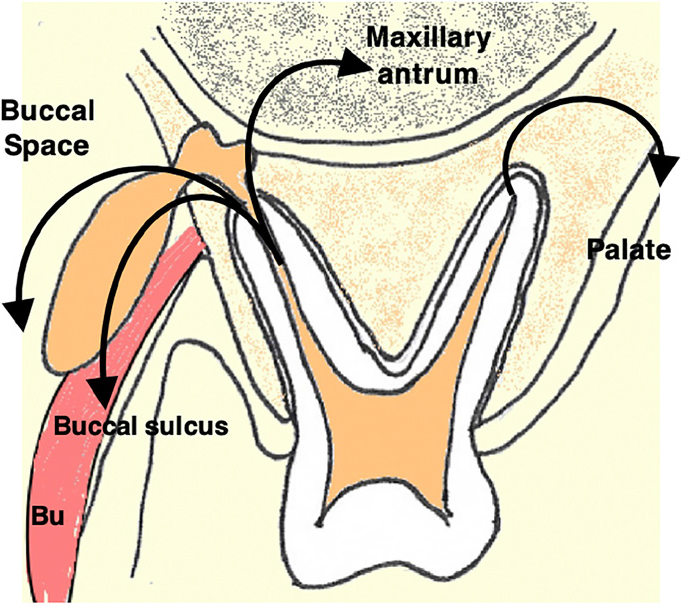
Other spaces into which maxillary odontogenic infections can spread include the palate and maxillary antrum (Figure 13).
Figure 13. Spread of infection from an upper molar, Bu = Buccinator muscle.
Ludwig's angina
Ludwig's angina occurs when there are concurrent bilateral sublingual, submandibular and sub-mental space infections. It is a potentially life-threatening infection and patients must be referred immediately to hospital for drainage of the infection and administration of intravenous antibiotics. Patients may present with pyrexia, dysphagia, dysarthria, dyspnoea and a raised floor of mouth.
A sound understanding of the anatomy of the fascial spaces can help in the diagnosis of a spreading infection and prevent delay in management.
Dento-alveolar surgery and its related complications
Preservation of vital structures is a basic principle of flap design. Careful planning and anatomical consideration must be undertaken before proceeding with a surgical procedure.
Maxilla
Greater palatine nerve
The greater palatine nerve emerges through the greater palatine foramen onto the hard palate (Figure 9). It supplies the palatal mucous membrane from the posterior teeth anterior to the canine region and the associated glands of the palate. The greater palatine artery runs alongside the corresponding nerve and provides vasculature to the hard palate. In considering these vital structures, it is important to avoid vertical relieving incisions in the palate. Where adequate access requires a vertical receiving incision, this should be made anteriorly to prevent bleeding caused by severing the greater palatine artery.
Nasopalatine nerve
The incisive region of the hard palate is innervated by this nerve which emerges onto the hard palate through the incisive fossa (Figure 8). An envelope flap in this region should ideally be sufficient to prevent damage to the nerve. However, as the area of mucosa supplied by this nerve is very small, any temporary or permanent anaesthesia caused by a relieving incision is rarely problematic for the patient.
Mandible
When planning dento-alveolar surgery in the mandible, the following structures should be considered:
Inferior alveolar nerve (IAN);
Mental nerve;
Lingual nerve.
Inferior alveolar nerve (IAN)
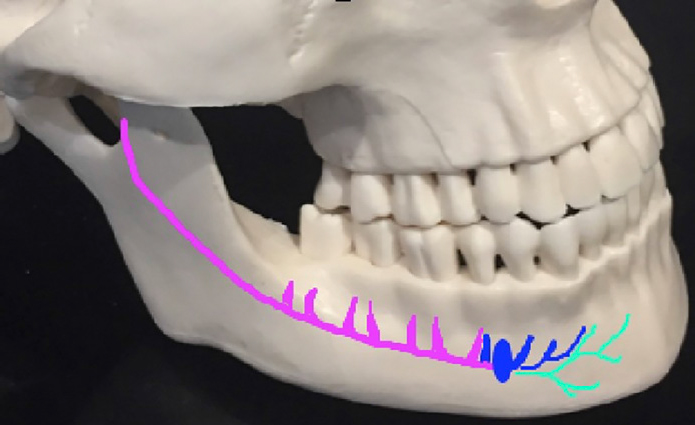
This nerve enters the mandible through the mandibular foramen and continues in the mandibular canal where it gives off branches to the mandibular molars and premolars (Figure 14).
The mental nerve – sensory to the chin and lower lip;
The incisive nerve – sensory to the mandibular anterior teeth and labial gingiva. When planning for dento-alveolar surgery in the posterior mandible, it is important to determine the risk of damage to the IAN (Figure 15). Radiographic assessment involves identifying high risk signs such as those listed in Table 1.5 Presence of these signs may warrant further imaging, for instance, a Cone beam CT scan to determine the risk and to plan treatment.
Figure 15. Radiographic assessment of the lower right 3rd molar in relation to the IAN.
Root signs
Canal signs
Darkening
Loss of cortication
Deflection
Diversion
Narrowing
Narrowing
Patients should be informed of the risk of temporary or permanent altered sensation to the lip, chin and tongue. Since this nerve is encased within the mandibular canal in the body of the mandible, there is no risk to this nerve when considering soft tissue management during flap design.6
Mental nerve
The common locations for the mental foramen are:
In the interdental space between the apices of the lower first and second premolars;
Apical to the second premolar.
The literature is divided in opinion regarding the most common location of the mental nerve.7 It is therefore essential to have a radiographic image prior to planning a surgical procedure involving this part of the mandible.
Due consideration should be given to this nerve when planning soft tissue management during the surgical process. The main risk is from an incision that may cause a crush injury to the nerve, as well as from excessive pressure during flap retraction.
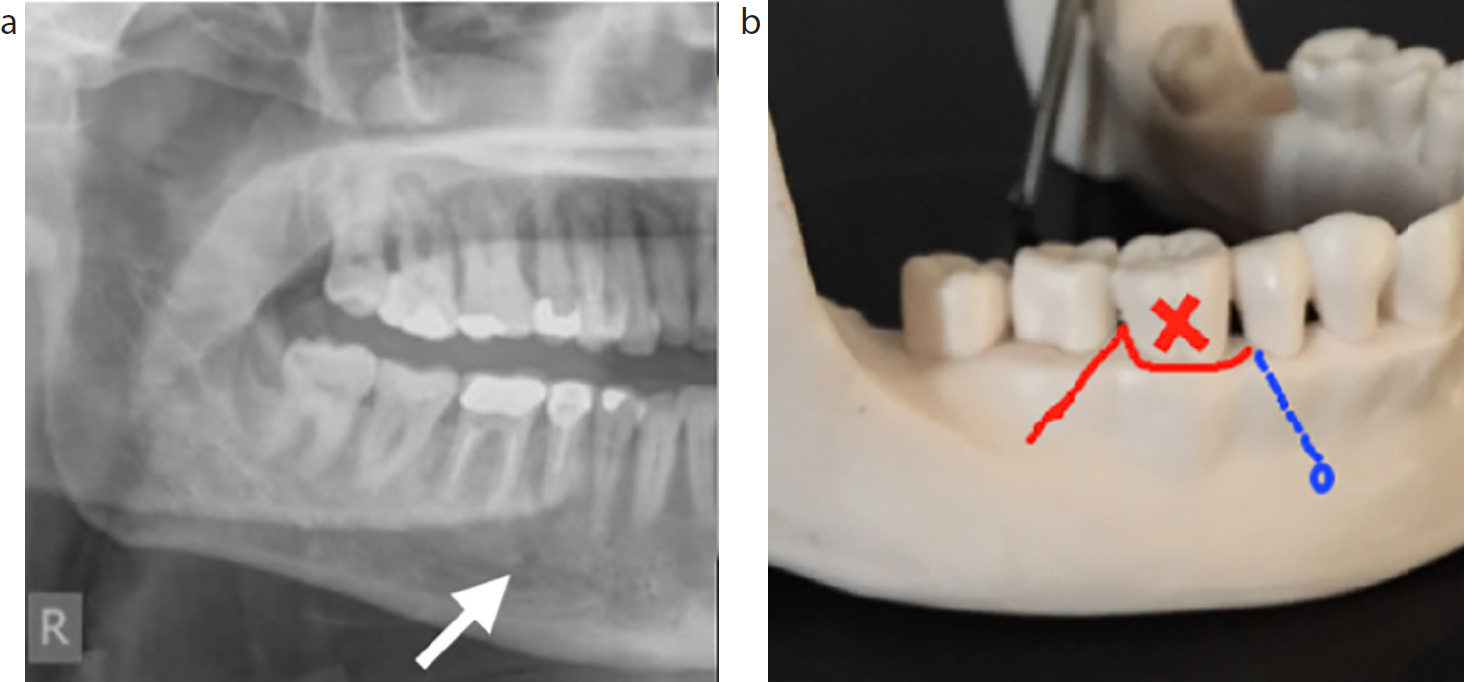
Figure 16 demonstrates the importance of considering the mental nerve when planning the flap design for removal of a lower first molar.
Figure 16. (a, b) The importance of considering the mental nerve when planning the flap design for removal of a lower first molar.
Lingual nerve
The lingual nerve runs between the medial pterygoid muscle and the mandible. The lingual nerve is joined by the chorda tympani and together they enter the posterior aspect of the oral cavity and run forwards. The lingual nerve enters the floor of the mouth and ventral surface of the tongue supplying sensation to the tongue, floor of mouth and lingual mucosa of the mandibular arch.
In the third molar region, this nerve is covered only by a thin layer of mucosa. For this reason, surgery should be performed via a buccal approach with no lingual bone removal. Care must be taken not to perforate the lingual cortex when sectioning mandibular teeth and lingual retraction should be avoided. In some surgical cases, lingual retraction may be required and should be carefully carried out by experienced clinicians.
Discussion
Sound knowledge of head and neck anatomy is essential for many common clinical encounters in both the primary and secondary healthcare settings. Awareness of key head and neck structures aids in planning investigations, determining diagnosis, surgical planning, delivery of treatment, patient education, and prevention and management of complications.
Clinicians should regularly review their knowledge of head and neck anatomy which has significant implications for daily general clinical practice.