Trauma of maxillary incisors is frequent and dental practitioners have to be competent in managing the consequences. Complicated crown root fractures of anterior teeth can have profound aesthetic and psychological implications on patients. In younger patients, if extractions are considered, it can lead to complex prosthodontic challenges in the future. Ideally, an attempt should be made in restoring the traumatized teeth, so an effective aesthetic and functional result can be reached. This case report highlights the treatment of complicated crown root fractures on maxillary incisors using endodontics and fragment re-attachment of the fractured crowns. Twelve-month follow-up of the treatment demonstrated aesthetic and functional success and delayed the need for prosthetic replacement.
CPD/Clinical Relevance: This paper describes traumatic injuries of teeth and how management via fragment re-attachment of the fractured crowns has led to delay of definitive prosthetic treatment.
Article
Khawer Ayub
Dental injuries are typically classified as displacements, fractures or combinations of the two.1,2 A crown-root fracture is defined by the fracture crossing enamel, dentine and cementum into the periodontal ligament.3 A complex injury will have pulpal involvement. These injuries are often associated with maxillary incisors4 and in patients before the age of 19.5
Once the fractured portion has been removed, an assessment must be made of the restorability of the tooth. Key considerations include the nature of the fracture, whether it is simple or complex. Further, the depth of the fracture must be assessed. In particular, if marginal isolation is possible without creating periodontal complications and the availability of remaining tooth structure to support restoration.
Where fractures are complex one must also assess the ability for optimal isolation with a rubber dam for possible endodontic treatment and, ultimately, the long-term restoration of the tooth.6 If a tooth is not restorable this can have profound implications for the patient. Never is this more important than in the growing patient for whom tooth loss may result in prosthodontic challenges in the future. As such, if a tooth is unrestorable, is it wise to leave the root in situ? If there is any possibility of restoration it should be considered, even if this is considered a provisional phase until adulthood, when more predictable solutions may be sought.
There have been many methods proposed for the management of crown-root fractures.3,7,8,9 Equigingival crown-root fractures can usually be treated with fragment re-attachment or adhesive restoration. If the pulp is involved, endodontic treatment may be required and a post-retained core placed if tooth structure is limited. If the extent of fracture is significantly more subgingival, then treatment may include: gingivectomy, surgical or orthodontic extrusion or intentional replantation.
Fragment re-attachment has been reported to be a success due to restoration of form, contour, positioning and aesthetics: in particular, shade, texture and tooth translucency/opacities.10,11 It can be considered a simple procedure, thereby saving time and reducing costs.12 Many methods have been suggested for re-attachment of fractured fragments, ranging from simple bonding to additional preparation of bevels and chamfers, over contouring, internal grooves or composite build-ups.13,14 The technique of re-attachment without additional preparation may be beneficial when complete adaptation of the fragment is possible.15
This case report describes the clinical management of complicated crown-root fractures of maxillary central and lateral incisors. Treatment included orthograde endodontics, direct fibre post, palatal gingivectomy and re-attachment of the fractured fragments.
Case report
A fit and healthy 17-year-old female presented at The University Dental Hospital of Manchester with fractured anterior teeth following trauma. Further history revealed she had attended her general dental practitioner (GDP) one week previously and the roots had been dressed with non-setting calcium hydroxide but no further treatment had been provided. A referral was made for definitive treatment planning. She presented in no pain or distress. She had located and kept the broken fragments at the time of trauma.
There were no abnormalities noted extra-orally or with the soft tissues;
The oral hygiene was good and there was no primary disease;
An intact, unrestored dentition having recently completed fixed orthodontic treatment;
She was wearing her vacuum-formed orthodontic retainer with a temporary crown and bridge material in the space of the fractured upper right central and lateral incisor;
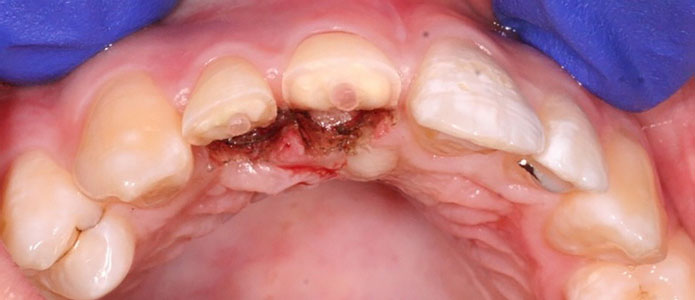
On removal of the vacuum-formed retainer there were complicated crown-root fractures of the UR1 and UR2 that extended sub-gingivally, with temporary restorations in situ;
Trauma assessment revealed: no mobility, no tenderness to percussion or abnormal periodontal pocketing, however, the UR1 and UR2 gave no response to sensibility testing;
The fractured fragments were retained by the patient, stored dry in tissue paper;
The two coronal fragments were held together with her fixed orthodontic bonded retainer that had fractured along with the teeth (Figure 2). The fractured fragments could be easily approximated back into their natural position (Figure 3).
Figure 1. Pre-operative view highlighting fractures of UR1 and UR2.Figure 2. Fractured crown of UR1 and UR2 held in place with the patient's fixed orthodontic retainer.Figure 3. Fractured fragments relocated into position
Radiographic findings
Radiographic examination revealed crown-root fractures of UR1 and UR2, radio-opaque dressings placed within the pulp and widening of the periodontal ligament at the root apices (Figures 4 and 5). No root fractures were evident.
Figure 4. Pre-operative radiograph of UR2.Figure 5. Pre-operative radiograph of UR1.
Diagnosis
Complicated crown-root fractures of the UR1 and UR2.
Management options
Leave and maintain the current retainer until a definitive implant or resin-retained bridge-based solution could be considered in the future;
Extraction of the retained roots with possible socket preservation strategy to minimize the loss of hard and soft tissues;
Root canal treatment and indirect restoration or, if possible, re-attachment of the fractured portions.
After discussion of all options it was agreed an attempt would be made to treat the teeth endodontically and re-attach the fragments. Following the injury, the patient retained the fragments which were stored dry.
Treatment
Appointment 1 (2 weeks post injury)
The teeth were isolated with rubber dam and the previous restorations were removed. Shaping of the root canals was completed with NiTi rotary instruments, copious irrigation with NaOCl and obturation using greater taper-matched cones and warm vertical compaction. The teeth were sealed with temporary restorations with a view to placing direct fibre posts and re-attaching the fragments (Figure 6).
Figure 6. Post-endodontic radiograph of UR1 and UR2
Appointment 2 (4 weeks post injury)
The patient returned asymptomatic following endodontic treatment. The root canal spaces were prepared for direct fibre posts. These were bonded and modified to extend approximately 2 mm from the remaining tooth structure. It was felt that this would aid resistance and retention form for re-attachment of the fragments.
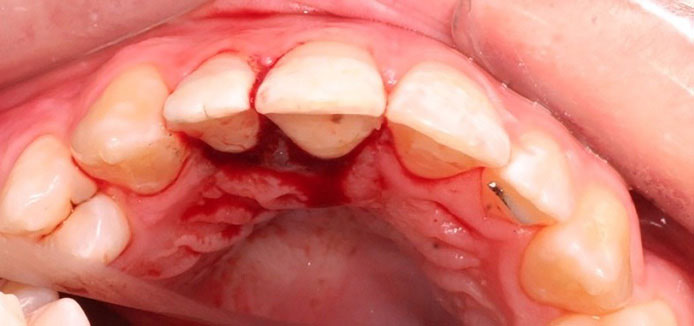
The pulp chambers of the fractured fragments were hollowed out to remove any necrotic tissue and accommodate the posts. The sharp and thin sections of cervical root dentine were also smoothed to aid seating of the fragments (Figure 7). An effort was made to ensure the fragments fit passively around the post and seated into position. Electrosurgery was completed to expose the palatal margins of the teeth (Figure 8). The fragments were bonded into place with a dual cure resin cement and the palatal margins were finished with diamond burs (Figure 9). Immediately post fragment re-attachment there was a mismatch in shade due to dehydration of the fragments (Figure 10). The patient was advised that this discrepancy in shade would improve with rehydration of the re-attached fragments.
Figure 7. Tooth fragments were hollowed out to accommodate the posts in the pulp space. Thin fragments of root dentine were smoothed to aid seating at the cervical margin.Figure 8. Occlusal view showing cemented posts in the UR1 and UR2 with palatal electrosurgery to expose the tooth margins.Figure 9. Occlusal view post fragment re-attachment. Bleeding is visible as the margins were smoothed with a fine diamond bur.Figure 10. Frontal view post fragment re-attachment showing the difference in shade due to fragment dehydration.
Appointment 3 (8 weeks post injury)
Clinical and radiographic review showed good rehydration of the fragments (Figures 11, 12 and 13), with no obvious pathology and good soft tissue healing. The patient was pleased with the aesthetic result.
Figure 11. Occlusal view showing soft tissue healing 8 weeks post injury.Figure 12. Frontal view showing reintegration of fragments 8 weeks post injury.Figure 13. Close up view of UR1 and UR2 showing acceptable aesthetics and restoration of shade, contour, texture and opacities at the incisal edges.
Appointment 4 (6 months post injury)
On review the patient was happy with the aesthetic and functional outcome. Clinical findings revealed no obvious abnormalities, however, there was some slight staining at the junction of fragment re-attachment. This was of no concern for the patient and options of masking this with composite were discussed. However, she decided not to have any treatment completed.
Appointment 5 (12 months post injury)
The patient was reviewed 12 months post injury and was happy with the aesthetic and functional outcome. She had returned to see her orthodontist who provided her with a new bonded wire retainer on the palatal aspect of her maxillary anterior teeth. Clinical examination (Figures 14, 15, 16 and 17) showed good integration of the re-attached fragments, however, the horizontal fracture lines at the junction of the re-attachment were visible; these were of no concern to the patient.
Figure 14. Frontal view at 12-month review showing acceptable aesthetics and good integration of the re-attached fragments.Figure 15. Lateral view showing the re-attached fragments.Figure 16. Occlusal view showing the new fixed wire orthodontic retainer and healing of soft tissue around the UR1 and UR2.Figure 17. Natural smile showing restoration of colour, contour, texture, opacities and function of the UR1 and UR2.
The authors will aim to review this case clinically and radiographically to assess longer term outcome of this treatment.
Discussion
When compared to alternative treatment options, fragment re-attachment can be more conservative, efficient, cheaper and provide favourable aesthetic outcomes. Complicated crown root fractures may require intra-canal anchorage in the form of a post. Numerous case reports have demonstrated successful treatment of complicated crown root fractures through the use of fibre posts and fragment re-attachment.16–21 Fibre posts can provide an aesthetic alternative to cast metal posts in the anterior zone. They have a similar modulus of elasticity so that, when bonded to remaining tooth structure, they can distribute occlusal stresses evenly.16,22 The use of resin cements alongside fibre posts can increase retention of the fragment as it interlocks both the fibre post and tooth fragment together.22,23 In this procedure, there was no need to drill through the crown as the post was bonded into the hollowed pulp chamber; retaining maximal tooth structure within the fragment can reduce stress placed on it.17
The above case highlights the complicated nature of treatment dental trauma. However, it demonstrates that good outcomes can be achieved in what appear to be hopeless cases. The treatment has allowed the patient to retain her teeth so far and delay the need for any possible prosthetic replacement. It was thought that fragment re-attachment would give the best aesthetic outcome over a direct resin restoration or prosthetic replacement, but it must be noted that there is a paucity of data to support this type of intervention. As such, the long-term prognosis of these teeth remains uncertain;24 accordingly, this has always been considered a provisional treatment plan that should be maintained for as long as possible.
The aesthetics were acceptable given that the teeth were re-attached 4 weeks post injury. A fracture line on the buccal aspect of the UR1 and UR2 has become visible and, with time, this will accumulate stains. This could be easily managed with direct composite veneer across the fracture line, if necessary.