DipRestDent, StR in Restorative Dentistry, Department of Restorative Dentistry, Liverpool University Dental Hospital, Pembroke Place, Liverpool, Merseyside L3 5PS
For patients presenting with more severe forms of tooth wear, removable dentures offer an alternative means of prosthodontic rehabilitation. The use of overdentures, onlay dentures or overlay dentures to restore severely worn teeth can achieve excellent aesthetic and functional results. This article looks at the indications for treatment planning and provision of these prostheses.
CPD/Clinical Relevance: The use of these prostheses may prove a useful treatment option for the dental clinician managing the moderate to severely worn dentition.
Article
Rahat Ali
The prevalence of tooth wear (TW) in the United Kingdom is increasing. The Adult Dental Health Survey of 2009 suggested that 77% of adults had anterior TW. The report also suggested that 2% of the dentate adult population were found to have severe wear exposing secondary dentine or pulp.1 This is concerning as tooth wear patients often present to the restorative dentist complaining of poor dental aesthetics and dentinal sensitivity (Figure 1). Consequently, they may request treatment. Fortunately, loss of pulpal vitality is relatively uncommon, even in patients with severe wear.2,3
Figure 1. (a, b) A 24-year-old patient who consumed multiple cans of Diet Coca-Cola® on a daily basis for many years. He also ground his teeth at night. He disliked how short his lower teeth were becoming and had severe dentinal sensitivity to hot and cold drinks.
Nevertheless, the oral rehabilitation of TW patients is still complicated by a number of factors, including a lack of interocclusal clearance (for prosthodontic rehabilitation) and poor gingival aesthetics (Figure 2).
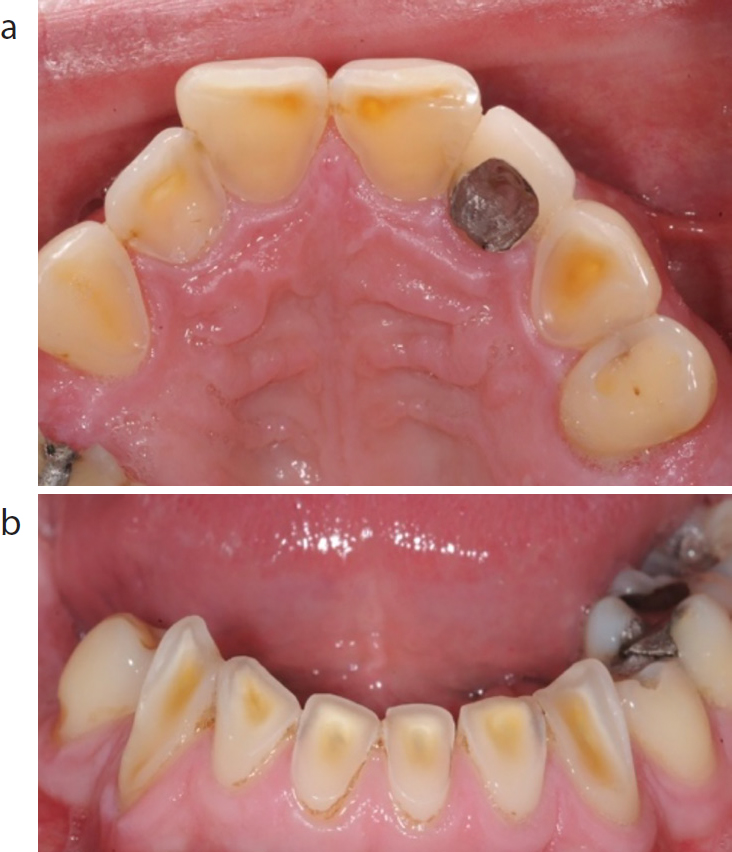
Figure 2. (a, b) A 22-year-old patient with previous anorexia nervosa. She had severe erosion of her maxillary teeth. Notice that the dento-alveolar compensation has obliterated the interocclusal clearance and produced excessive gingival display on smiling.
A number of operative options are available to the restorative dentist to rehabilitate patients with a worn dentition. These include the placement of direct composite resin (Figure 3), indirect extra-coronal restorations (both full and partial coverage) (Figure 4), as well as removable dentures.
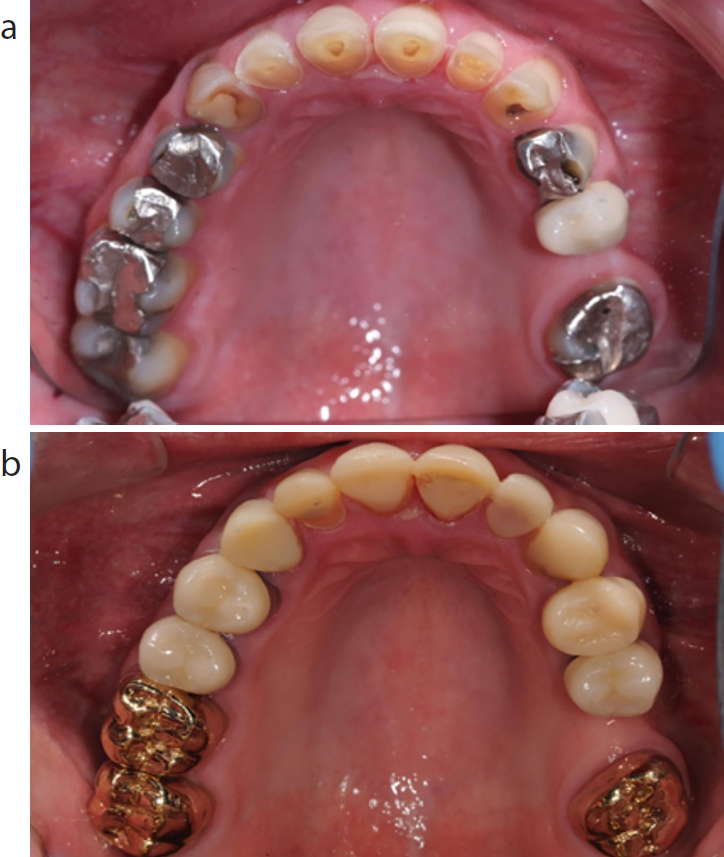
Figure 3. (a, b) A 21-year-old bulimic patient with erosion on his maxillary teeth who was rehabilitated with composite resin.Figure 4. (a, b) A 42-year-old patient with Gastro-Oesophageal Reflux Disease (GORD). He had erosion on his maxillary teeth and secondary caries and/or apical pathology on all of his maxillary posterior teeth. He was rehabilitated with anterior composites and posterior metal ceramic and full gold crowns (after any necessary root treatments were completed).
For patients presenting with more severe forms of TW, removable dentures offer an alternative means of prosthodontic rehabilitation. They can be prescribed as overdentures, onlay dentures or overlay dentures to restore any severely worn teeth. Overdentures are particularly useful when patients have teeth worn to near gingival level, which are are not suitable for crown lengthening surgery (CLS), that would have allowed restoration via direct/indirect restorations. Contra-indications to crown lengthening surgery include patients with multiple medical co-morbidities (eg severe bleeding dyscrasias or a history of anti-resorptive medications such as intravenous bisphosphonates or monoclonal antibodies therapy for malignancy). CLS is also contra-indicated for patients where the surgery would produce an unfavourable crown-to-root ratio on the worn teeth. Onlay/overlay dentures can be useful in patients with moderate to severe TW who may not be able to attend the multiple, lengthy appointments that may be necessary to allow fixed restoration of the worn dentition.
There are many techniques that can successfully be used to manage TW. In this paper, the design features, advantages and disadvantages of overlay/onlay and overdentures will be described for TW patients. The synchronous oral rehabilitation of a severely worn dentition requiring a maxillary overdenture and the opposing arch requiring direct restoration with composite resin will also be described. The importance of providing posterior occlusal stability in bilateral free-end saddles with partial dentures (after restoring a severely worn anterior dentition) is beyond the scope of the present article, and is covered elsewhere.4
Denture design and the tooth wear patient
For patients with severely worn dentitions, removable dentures can offer an attractive means of oral rehabilitation. Worn teeth can be restored/replaced with overdentures, onlay dentures or overlay dentures.
Overdentures
Overdentures sit over retained roots, (or severely worn teeth to gingival level) which provide support. The presence of the roots (and therefore a marked boney undercut) may preclude the provision of a fully extended flange for the denture (Figure 5). A flangeless tooth set-up could be considered for aesthetics (Figure 6). However, a peripheral seal cannot be obtained from this type of design. Therefore, any necessary retention must be obtained by alternative means, such as adhesives, clasps, guide surfaces, or utilizing the path of insertion to engage tooth undercuts. Where possible, the authors prefer the provision of a minimal labial acrylic flange (Figure 5). The technician should be asked to survey the alveolar ridge (where the the roots are located) and then asked to extend the acrylic flange 1 mm above the survey line. This will enhance the peripheral seal and retention of the prosthesis.
Figure 5. (a, b) A head and neck cancer patient with previous radiation-induced caries and severe GORD. The maxillary teeth ultimately fractured/eroded down to gingival level and were replaced with an acrylic overdenture. Notice the minimal flange for retention.
Onlay dentures
An onlay denture extends over the incisal or occlusal surfaces of worn abutment teeth and forms a butt joint finish.5 The butt joint can either be an acrylic resin-tooth interface (Figure 7) or metal-tooth interface. The latter interface is preferable in non-aesthetic zones. Parafunctional patients can fracture resin-based materials more frequently than metal and therefore metal may be the preferred option to onlay any worn (higher load-bearing) posterior teeth. This is especially true for parafunctional cases and in situations where there is limited interocclusal clearance to accommodate both acrylic and metal.
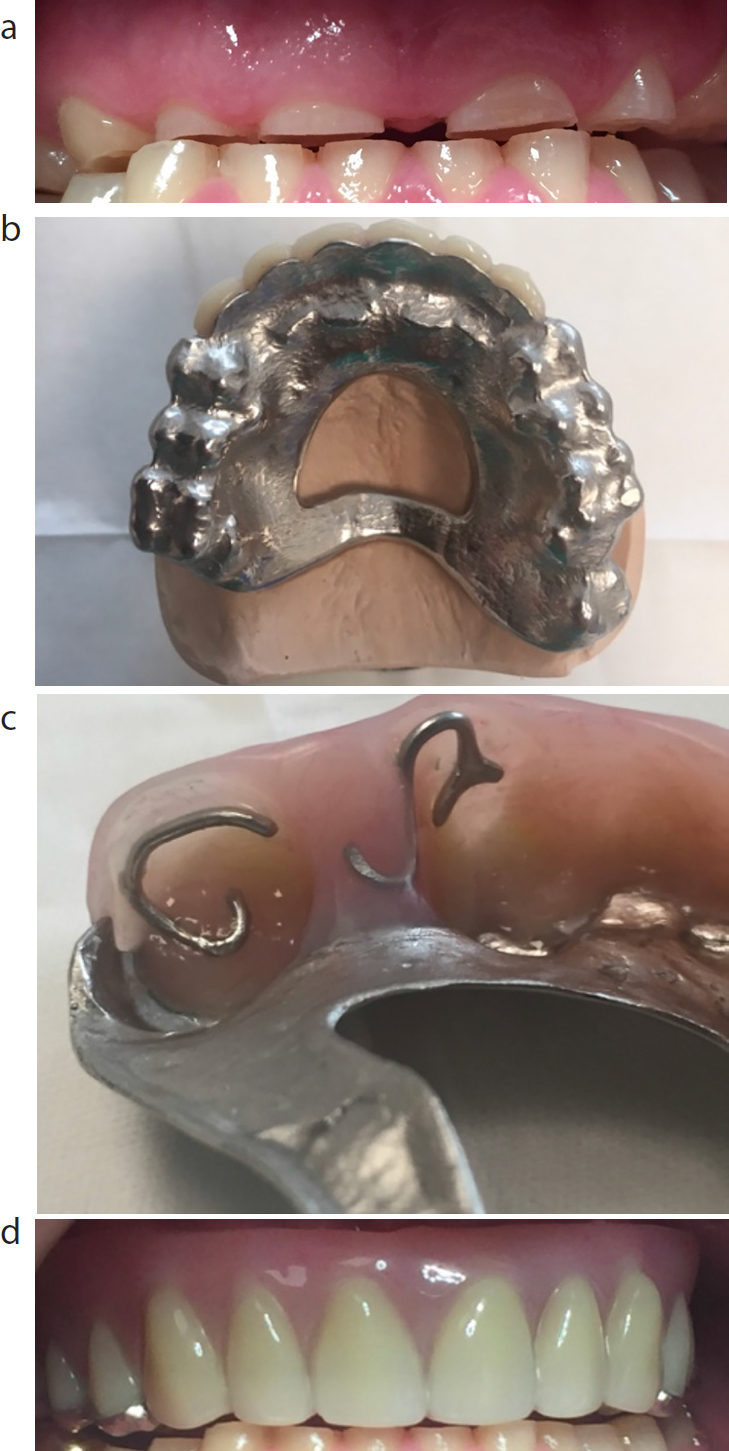
Figure 6. (a, b) A parafunctional patient rehabilitated with an overdenture. Note the flangeless set-up. Retention was obtained from clasps on the posterior teeth. This diminished the need for an anterior flange and therefore a peripheral seal.Figure 7. (a, b) A 55-year-old patient with severe GORD who eroded the majority of his maxillary teeth to near gingival level. He was rehabilitated with a chrome-based, removable onlay/over denture. The prosthesis located over his worn anterior roots, and onlayed onto the posterior teeth in the upper left quadrant. Note the use of tooth-coloured acrylic and conventional clasps for aesthetics and retention.
Overlay dentures
An overlay prosthesis veneers the labial surfaces of the worn teeth with tooth-coloured acrylic resin.5 Such prostheses are particularly useful in patients with moderate/severe TW (Figure 8). Internal clasps can be prescribed for the underlying teeth to augment retention. They are also of use in patients with an underlying skeletal or arch/width discrepency.6 The nature of the denture allows any underlying skeletal discrepencies and worn teeth to be camouflaged (Figure 9) and avoids the need for invasive orthodontic/orthognathic treatment.
Figure 8. (a–d) A 23-year-old patient with a severe parafunctional habit. He preferred rehabilitation with an overlay denture. Notice the prescription of chrome backings on the anterior teeth/metal occlusal surfaces on the posterior teeth and internal clasps to engage undercuts on the underlying teeth.Figure 9. (a–d) A 40-year-old patient with unglazed palatal porcelain on her maxillary crowns who consumed a high volume of carbonated drinks. Notice the tooth wear on her mandibular teeth. She had a Class II/1 incisal relationship and postured her mandible forward to gain more occlusal contacts. She was provided with a mandibular overlay prosthesis to produce a more Class I incisal relation.
However, the presence of teeth and alveolar bone can also reduce the space required to allow provision of a prosthesis. Also a denture may not be socially acceptable to many patients who may request rehabilitation with a fixed option. Furthermore, the teeth and roots underneath the denture are at risk from developing caries and periodontal disease, unless patients demonstrate excellent plaque control.7 The authors therefore advise their patients to load their dentures with Duraphat® 2800ppm F toothpaste at least once a day before insertion, and to clean the underlying roots and teeth meticulously at least 2–3 times daily.8 Rehabilitated patients are advised to visit their dental practitioner on a 3-monthly basis to ensure that plaque control is optimal, especially around the underlying roots and teeth.
Synchronous oral rehabilitation of a worn maxillary and mandibular dentition
If a patient with moderate to severe TW is to be rehabilitated with a removable prosthesis, it must be ensured that he/she has good plaque control and is free of primary dental disease. The occlusion should be carefully evaluated to identify the patient's intercuspal position (ICP) and retruded contact position (RCP). Patients with a pronounced horizontal slide from ICP to RCP may already have sufficient space to allow prosthetic rehabilitation (Figure 10). Patients with insufficient space will need their vertical dimension carefully increased on the retruded arc of closure (RAC).
Figure 10. A parafunctional patient requiring a maxillary denture. His ICP (a) does not lend itself to prosthodontic rehabilitation. However, in RCP (b) he had sufficient space to allow provision of a maxillary partial denture and restoration of his mandibular teeth.
Initial planning will involve making primary impressions of the worn dentition with irreversible hydrocolloid. The resulting casts should be surveyed and an appropriate path of insertion (POI) should be selected, being mindful of the patient's dexterity. Once the denture has been designed, appropriate tooth preparation should be performed. Any sharp edges on retained roots should be smoothened off. Otherwise they may fracture off the master cast. Any teeth due to be overlayed may need reduction, both vertically and labially, to facilitate optimal tooth positioning. The master impressions should then be made in an accurate and stable impression material.
Once the master casts have been poured and trimmed, wax rims on rigid, stable base plates should be requested and the occlusion should be recorded in RCP (Figure 10) or on the RAC, if there is insufficient space (Figure 11 (a-d)). When an overdenture is being fabricated, a minimal flange should be prescribed for the wax rim. This will prevent the patient's lip support from being unduly distorted. If an overdenture is being prescribed for one arch and the opposing arch is also planned for restoration, the occlusion must be recorded to allow rehabilitation of both dentitions, otherwise all of the available space may be obliterated by provision of the overdenture alone (Figure 11 (c, d)).
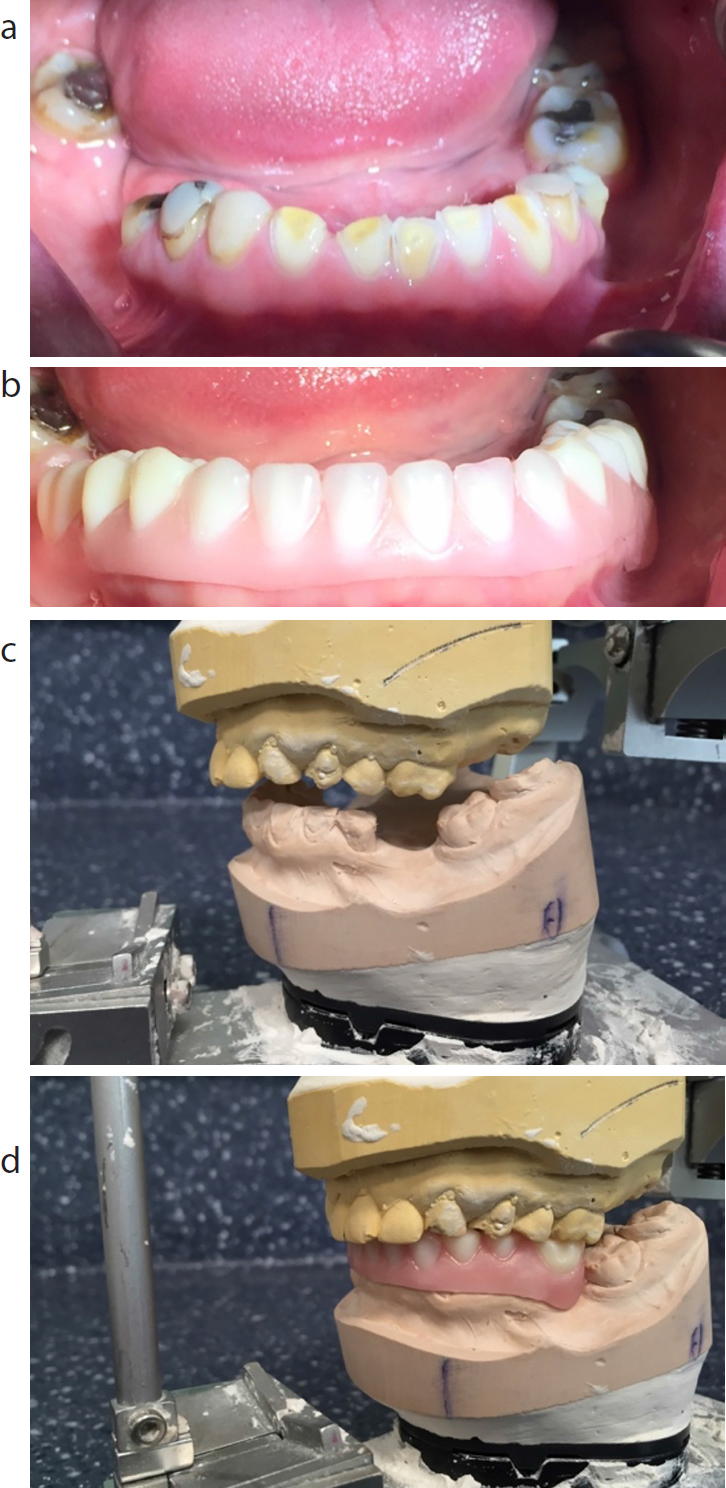
Figure 11. (a, b) A 41-year-old patient with previous GORD and a parafunctional habit. Notice the severe acid erosion of the maxillary teeth and the mild wear on the mandibular teeth. His ICP and RCP were co-incident with no space to allow rehabilitation. (c, d) Wax rims were used to record the occlusion on the RAC at a slightly increased vertical dimension to accommodate a maxillary overdenture. Notice the minimal flange on the wax rim and how space was also left to allow restoration of the worn mandibular teeth. (e, f) The tooth try-in for the maxillary overdenture and the wax-up of the worn mandibular teeth for the patient in (a, b). (g, h) The wax-up of the mandibular cast can be duplicated and a full coverage index can be constructed in a vacuum-formed material or transparent silicone (eg Memosil®). (i) The tooth try-in of the maxillary overdenture and aesthetic preview of the mandibular arch for the patient in (a, b).
Once the casts have been mounted, the laboratory can set up a tooth try-in for the overdenture. If the opposing arch needs restoration (with composite or indirect restorations), the technical team can also wax-up the opposing cast (Figure 11 (e, f)) as per the vertical dimension dictated by the the wax rims.
A vacuum-formed or silicone stent of the waxed-up opposing teeth is used to carry out an aesthetic preview stage (Figure 11 (g,h).9 The opposing teeth are coated with vaseline (as a separating medium) before loading the stent with temporary crown and bridge material. Once set, the stent can be removed and the tooth set-up, occlusal relationship, vertical dimension and aesthetics of the proposed treatment can be evaluated.
Once the tooth position of the overdenture has been agreed upon, the prosthesis can be processed in acrylic. Although acrylic can be useful for erosive cases where there is an abundance of prosthetic space, it is an ill advised material for parafunctional cases. It is prone to fracture and therefore patients who clench/grind should be prescribed a chrome-based denture with metal backings on the anterior teeth (Figure 8). Metal-based dentures require less prosthetic space and are less prone to break than acrylic.
If metal backings are required for the teeth, both the patient and clinician must clinically verify the tooth set-up before the metal work is waxed-up and cast (Figure 12 (a, b)). If backings are prescribed, they normally terminate just short of, or up to, the incisal edge, to protect the teeth (Figure 8).
Figure 12.
(a) A putty index of the tooth set-up can be made to help construction of the metal framework (b) for the patient in Figure 11 (a, b). The laboratory can use the index as a point of reference and ensure that the metal backings (and any retention tags) can be positioned without encroaching on the proposed tooth position. Notice the overlay of the metal framework onto the UR6 for support as the tooth was unopposed. (c) The definitive maxillary chrome-based overdenture for the patient in Figure 11 (a, b). Notice the conversion from a Class III to Class I incisal relationship. Also note the minimal labial flange for retention and conventional clasp on the UR6. After the patient adapted to the prosthesis, the mandibular teeth were due for restoration as per the wax-up in Figure 11 (e, f). (d, e) The mandibular wax-up and lingual Memosil® index for the patient in Figure 11 (a, b). (f, g) The definitive maxillary chrome-based overdenture and mandibular composite restorations for the patient in Figure 11 (a, b). The lingual index in (d, e) was used to restore the mandibular teeth with Ceram-X Mono® composite resin (Densply Sirona). Notice the similarity to the aesthetic preview in Figure 11 (i).
By virtue of retaining and overlaying any roots, maxillary chrome overdentures can gain considerable amounts of tooth support. It is therefore not necessary to prescribe full palatal coverage connectors to gain additional support from the hard palate. Chrome-based ring connectors for maxillary overdentures can be advanageous if the patient has a mild gag reflex or a palatal torus (Figures 8 and 12 (a, b)).
The metal work is tried in clinically to assess its fit, accuracy and retention. Teeth can then be added in wax onto the metal framework. This penultimate stage is strongly recommended to evaluate the occlusion and shade of the acrylic teeth (which may change with the provision of metal backings). Any necessary changes can then be made before the overdenture is processed and delivered (Figure 12 (c)).
Once the overdenture has been inserted, the opposing dentition can be restored to contact it. If the antagonistic teeth have been waxed-up and verified as being accurate at the preview appointment, a lingual index in putty or clear silicone (Memosil®, Kulzer) can be be constructed (Figure 12 (d, e)). This can be used to place direct composite restorations in a planned fashion to contact the opposing denture at the correct vertical dimension (Figure 12 (f, g)).10 Alternatively, a full coverage index of the wax-up can be used (for temporization) if crowns are to be prescribed.
For severely worn dentitions, the authors frequently work up the maxillary and mandibular dentitions in tandem, as per the protocol described above. Once the overdenture has been delivered, it is used as a reference point to restore the opposing arch with either direct or indirect restorations (Figure 12 (f, g)).
Discussion
Removable prostheses clearly allow the aesthetics of a worn dentition to be restored. They represent a minimally destructive means of rehabilitating the patient. The teeth (or roots) are often retained underneath the denture. From a patient's psychological perspective, this may be preferable to extracting a set of worn teeth. Maintaining the worn teeth can allow clasps to be incorporated into the denture design (Figure 8), and therefore augment retention. Tooth retention will also maintain their periodontal ligaments and therefore the proprioceptive feedback, jaw reflexes, neuromuscular control and ability to adapt to an increased vertical dimension, which is typically absent in an edentulous patient.11, 12, 13, 14 Tooth retention will also retain the associated alveolar ridge.15,16
As a result, any useful boney undercuts can also be engaged to further enhance retention for the removable prosthesis (Figures 5 and 12).
For the aforementioned reasons, prosthetic retention is not a commonly reported problem for TW patients. Rather they tend to encounter problems with their prosthetic superstructures. Woodley et al reported that 64% of their denture cohort had complications, which was mainly fracture of the acrylic or the teeth.17 Patients and their referring practitioners must be warned of this. The use of chrome-based dentures (especially in parafunctional cases) for the framework and to onlay the posterior teeth may reduce these reported complications. Furthermore, the prescription of metal backings can be exploited to enhance tooth retention, if acrylic teeth keep fracturing off. Although the authors routinely prescribe backings and retention tags, anterior teeth can still fracture. It is therefore imperative to ensure that the metal backing extends just short (or up to) the incisal edge of the acrylic teeth. This will protect them from debonding during static and dynamic mandibular movements. If repeated debonding is observed, the metal work can be perforated to further enhance macro-mechanical retention of the acrylic teeth to the framework.
Conclusion
In this paper, the authors have described how overlay, onlay and overdentures can be used to rehabilitate moderate/severe TW patients. Although the prostheses can be technically complex to work up and fabricate, the improvement in aesthetics can be impressive (Figures 5, 9 and 12). Clinicians clearly need an excellent understanding of prosthodontics and equally good laboratory support if they wish to provide such complicated prostheses.