Luyk NH, Steinberg B Aetiology and diagnosis of clinically evident jaw trismus. Aust Dent J. 1990; 35:532-539
Vaishali MR, Roopashri G, David MP, Indira AP Trismus. Ind J Dent Advance. 2010; 2:304-308
Dhanrajani PJ, Jonaidel O Trismus: aetiology, differential diagnosis and treatment. Dent Update. 2002; 29:88-94
Poormina G, Poormina C Trismus. J Health Sci Res. 2004; 5:15-20
Chen E, Ricciotti R, Futran N, Oda D Head and neck rhabdomyosarcoma: clinical and pathologic characterisation of seven cases. Head Neck Pathol. 2017; 11:321-326
Rahman HA, Sedky M, Mohsen I, Taha H, Loaye H, Zaghloul MS Outcome of pediatric parameningeal rhabdomyosarcoma. The Children Cancer Hospital, Egypt, Experience. J Egypt Nat Cancer Inst. 2013; 25:79-86
Iatrou I, Theologie-Lygidakis N, Schoinohoriti O, Tzermpos F, Vessala AM Rhabdomyosarcoma of the maxillofacial region in children and adolescents: report of 9 cases and literature review. J Cranio-Maxillofac Surg. 2017; 45:831-838
Lee RJ, Lee KK, Lin T, Arshi A, Lee SA, Christensen RE Rhabdomyosarcoma of the head and neck: impact of demographic and clinicopathologic factors on survival. Oral Surg Oral Med Oral Pathol Oral Radiol. 2017; 124:271-279
Radzikowska J, Kukwa W, Kukwa A, Czarnecka A, Krzeski A Rhabdomyosarcoma of the head and neck in children. Contemp Oncol. 2015; 19:98-107
Trismus can be a common complaint encountered in general dental practice. A 15-year-old female presented to the Emergency Department with a history of acute onset and worsening trismus, pain and extra-oral swelling following placement of a restoration in the lower right first molar tooth. An initial diagnosis of trismus associated with either muscular spasm or a haematoma following an inferior alveolar nerve (IAN) block was assumed. The patient was reviewed the following week, the trismus and swelling having increased. An urgent MRI scan showed a large heterogeneous mass in the right masticator space. A biopsy under general anaesthetic diagnosed a rhabdomyosarcoma. The patient was referred to the oncology team for chemo/radiotherapy treatment.
CPD/Clinical Relevance: Although ‘common things occur commonly’, it is important to remember that common symptoms and presentations can lead to more rare diagnoses. Prompt referral for specialist advice needs to be sought should first line management of trismus prove to be unsuccessful.
Article
Manal Mohammed
Trismus is defined as the ‘prolonged tonic, spasm of the masticatory muscles that restrict normal mouth opening’.1 Degree of mouth opening varies widely between patients but between 40–60 mm is considered a normal range. Mild trismus is considered >30 mm, moderate between 15–30 mm and severe trismus <15 mm.2
There are many causes of trismus and it can be a common complication of dental treatment, such as the extraction of teeth, in particular lower third molars.3 Trismus is a known complication following the administration of an inferior alveolar nerve (IAN) block.2 This usually occurs if the needle has penetrated a vessel or the medial pterygoid muscle and can result in the formation of a small haematoma.3
Another common cause of trismus is masticatory space infection. These infections can be odontogenic or non-odontogenic in origin.4 Antibiotics are often required to be given immediately to prevent the spread of infection to neighbouring fascial spaces. This in turn can lead to serious complications, such as mediastinitis3 or airway compromise.
Temporomandibular joint disorders (TMJDs) are regularly associated with trismus, as well as other associated symptoms. TMJDs include myofasial pain, disc displacement, arthritis or fibrosis.2,3,4 Other causes of trismus include fractures to the mandible or zygomaticomaxillary complex, congential malformations, drug therapy, such as phenothiazine and succinyl choline, radiotherapy, chemotherapy and psychogenic causes, such as hysteria trismus.1–4 Less commonly, tumours can arise in the temporomandibular joint itself or in the surrounding anatomical structures.
The initial phase of trismus can be managed with the application of heat therapy, analgesics, muscle relaxants, eg diazepam, and soft diet.3,4 Jaw physiotherapy exercises, appliances and, in some cases, surgery may be required to manage the trismus in the long term, depending on the diagnosis.4 Successful treatment depends on the recognition of the cause of the trismus. If first line management proves to be unsuccessful, then specialist advice will usually need to be sought.
A case of a 15-year-old who developed acute trismus, pain and swelling following a routine restoration of her lower right first molar (LR6) by her general dental practitioner will be presented.
Case report
A 15-year-old girl presented to the Emergency Department (ED) at Gloucestershire Royal Hospital (GRH) with pain and swelling to the right side of her face. The patient was fit and well, had no known allergies and was taking no regular medication apart from analgesia. The pain and swelling began directly after the restoration of the LR6 under local anaesthetic 4 weeks previously. After 2 weeks, symptoms had not improved so advice was sought from her dentist and subsequently an out-of-hours emergency dentist. Both clinicians had assumed a diagnosis of an acute dental abscess and prescribed her broad-spectrum antibiotics.
The patient was then brought by her parents with worsening symptoms to the ED at GRH. The swelling was hard and non-fluctuant, extending from the preauricular area beneath the zygomatic arch to the angle of the mandible. Her mouth opening at the time of presentation was around 15 mm. As a result of the reduced mouth opening, she could only manage a soft diet. The pain was described by the patient as a generalized ache to the right side of her face which had localized to the upper right quadrant of the mouth in the previous two days.
Owing to limited mouth opening, it was difficult to visualize the teeth in the upper right quadrant, however, when digital pressure was applied to the occlusal surfaces of the teeth, all the teeth were tender. It was not possible to examine the palatal aspect of her teeth or hard and soft palate. The restoration in the LR6 appeared to be clinically sound. The patient was systemically well and apyrexial.
Investigations
Initially, an orthopantomogram (OPG) was taken to try and ascertain whether the swelling was due to a dental cause. The OPG showed the teeth were sound with no sign of dental decay and the recent restoration on the LR6 was small and not in close proximity to the dental pulp. The OPG, however, did show a diminished right condyle and mandibular ramus and an increased depth of the sigmoid notch. The height of the condyle remained the same, but was significantly narrowed in the anteroposterior and mediolateral dimensions (Figure 1).
Figure 1. An OPG showing a diminished right condyle and increased depth of sigmoid notch.
Differential diagnoses
A dental cause for her swelling was ruled out due to insufficient evidence clinically and radiographically. Owing to the appearance of the right side of her mandible on the OPG, destructive pathology was suspected, despite it being rare in a patient of this age.
Diagnosis
An urgent MRI scan was requested and the patient was reviewed. At her review appointment, it was found that swelling had increased markedly, felt much firmer and was more prominent extra-orally. The trismus had significantly increased and her mouth opening was 8 mm. The patient's pain was unchanged.
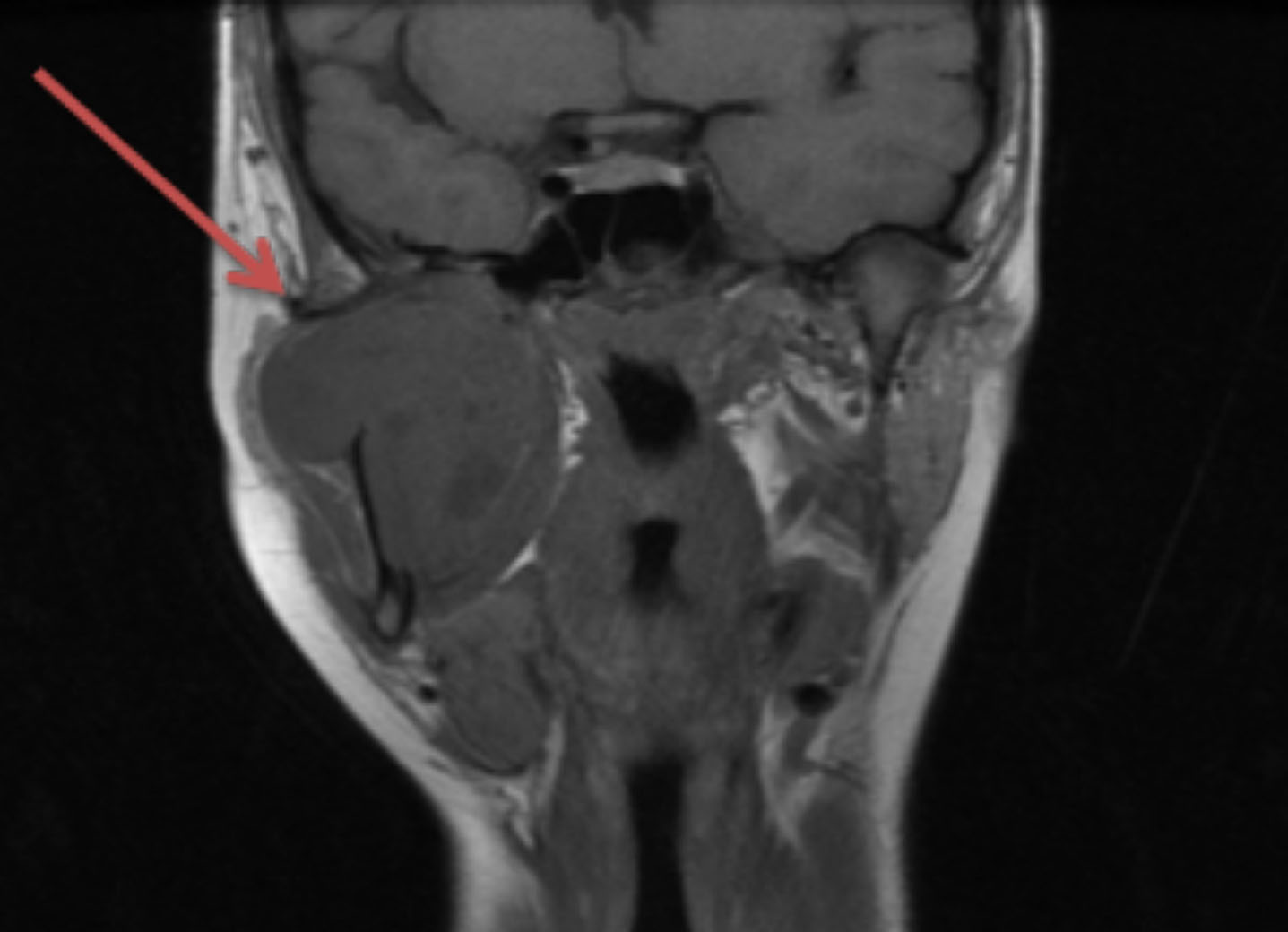
The MRI scan showed ‘a large solid enhancing mass on the right masticator space. There was associated extensive destruction of the right mandibular condyle and ramus which extended into the angle and posterior body of the mandible inferiorly. There was bulging into the parapharyngeal region medially, and the deep lobe of the parotid gland postero-laterally, abutting the external carotid artery. Postero-medially, it extended to the carotid space, abutting the non-dominant right internal jugular vein and internal carotid. Anteriorly, it extended to the lateral wall of the maxillary sinus in the retromaxillary fat pad and there was involvement of the posterior aspect of the maxilla, including the posterior right alveolar process. There appeared to be paraneural extension of the tumour along the mandibular division of the right trigeminal nerve extending up to the foramen ovale’ (Figure 2).
Figure 2. A coronal view of the MRI scan indicating the extensive tumour of the right masticator space.
As a result of the MRI scan, an urgent biopsy of the swelling was arranged under a general anaesthetic by the oral and maxillofacial surgery department. The biopsy confirmed the lesion to be a parameningeal embryonal rhabdomyosarcoma. A staging CT scan showed metastatic disease bilaterally in the level II neck nodes and multiple additional lung nodules.
The patient was then referred to the paediatric oncology team at the closest regional centre. She had a percutaneous endoscopic gastrostomy (PEG) inserted to help her with feeding and began chemotherapy and radiotherapy in accordance with the European Paediatric Soft Tissue Sarcoma Study Group (EpSSG) protocol. This involved an initial 12 weeks of chemotherapy followed by 4 months of radical radiotherapy to both the primary and metastatic sites. The tumour had regressed from 63 mm to 37 mm in diameter following this, indicating stable residual disease.
The patient is now completing a 12-month maintenance chemotherapy regimen. Unfortunately, surgery was not a viable option at this stage as the tumour had extended to the base of the skull. A future MRI scan will help plan her next phase of treatment once the maintenance chemotherapy regimen is complete.
Discussion
Rhabdomyosarcoma (RMS) is a rare soft tissue sarcoma originating from primitive mesenchyme tissue.5,6 It is the most common paediatric soft tissue sarcoma with an incidence of 3.5% malignancies in children younger than 14 years and 2% in adolescents aged 15–19 years.7 RMS can occur in various sites in the body, such as head and neck, genito-urinary and the extremities.8 Head and neck RMS accounts for about 35% of all RMS in children.6 The male to female ratio is 1:1.5.7
RMS are known to proliferate rapidly and can infiltrate neighbouring tissues and organs. Metastasis to distant organs, such as lungs, bone marrow and the central nervous system, occurs statistically more often than to lymph nodes.6
Owing to the rarity of head and neck RMS, most narratives of this disease have been published as case reports.5 The pathogenesis of RMS remains unclear due to its relative rarity but the mesenchymal cancer cells responsible for RMS are largely believed to originate from regulatory disruption of skeletal muscle progenitor cell growth and differentiation during myogenesis.8
RMS is often difficult to diagnose, given its similarities to other cancers and varying levels of differentiation.8 Differential diagnoses include lymphoma and Ewing sarcoma.8 Localization of the primary tumour has a prognostic value and can aid with the therapeutic management strategy.6 There are three tumour sites that can be distinguished in the head and neck region: orbital, parameningeal and nonparameningeal sites.6 Parameningeal RMS are the most common and account for around 50% of all head and neck RMS cases. Parameningeal RMS include tumours of the nasopharynx, middle ear, paranasal sinuses, infratemporal fossa and pterygopalatine fossa.6,9 They represent a diagnostic and therapeutic problem as they have a tendency to invade critical anatomical structures such as the central nervous system.6,9 They remain asymptomatic at the early stages of tumour growth.9 As a result, the outcome of parameningeal RMS is poor in comparison to other sites and often necessitates a more aggressive therapy response owing to the delay in diagnosis, tumour tendency to intracranial spread and increased local recurrence.6
Treatment modalities for RMS of the head and neck may involve a combination of surgical resection, chemotherapy and/or local adjuvant radiotherapy.8 For parameningeal RMS, a radical surgical approach may not be feasible due to the vital structures involved,6 as was the case for this patient.
Prognosis of RMS is dependent on patient age, tumour stage, size, histology, distant metastases and response to chemotherapy.6 The 5-year survival rate for RMS has increased from 25% to 73% due to advances in oncology over recent decades.9 Unfortunately, this can decrease significantly if there are distant metastases involved.9
Conclusion
Although this case presents a patient with a rare cause for acute trismus, it is important to remember that ‘common things occur commonly’. Hence the initial differential diagnoses of an acute dental abscess or muscular trismus post-operatively after an IAN block. However, should trismus persist after first line management is unsuccessful, then concerns should be raised. Urgent referral to the local oral and maxillofacial department is advised for further specialist investigation.