Solutions for implants placed with prosthetic inconvenience Graeme Bryce Nicholas Diessner Ken Hemmings Neil MacBeth Dental Update 2024 46:11, 707-709.
Surgeon Commander (D) Graeme Bryce Royal Navy, Consultant in Restorative Dentistry, Centre for Restorative Dentistry, Defence Primary Health Care (Dental), Evelyn Woods Road, Aldershot, GU11 2LS
BDS, MSc, FFGDP, MGDS, MFGDP, MFDS, FDS(Rest), Consultant in Restorative Dentistry, Defence Primary Health Care Centre for Restorative Dentistry, Evelyn Woods Road, Aldershot, GU11 2LS, UK
A prosthetically-driven approach for dental implant placement offers the most predictable means of achieving a biologically stable and aesthetic implant-supported restoration. Optimal dental implant placement may be limited by local factors and complicate the prosthetic reconstruction. This article aims to offer guidance on the surgical and prosthetic options available to manage suboptimally-positioned dental implants.
CPD/Clinical Relevance: This article is relevant to dental clinicians placing and restoring dental implants, and those who are considering them in treatment planning.
Article
Graeme Bryce
The popularity of implant-supported restorations has led to the development of increasingly innovative clinical techniques to provide successful and aesthetic tooth replacements. Successful implant outcomes are underpinned by positioning the fixture at the optimal vertical and horizontal position within the alveolar bone, encouraging the development of a healthy peri-implant soft tissue collar1 and reducing the risks of peri-mucosal complications.2 The importance of this implant-tissue association has led to the development of ‘prosthetically driven’ surgical protocols, where the optimal prosthetic tooth position2 is used to determine the correct spatial position for the implant fixture.
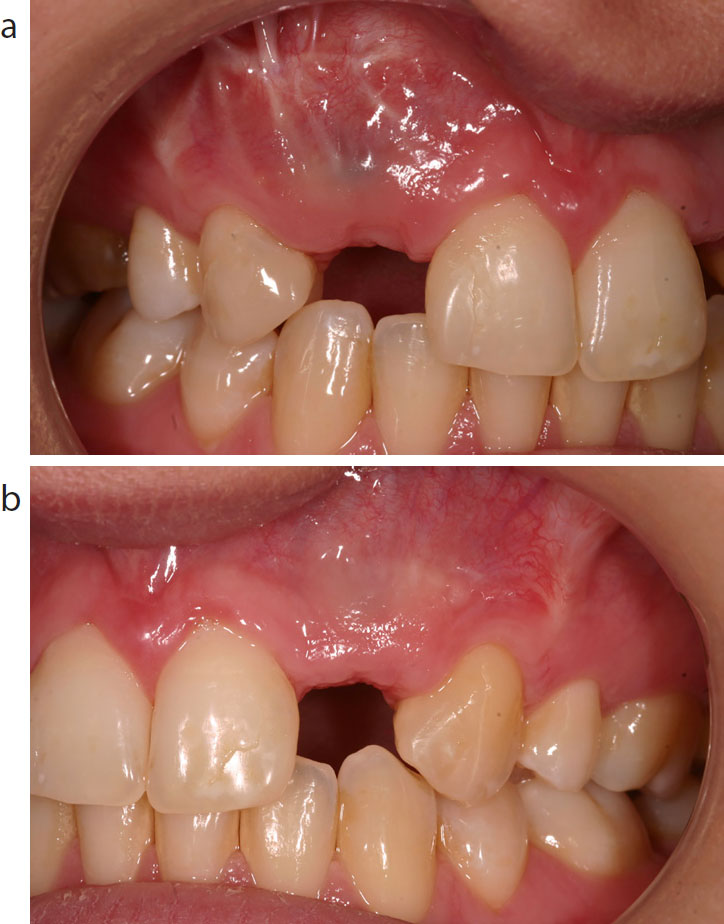
Failure to achieve the ideal horizontal and vertical spatial relationships can lead to problems. Horizontal misalignment within the buccal plane may increase the risk of alveolar bone loss3,4 and mucosal recession2,5,6 (Figure 1). In contrast, palatal placement risks an inferior emergence profile of the prosthetic crown.7 Inappropriate mesial-distal implant position may also affect the shape and size of the interproximal papilla,8 with failure to achieve a 1.5–2 mm peripheral bone margin, resulting in loss of the papilla height, reduced thickness of the gingival collar and an undesirable embrasure form and emergence profile.
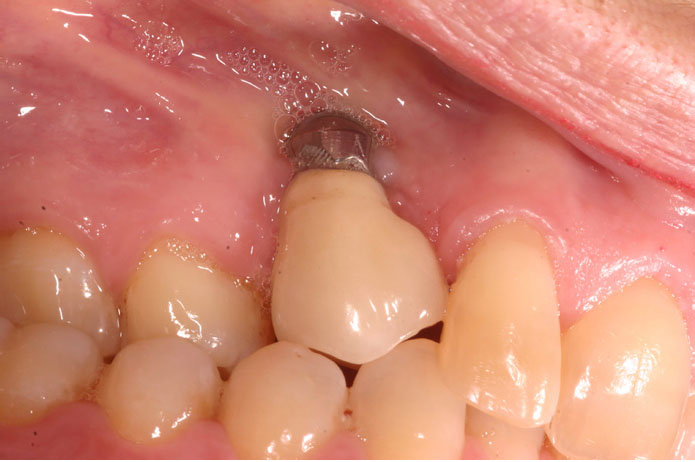
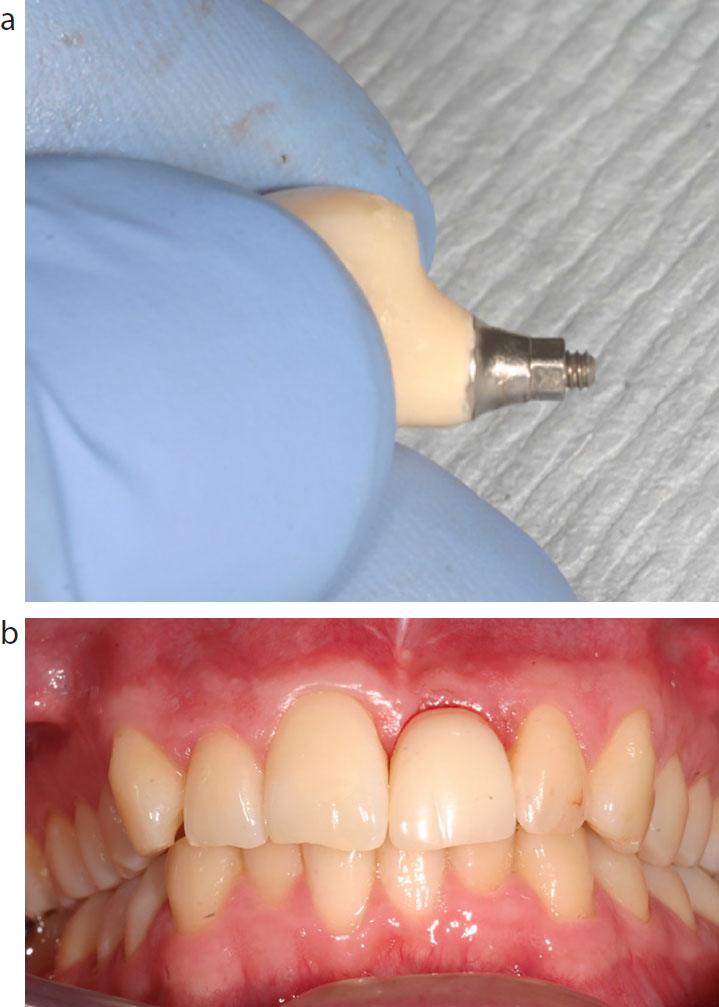
Figure 1. UR3 implant placed too deep and in too buccal a position with subsequent soft tissue recession and metal abutment show.
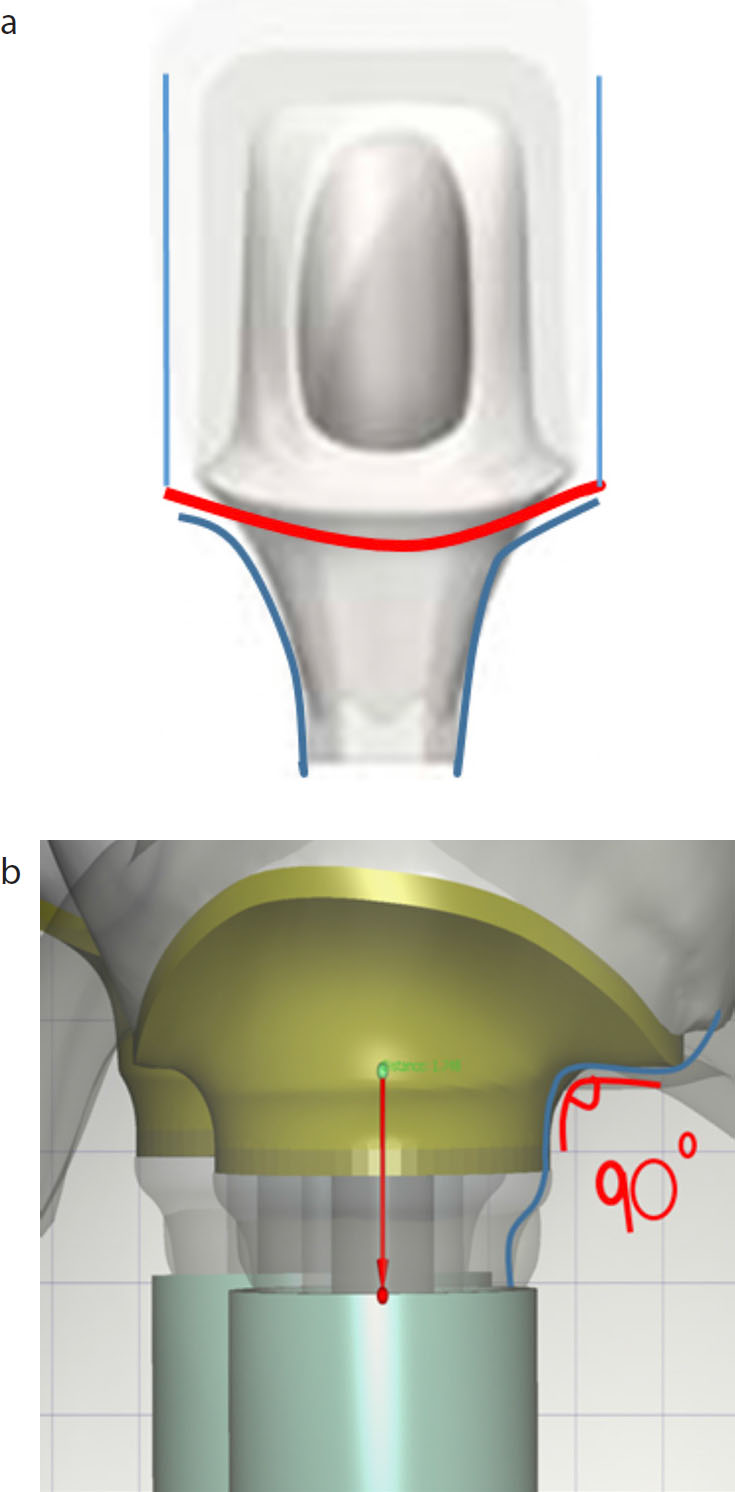
With regards to vertical apical-coronal malpositioning, deep implants (>2 mm) can result in an increased risk of bone resorption, tissue shrinkage, a compromised aesthetic outcome and long-term maintenance issues.9 Conversely, superficial fixture placement (<2 mm) can also lead to aesthetic complications as it may create a more acutely angled emergence profile of the prosthetic restoration and risk exposure of the abutment and possibly the fixture10 (Figure 2).
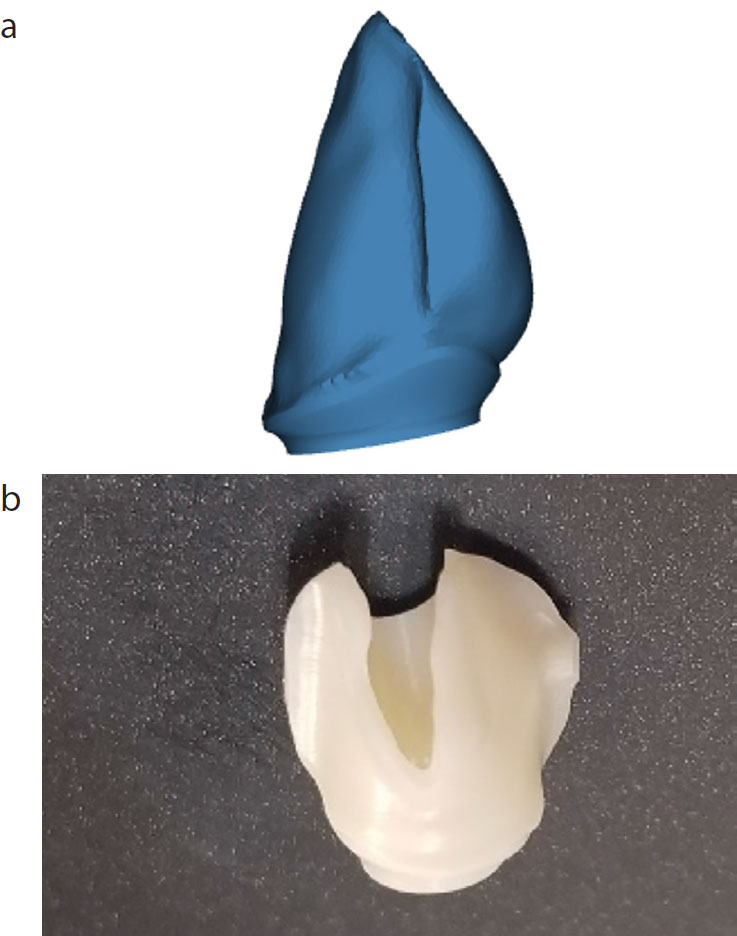
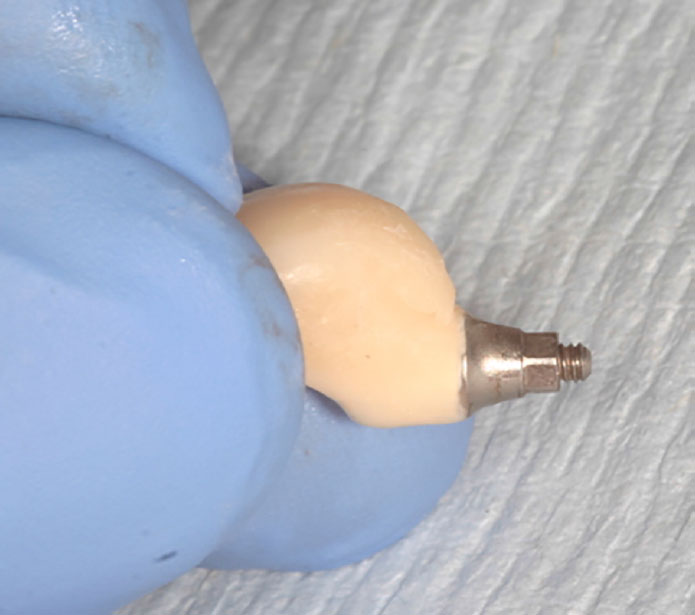
Figure 2. (a, b) These CAD images illustrate two different emergence profiles resulting from implant placement. The abutment in (a) has a tapered design (marked in blue), leading to the emergence at the mucosal margin (marked in red). The abutment in (b) has been placed too shallow and has resulted in an abrupt crown margin emergence (measured as 90°). Such an angulation may impinge upon the aesthetics of the crown emergence and creates a plaque trap that impacts upon the implant mucosal health.
Comprehensive patient assessment and treatment planning, in combination with a good surgical technique, can normally mitigate against the risk of implant malposition. A diagnostic wax-up of the final prosthetic restoration can help determine not only the ideal shape of the restoration, but also optimally guide the implant position. However, despite meticulous planning, the ideal fixture position may be inherently compromised by the presence of adverse anatomical features (neurovascular bundles, maxillary sinus, adjacent teeth alignment) or alveolar bone and soft tissue defects, resulting in a challenging prosthetic reconstruction. The early identification of cases, where the prosthetically-driven protocol cannot be followed, allows for investigation of different prosthetic solutions. Close liaison with the dental laboratory technician at this stage can ensure that the subsequent prosthesis is both harmonious with the mucosal tissues and aesthetically acceptable, minimizing the risk of longer-term prosthetic and peri-implant complications.9
This article uses clinical cases to present both clinician and dental technician with solutions for implants placed in sub-optimal positions.
Soft tissue strategies
The consequences associated with implants placed in a sub-optimal position are particularly severe in the aesthetic zone and can be further complicated when the individual has a thin and scalloped biotype, a tapering tooth form11 and less than 2 mm of keratinized mucosa (KM).12 It has been suggested that patients with a thin scalloped biotype require placement of the implant shoulder more palatally, in order to reduce the risk of titanium show through,13 but this may be at the expense of the ability to construct an optimal prosthetic emergence profile.
Simple management of a buccal placed implant may involve the use of a two-stage protocol, which aims to distribute the residual mucosal tissue electively. In the maxillary area, the alveolar crestal secondary stage incision can be placed palatally and the reflected flap displaced towards the buccal aspect of the fixture. This protocol promotes the retention of keratinized mucosa, at an adequate tissue thickness around the implant neck. However, primary closure may sometimes be difficult after this procedure, as it can be dependent on the tissue thickness and the extent of the displacement. Delayed healing by secondary intention, with increased risk of recession to the adjacent teeth, can result if the tissues cannot be closely approximated.
A variety of surgical peri-implant mucosal augmentation techniques have been promoted, with the aim of either improving the prosthetic emergence profile of the restoration and/or reducing the risk of soft tissue recession.14 These techniques attempt to increase either the volume of connective tissue at the site, resulting in increased vascularity to the region and enhancement of the body's regenerative response,15,16 or the development of a more robust and stable zone of keratinized mucosa. Reported augmentation techniques are wide-ranging and include the use of autogenous tissue-free gingival grafts (FGGs),17 connective tissue grafting (CTG),18 xenogenous (porcine-derived products such as MucoGraft®19) or allografts (Alloderm®). Although opinions on the optimal soft tissue augmentation approach differ, the use of autogenous grafts (CTG/FGG) has been found to be effective at increasing the mucosal thickness and KM.20
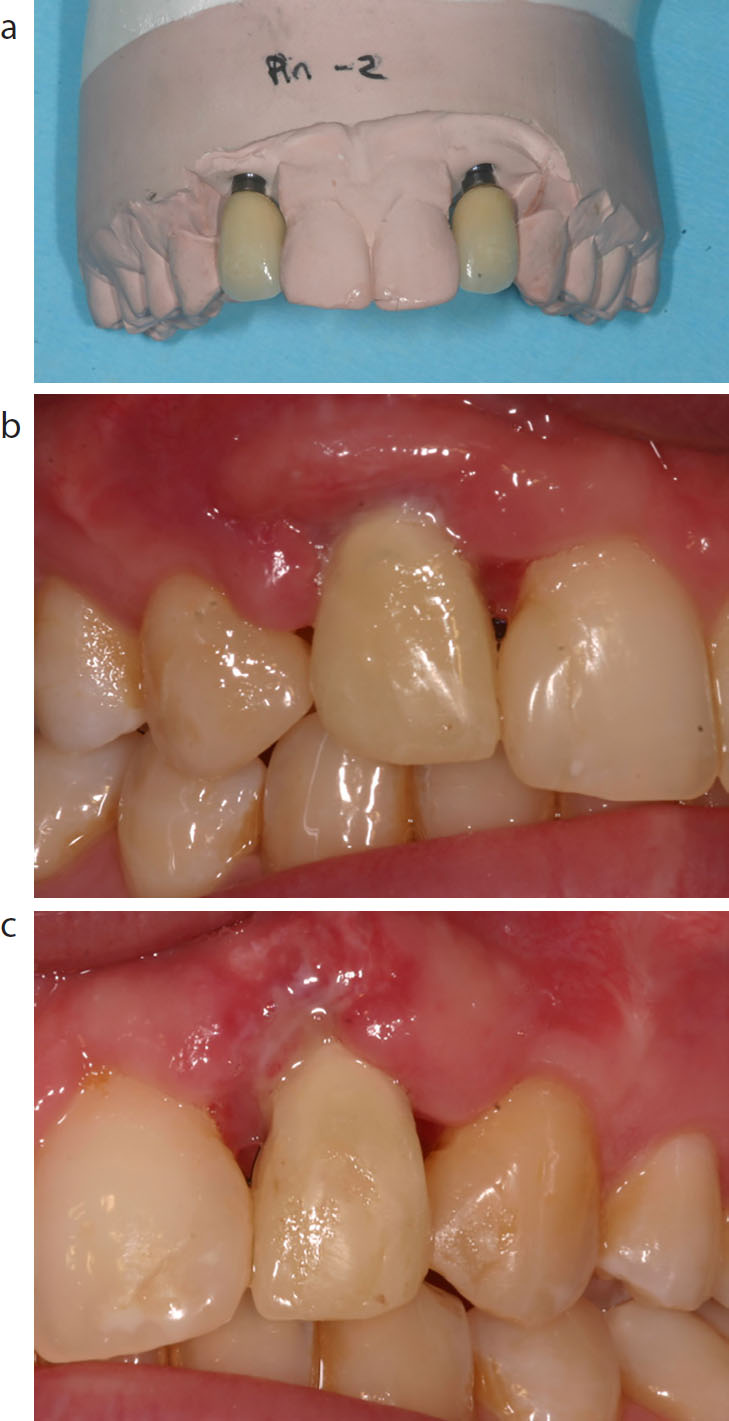
The early identification of implant fixtures, positioned with an angulation that may predispose to soft tissue loss, is crucial for early intervention to promote successful management. Case One (Figures 3–6) details the use of an apically repositioned flap in combination with a FGG, to increase the KM and improve soft tissue health around two buccal-orientated implants.
Figure 3. (a, b)
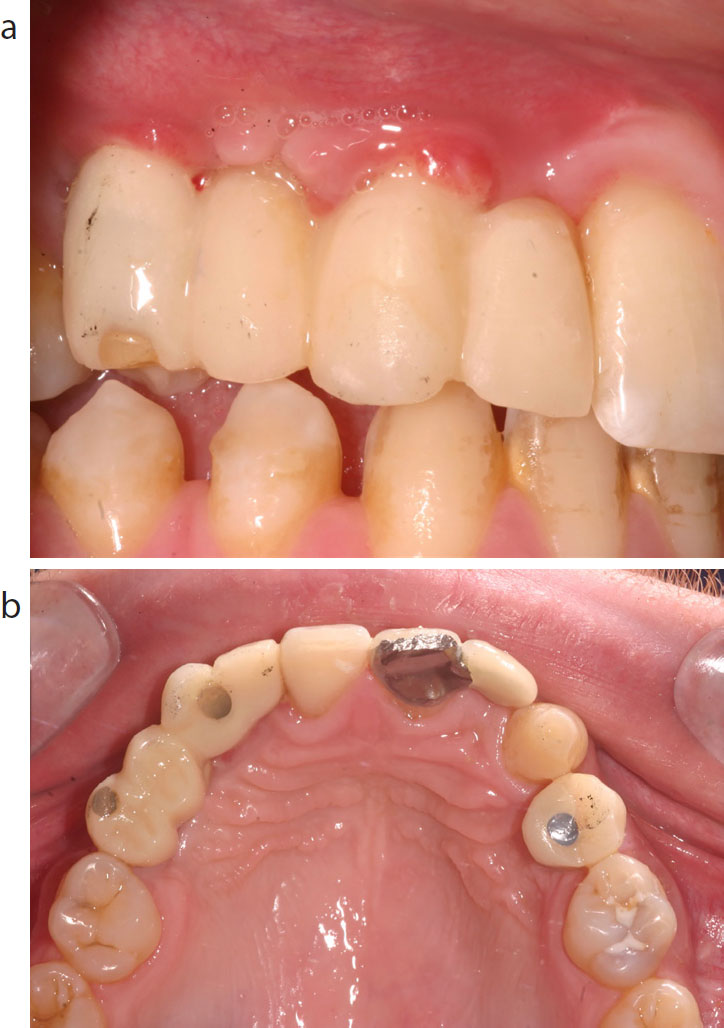
Case 1: This hypodontia case illustrates failed block bone grafting with resultant vertical and horizontal bone defects that necessitated buccal angulation of both the UR5 and UR3 fixtures. Subsequently, the provisional restorations can be seen to have a reduced band of KM and the mucosa is erythematous and oedematous.Figure 4. (a, b)
Case 1: To stabilize the peri-implant soft tissues, an FGG was harvested from the palate and sutured onto the buccal aspect.Figure 5. (a, b)
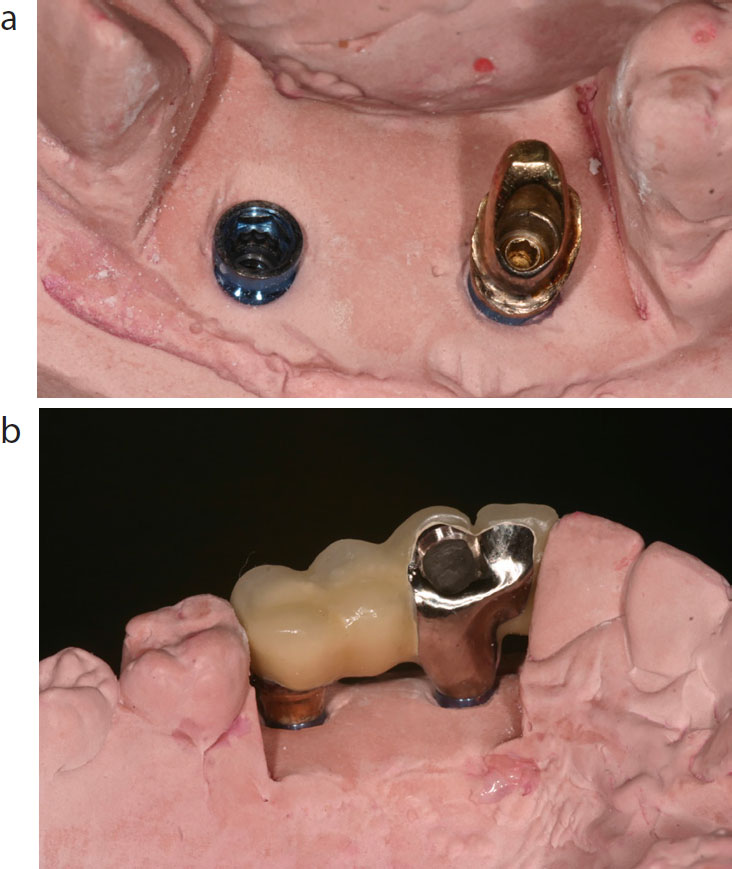
Case 1: The definitive restoration was a hybrid bridge with screw retention on the UR3 implant and a gold cast custom abutment, with a margin lying 0.5 mm below the soft tissue collar, for the UR5 fixture.Figure 6.
Case 1: The final outcome shows improved peri-implant soft tissue health associated with the increased width of KM around the implant-retained bridge. However, the limitations of the buccal angulation of the implants with metal show at the neck of the UR3.
Prosthetic management at second stage surgery: abutment selection
Temporary abutments include cover screws, healing abutments and provisional crowns. Surprisingly, little research is available to guide the clinician on appropriate abutment choice, with most guidance originating from case reports or manufacturer guidelines. Conventional parallel-sided healing abutments have been augmented with a range of contoured, aesthetic or adjustable abutments that aim to improve soft tissue adaptation around the coping during early healing. Such contoured healing abutments may mitigate against the risk of soft tissue recession around implants positioned with an increased buccal emergence. Alternatively, enhanced soft tissue healing can be achieved by using same-day provisional crowns, provided chairside or through the laboratory, if close support is available. The early use of provisional crowns has been found to improve the mucosal profile around the definitive prosthetic structures.21,22 Adaptation and individual molding of the provisional crowns (see Case Two) can be an effective means of preserving and manipulating the soft tissues until the desired mucosal emergence profile and papilla contours are achieved.23
Case Two details a clinical example of implants that were labially angulated due to lack of bone (Figure 7). Clinical options to manage the case included explantation and repositioning of the implant or, as detailed, soft tissue augmentation at second stage surgery using the combination of immediate provisional crowns (Figure 8a) and a roll-flap connective tissue graft (Figure 8b and c). The definitive management of the case employed UCLA cast custom abutments with cement-retained crowns. Despite the aesthetic compromise, the mucosal tissues were stable at the 2-year review (Figure 9).
Figure 7. (a, b)
Case 2: This case details incorrectly placed implants within the UR2 and UL2 sites with subsequent labial mucosa shine through of the implant collar.Figure 8. (a–c)
Case 2: The case was managed using a CTG roll-flap technique, with connective tissue rolled from the palatal to the buccal aspect and same-day laboratory manufactured provisional crowns. This avoided the need for the placement of healing abutments that may have encouraged soft-tissue recession.Figure 9.
Case 2: The 2-year review shows a thick soft tissue collar around the crowns, masking the underlying implants. However, the custom abutments were unable to disguise the poor positioning of the implants, with the emergence of the crowns lying apical to the gingival zenith of the adjacent central incisors. Alternative treatment options would have been explantation with block bone grafting to facilitate improved positioning.
Definitive restoration
The definitive implant restoration can be manufactured as either a one-piece screw-retained structure starting at the implant level, or in two components, using an angulated or custom abutment and cemented crown. Although both techniques are successful, the use of an angulated abutment allows the clinician to use a variety of abutment orientations to support the prosthetic structure. Influencing factors include: the type of implant (bone level or trans-mucosal designs), the implant configuration (internal or external hex), divergent implant direction, the available restorative space, aesthetic demands and desired prosthetic outcome.
Implant level abutments
Dental implant fixtures can be restored with screw-retained or cement-retained crowns, with each technique having individual advantages and disadvantages. The major benefits of screw retention include a reduction in the inter-occlusal vertical space required for restoration and simplification of prosthetic retrieval. Retention of an access foramen may, however, be at the expense of impaired control over occlusal contacts.24
Successful planning for screw-retained restorations requires the adoption of a prosthetically-driven surgical protocol, where the vertical screw access emerges within the cingulum envelope of the implant crown (anteriorly) (Figure 10) or inter-cuspal fossa (posteriorly).
Figure 10. (a, b) Screw-access channel lying within the cingulum plane of a canine crown. This position negatively impairs the technician's ability to contour the crown effectively to provide both an occlusal contact and dynamic guidance.
Within the aesthetic zone, adoption of this protocol can result in the implant being palatally positioned in the alveolar ridge, with the requirement to use a labially cantilevered crown, to achieve alignment in the arch. Cantilevering the crown in this manner can increase the difficulty associated with creating a natural emergence profile, particularly when the technician attempts to recreate a desired ‘triangular’-shaped anterior crown against the circular cross-sectional shape of the dental implant. Again, the use of provisional crowns, with additions or alterations, can help manipulate the soft tissue collar until the desired emergence profile is achieved (Case Three: Figures 11–13). The preferred soft tissue contour, produced by the provisional restoration, can then be captured with either an impression coping customized through the addition of a composite material (Figures 14 and 15), or through a direct impression of the provisional crown emergence surface. Both techniques allow the developed soft tissue profile to translate directly into the definitive restoration (Figures 16–18). Small subsequent changes in emergence profile are well tolerated by the mucosal tissues in most circumstances, resulting in transient blanching of the adjacent soft tissues which normally resolves after a few minutes. Large changes to the emergence profile may promote apical displacement or recession of the mucosal tissue and unwanted aesthetic gingival changes.
Figure 11.
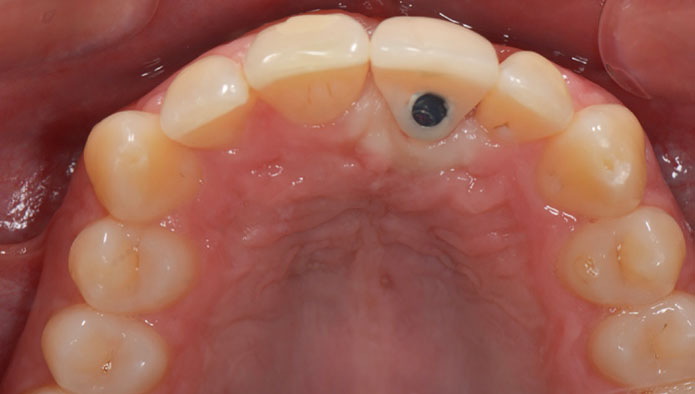
Case 3: Conventional screw-retained implant placement in UL1 site with access cavity within the cingulum of the restoration.Figure 12.
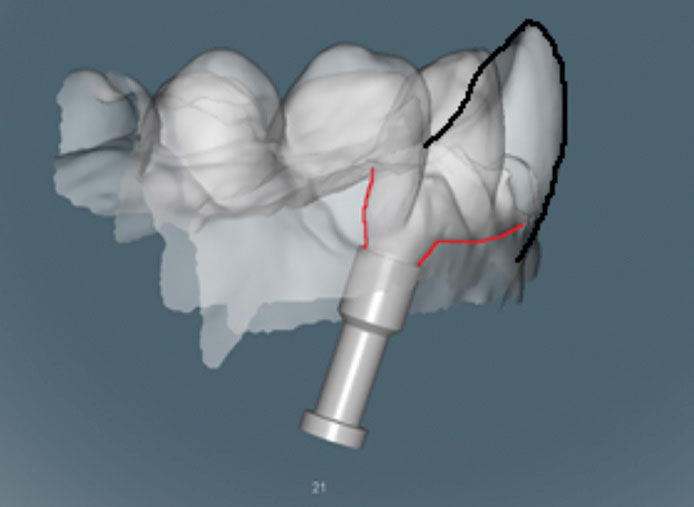
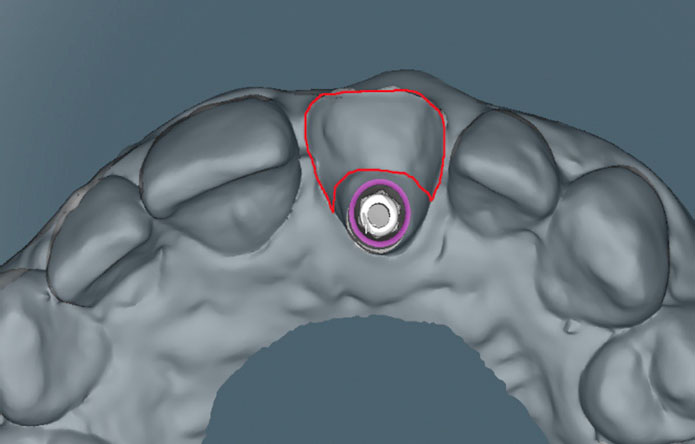
Case 3: The shallow placement of the implant has challenged the emergence profile as illustrated by the dimensional disparity between the ‘red’ line of the emergence profile and ‘black’ line of the ideal crown shape.Figure 13. (a, b)
Case 3: The subsequent provisional crown had a labial cantilever of labial crown margin and a poor emergence profile, with the soft tissue collar lying below the gingival margin of the adjacent UR1 tooth.Figure 14. Addition of composite to the provisional restoration until a satisfactory emergence was achieved.Figure 15. Addition of composite onto an impression coping to capture the emergence profile.Figure 16. The emergence of the provisional profile was subsequently copied and captured within the definitive digital model (outlined in red) constructed screw-retained crown.Figure 17. Translation of labial emergence profile from adjusted provisional to definitive crown.Figure 18. Improved aesthetics achieved by adjusted emergence profile of definitive crown.
The use of angulated abutments and cement-retained crowns can facilitate restoration of implants that are not restorable via conventional screw retention. In addition to purported improved aesthetics, cement retention may add a stress-breaking cement interface between the crown and abutment, reducing the risk of damage to the implant. Abutments for cement-retained crowns can be either prefabricated standard abutments or custom made, where they are designed to promote an idealized mucosal peri-implant collar.
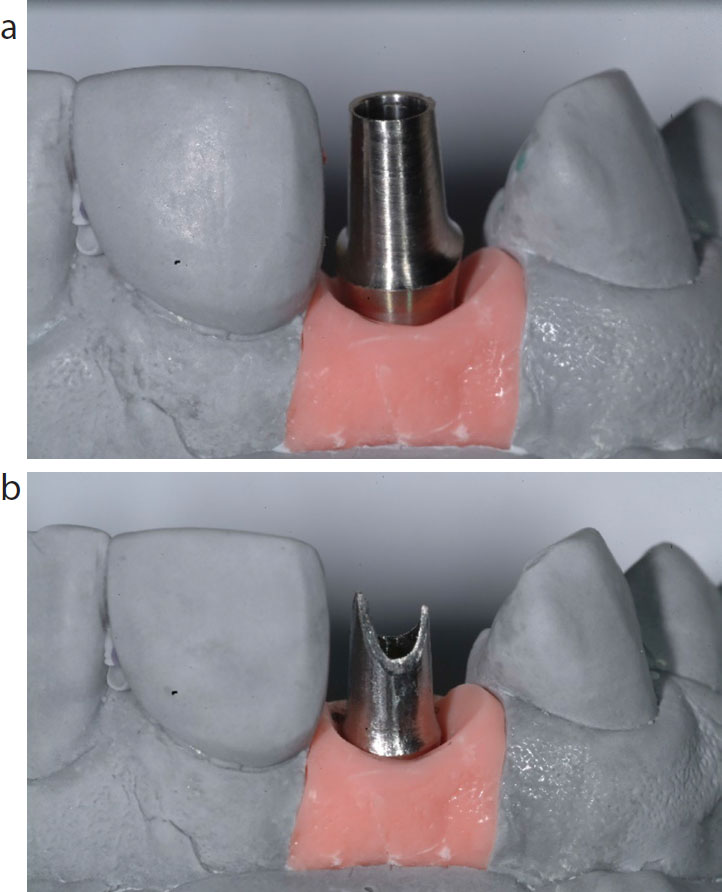
Stock/standard abutments are relatively inexpensive and are available in an array of angle-correction sizes (ranging from 12°–30°), to simplify the prosthetic manufacturing process. However, their use is limited, as they can only be used when their design correlates with the requirements for the abutment margin and its relationship with the mucosal tissue collar (Figure 19). Sometimes, significant angle correction, in combination with a superficial implant fixture placement, can result in visibility of the abutment structure affecting the aesthetics of the prosthetic restoration. Use of standard angled abutments can also result in a deep abutment/crown interface that predisposes to both sub-gingival cement extrusion and an uncleansable junction, with increased risk of peri-implant disease.
Figure 19. (a, b) Stock abutment with inappropriate marginal height, lying above the mucosal collar (Figure 9) and post-technician adjustment.
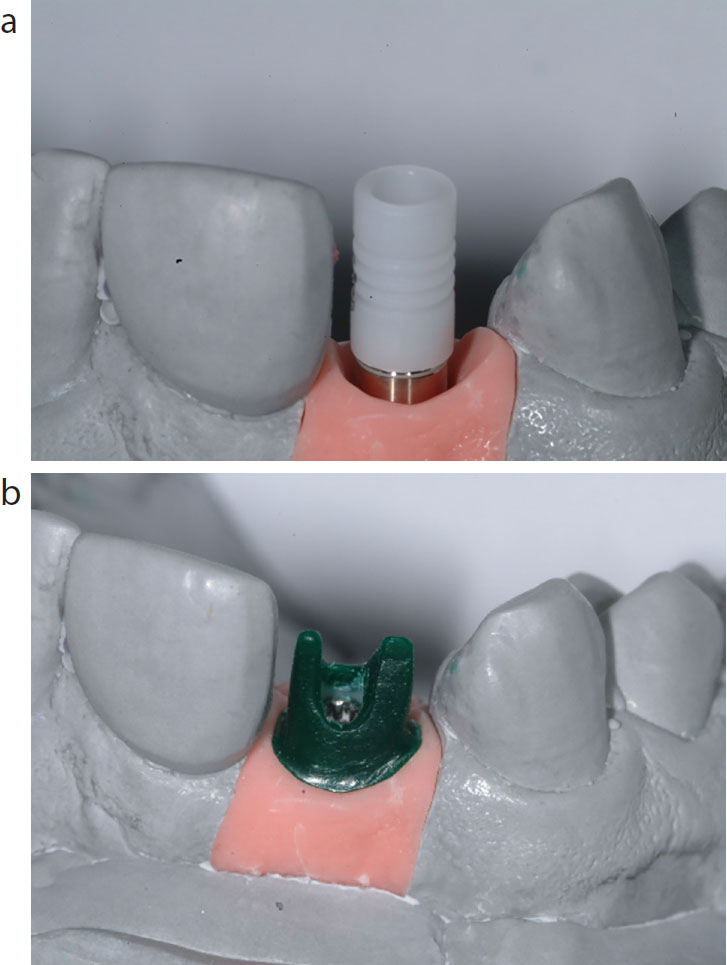
In contrast, custom abutments can limit the risks associated with the creation of this interface, through the manufacture of an abutment/crown margin that lies 0.5 mm to 1 mm below the peri-implant mucosal collar (Figure 20). Custom abutments can also help to manage the complex 3D emergence profile requirements, when implant fixtures have been placed too deep or shallow.
Figure 20. (a, b) UCLA in process of wax-up.
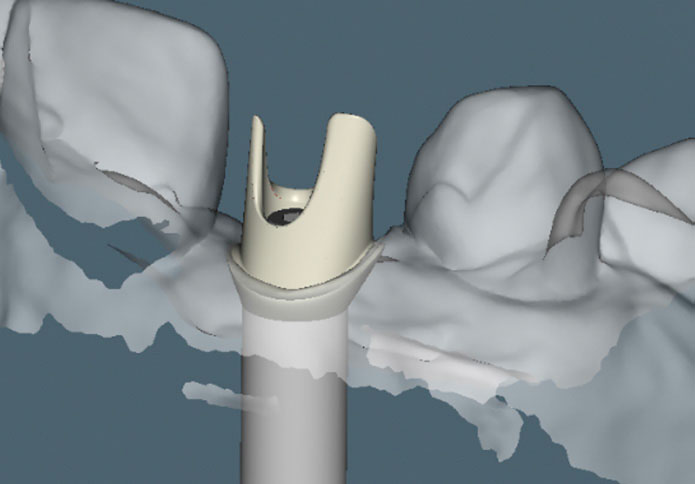
Custom abutments may be waxed-up and cast (UCLA) or manufactured using CADCAM processes (Figure 21). Cast custom abutments have good survival rates,25,26 predictability and can allow the crown to be cemented with a provisional cement, aiding retrieval if required. However, their use is more expensive, owing to the high costs associated with the components and cast metals, in addition to their labour-intensive manufacture.
Figure 21. CADCAM design of same abutment.
CADCAM abutments retain many of the benefits of cast custom abutments but are cheaper and, from a laboratory perspective, more time-efficient to construct.27 CADCAM also facilitates the use of additional materials such as zirconia, titanium and cobalt chromium. Zirconia has been viewed as an attractive sub-structure material as it has excellent strength, comparative marginal fit and aesthetic properties.28 Its use in situations involving patients with thin mucosal tissues or a higher risk of recession has been seen as advantageous as its white coloration can mask unwanted aesthetic changes. However, concerns have also been expressed relating to potential damage to the implant hex through micro-movement fretting of the harder zirconia on the softer titanium alloy of the implant.29 In addition, fractures of zirconia abutments have been reported when it is used in thin sections.30
Angle correcting implants and abutments
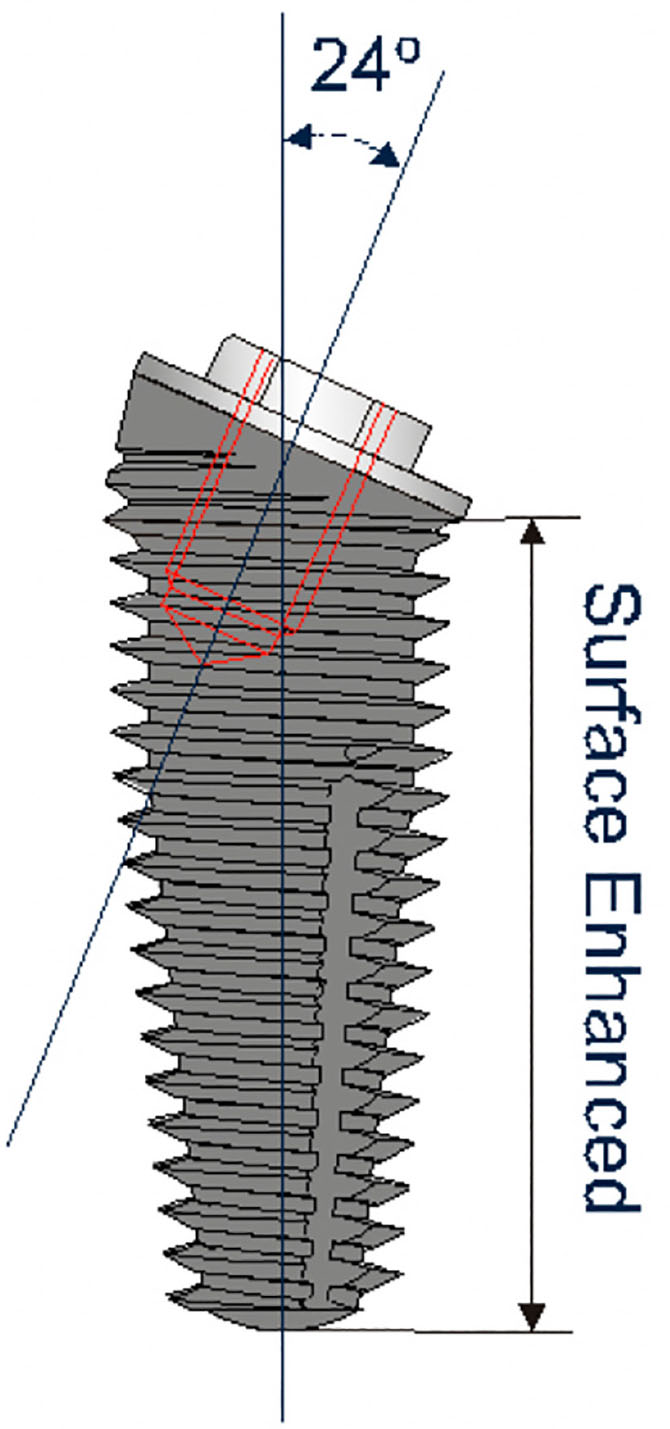
Implant companies have sought innovative solutions to the conundrum of merging the biological benefits achieved when adopting a cement-retained implant placement orientation and the benefits of a screw-retained prosthetic solution. Implants with angled prosthetic correction of 12, 24 and 36 degrees (Co-Axis®, Southern, Centurion, RSA) offer solutions to optimize placement within bone whilst retaining screw-retained retrievability (Figure 22).
Figure 22. Co-Axis® implant with prosthetic angle-correction.
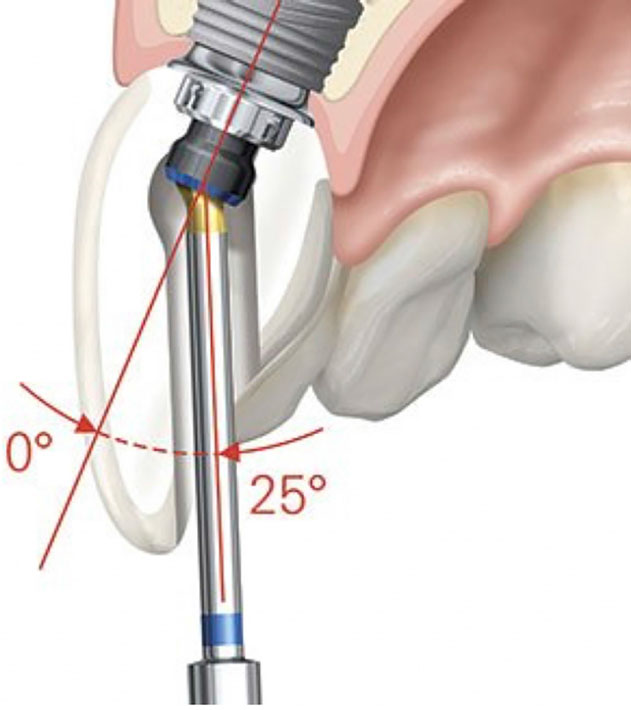
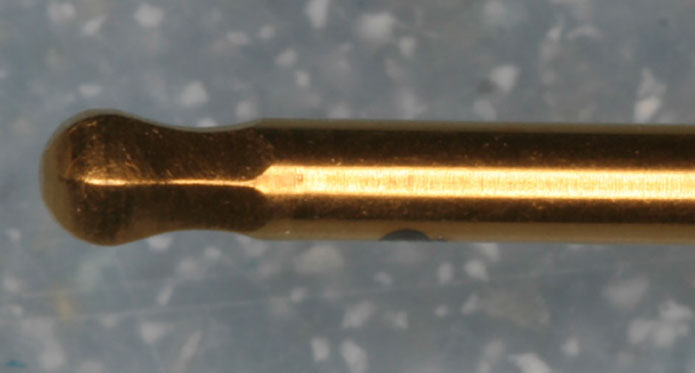
Recently, manufacturers have introduced a modification to the retaining screw head, allowing a matching screwdriver to engage with the head at an angle tilted to 25 degrees from the path of screw insertion (Figures 23 and 24). Such systems may allow the implant to be placed in the ideal buccal-lingual direction to optimize aesthetics whilst retaining the benefits of screw-retained retrieval. In addition, the flexible nature of these systems allows metal interface with the implant and zirconia substructure to support the restoration, redressing the reported problems with implant/zirconia interfaces (Figure 25).
Figure 23. Nobel® angulated screw channel.Figure 24. Head of an angled screw-driver (Neoss®, Harrogate, UK).Figure 25. Two part zirconia with metal base held to the implant by the Nobel Biocare Omni® screw.
Multi-unit abutment restoration
Multi-unit abutments can facilitate restoration of multiple divergent implants with both fixed and removable prostheses. Multi-unit abutments are stock components and generally allow angle correction of between 12 and 30 degrees, in full-arch, implant-supported restorations. They are used as a transitional or intermediate component, to establish a common screw orientation of the abutment structure at a preferred vertical level to facilitate restoration of the patient. Their use has been found to be associated with longstanding bone stability31 and allow for simplified prosthetic outcomes.32
Multi-unit abutments once fitted, are left in situ, with subsequent impressions and fit of the prosthetic components occurring at the newly determined transitional abutment level. The increased height of the abutment platform increases visibility and ease of access to the prosthetic interface, whilst reducing the risk of trauma to the peri-implant mucosal collar during the rehabilitation pathway. The reduced need to disrupt the mucosal margin may be of particular benefit in patients with reduced KM, for instance, in implant-supported over-denture cases. In addition, the use of these components allows the clinician to check the seating of impression copings visually and check-jigs on the abutments, making impression-taking and cast-verification simpler. Patient comfort may also be improved, with reduced requirement for local anaesthesia at the clinical stages of prosthesis construction and easier cleansability.
The major limitations associated with the use of multi-unit abutments relate to the requirement to use smaller diameter retaining screws, that have reduced maximum torque value (with increased risk of loosening of the superstructures) and the requirement for sufficient inter-arch vertical restorative space, to house both the multi-unit abutment and the definitive prosthetic structure.
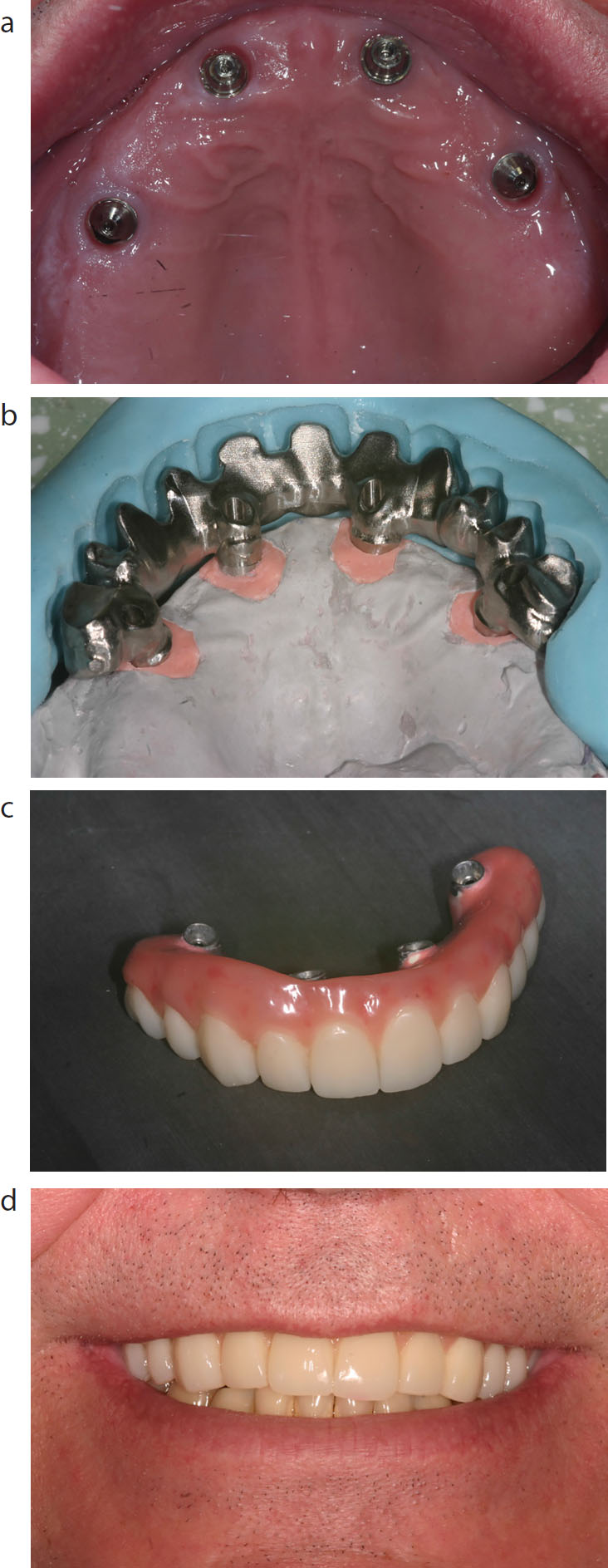
The use of angled multi-unit abutments have facilitated the development of novel approaches to full-arch reconstructions, such as All-on-Four™ (Nobel Biocare, Zurich-Flughafen, Switzerland) (Case Four: Figure 26). This approach facilitates the placement of larger implants in divergent orientations that avoid the anatomical limitations associated with the inferior dental nerve and maxillary sinus. The ability to place implant fixtures which do not conform to the prosthetically-driven protocol can help to avoid the needs for grafting procedures and can allow for longer but fewer implants to be used, reducing the subsequent cost to the patient.
Figure 26. (a–d)
Case 4: The use of multi-unit abutments to correct angulation from implants placed for an All-on-Four® rehabilitation (Nobel Biocare). The definitive CADCAM framework has employed mucosal-coloured composite to disguise the soft tissue loss and give the appearance of papilla.
The replacement of extensive vertical or horizontal alveolar/mucosal tissue defects cannot always be easily managed with bone and soft tissue grafting procedures. If the tissue loss is accepted, then the prosthetic structure may need to cope with an increased inter-arch distance, longer teeth, a reverse smile line, rectangular tooth forms, inverted tooth axes, and lack of support for the upper lip.
Alternatively, dental technicians can use an array of techniques and materials (including pink ceramic, acrylic or composite) to replace gingival tissues. Small defects (single or two-unit cases) can often be simply managed using small additions of pink ceramic (Case Five: Figure 27) or larger teeth compensating for reduced proximal tissue. More severe defects, involving multiple implant sites, may include sizable composite layering techniques as detailed in Case 4 (Figure 26). Hybrid techniques, such as the use of a mucosal coloured screw-retained base with individual cemented crowns, have also been advocated as a means of replacing larger defects, whilst reducing the maintenance burden. Such prostheses require careful liaison with a technician to ensure that the substructure design is: cleansable, provides support for the overlying materials to enable replication of the gingival form and that sufficient intra-arch distance space remains to allow placement of suitably sized teeth.
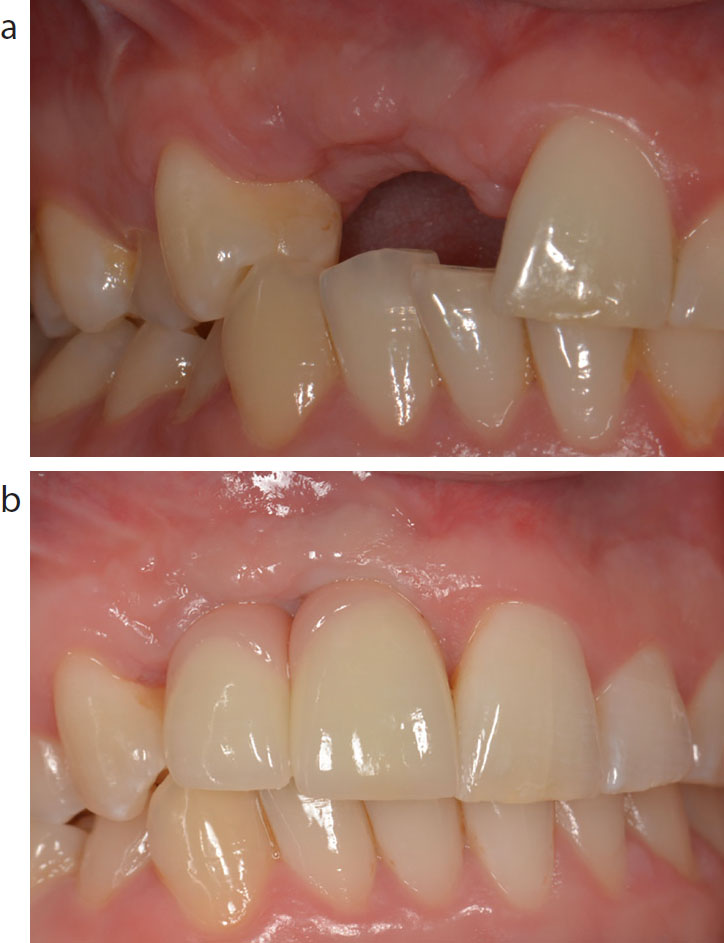
Figure 27. (a, b)
Case 5: Use of mucosal-coloured porcelain to disguise loss of inter-dental papilla.
Explantation
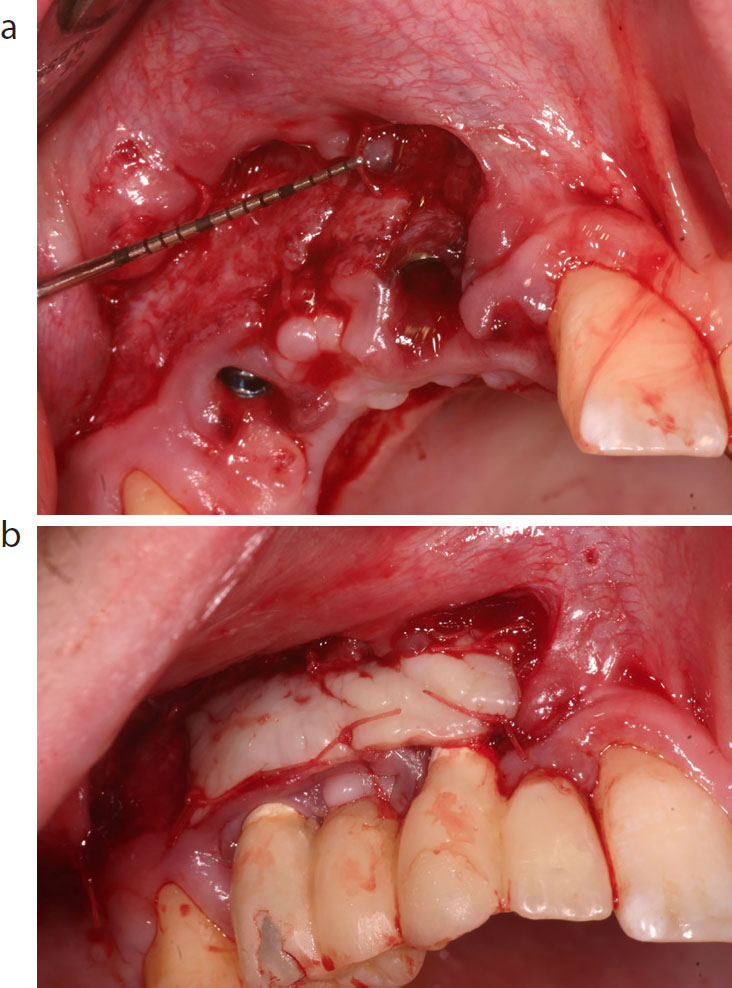
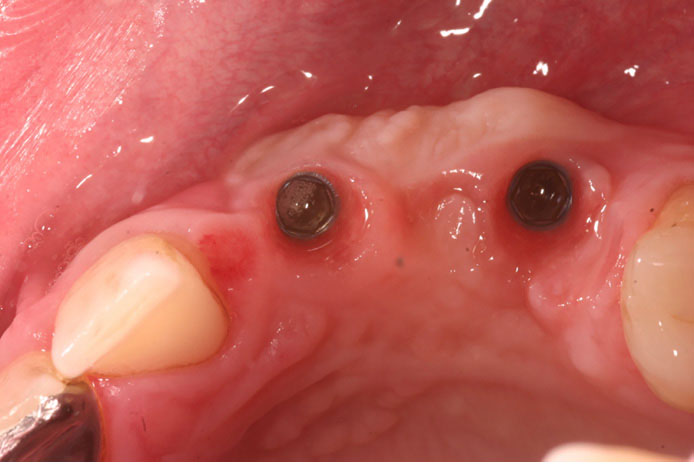
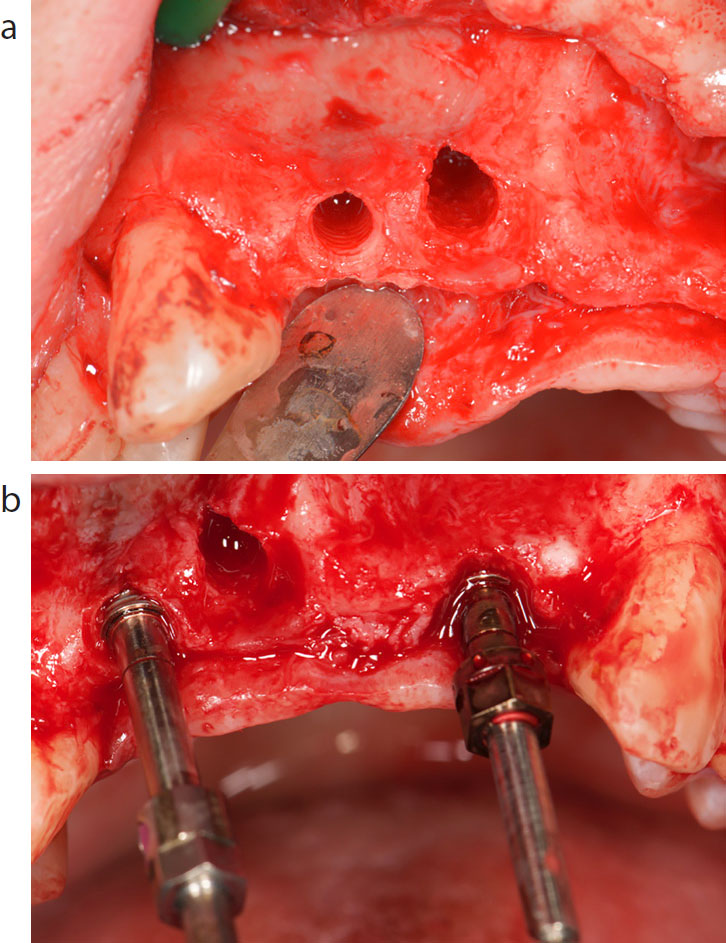
Historically, removal of unrestorable dental implants was challenging, often involving significant bony trauma. The introduction of implant removal kits has simplified explantation and allows removal of fixtures with minimal destruction to the surrounding bone tissues. In cases (Case Six) where sub-optimal implant placement has compromised the immediate or longer-term outcomes (Figure 28), explantation (Figures 29 and 30) and placement of new implants may be a preferable solution (Figure 31). However, these kits cannot be used in situations of abutment screw fracture or damaged fixture head.
Figure 28.
Case 6: This case shows unrestorable implants within the UR1 and UR2 sites.Figure 29. (a, b)
Case 6: The implants were explanted using 3i BioMet® (Palm Beach, Fl, USA) Implant Removal Kit and a further two implants placed.Figure 30.
Case 6: 3i BioMet® Implant Removal Kit.Figure 31. (a, b)
Case 6: Definitive screw-retained prosthesis restoring the implants.
Deep uncleansible periodontal pocketSoft tissue recessionPeri-implantitis
Increased abutment lengthRisk of abutment exposure
Manufacturing a tapered abutment to achieve a natural emergence profile.
Gauging the correct amount of pressure that the abutment/restoration can apply to the soft tissue (biotype is difficult to determine from models).
A removable soft tissue model is required.
Shallow (<1 mm peri-implant pocket)
Unsatisfactory emergence profileRisk of implant exposure
Achieving contact points that manage the papillae to reduce the aesthetic limitations posed by dark triangular spaces.
Managing an acute emergence profile angle.
Buccal
Mucosal recession
Mucosal shine through of implantUnsatisfactory emergence profile
Managing the aesthetics of the prosthesis labial face – the reduced space often leads to over contouring of the restoration.
Managing the alignment of the prosthesis in relation to the surrounding dentition.
The creation of a greying of the mucosal tissues around the margin (if metal is used).
Palatal
Cleansability of pontic
Labial cantilever of crown
Hard to match emergence profile of teeth.
Gauging the correct amount of pressure that the abutment/restoration can apply to the soft tissue.
Intrusion of the abutment/restoration onto the palatal/lingual aspect leading to over-contour of the palatal restoration surface.
Implant treatment is a complex procedure with multiple factors associated with a successful functional and aesthetic outcome for the patient. Implant placement using an ideal prosthetic protocol is not always feasible and, in particular, may present challenges to the creation of an abutment that is in harmony with the soft tissues. Meticulous treatment planning and close liaison with laboratory technicians can ensure that successful outcomes can still be achieved in sub-optimally positioned dental implants.