Assessment and management of endo-periodontal lesions Philippa Hoyle Manoj Tank Somayeh Modarres-Simmons Claire Annabel Storey Dental Update 2024 46:10, 707-709.
Authors
PhilippaHoyle
BChD(Hons), MJDF RCS(Eng), MPros RCS(Ed)
Specialty Registrar in Restorative Dentistry, Department of Restorative Dentistry, Charles Clifford Dental Hospital, 76 Wellesley Road, Sheffield S10 2SZ, UK (philippahoyle1@hotmail.co.uk)
Endo-periodontal lesions present a number of challenges for clinicians. These include understanding their underlying aetiology, forming an accurate diagnosis and suitable prognosis and subsequently formulating an effective treatment strategy. This article aims to provide a summary of the literature available in the areas highlighted above, with particular reference to the recent joint American Academy of Periodontology and European Federation of Periodontology (AAP/EFP) world workshop for classification of periodontal and peri-implant diseases.
CPD/Clinical Relevance: This paper outlines important aspects a clinician must consider, including anatomy, a systematic methodology for assessment and introduction of the new classification of periodontal diseases in diagnosis. Prognosis and formulation of appropriate management strategies are explored.
Article
Philippa Hoyle
The new classification of periodontal and peri-implant diseases has retained the recognition of endo-periodontal lesions (EPLs) as a separate disease classification, due to the known pathophysiological differences from periodontitis, especially in the acute form, which includes its rapid onset and tissue destruction, as well as symptomatic presentation to the clinic.1
In general dental practice, there can be confusion unpicking the signs and symptoms in patients presenting with an EPL. Part of this uncertainty is deciphering whether the infection is endodontic or periodontal in origin. In all EPL cases, whether acute or chronic, there is a pathological communication between the periodontal and pulpal tissues, thereby resulting in more complex and challenging management. The anatomical variations in root canal morphology internally, including the presence of accessory and lateral canals and intricacy of the periodontium externally, provide challenging conditions for diagnosing and controlling bacterial infections. EPLs significantly negatively affect the prognosis of a tooth and present challenges for management, involving multiple treatment modalities.2
Prognosis is dependent upon an accurate diagnosis and this can be aided by a good disease classification system. The first reported classification of EPL divided the condition into five subcategories,3 however, subsequently this was adapted by Chapple and Lumley4 into the following categories:
Primarily endodontic in nature − when triggered by a deep carious lesion which is driven bacterially or trauma to the tooth allowing ingress of bacteria.
Primarily periodontal in nature − when periodontal destruction has exposed the pulp canal orifices and retrograde bacterial ingress to the pulpal complex is possible.
Combined perio-endo lesion − when both processes occur concurrently.
However, the recent joint American Academy of Periodontology and European Federation of Periodontology (AAP/EFP) world workshop for classification of periodontal and peri-implant diseases advised that a classification system based upon disease history was unhelpful for assessing the current clinical condition of the lesion,5 nor did it give insight in how to approach the treatment of such lesions. The new classification for EPLs is presented later in this paper and addresses these shortcomings.
By exploring the anatomy and pathophysiology of the EPL, systematically assessing such a lesion and diagnosing based upon the new classification, provides guidance to practitioners on their appropriate management.
Anatomy and pathophysiology
Periodontal and endodontic diseases are both of bacterial origin. It is the formation of a biofilm (aggregation of micro-organisms in an extracellular matrix attached to a solid surface) that increases the virulence of such bacteria. This is mainly due to the synergy, chemotaxis and production of endotoxins within a biofilm. The micro-organisms in EPLs are correlated with those involved in pulp and periodontal disease, particularly protease-producing anaerobic bacteria. The flora, together with their interaction with the tissues and the potential synergistic impact, are summarized in the sections below.
1. Pulpal effects on the periodontium
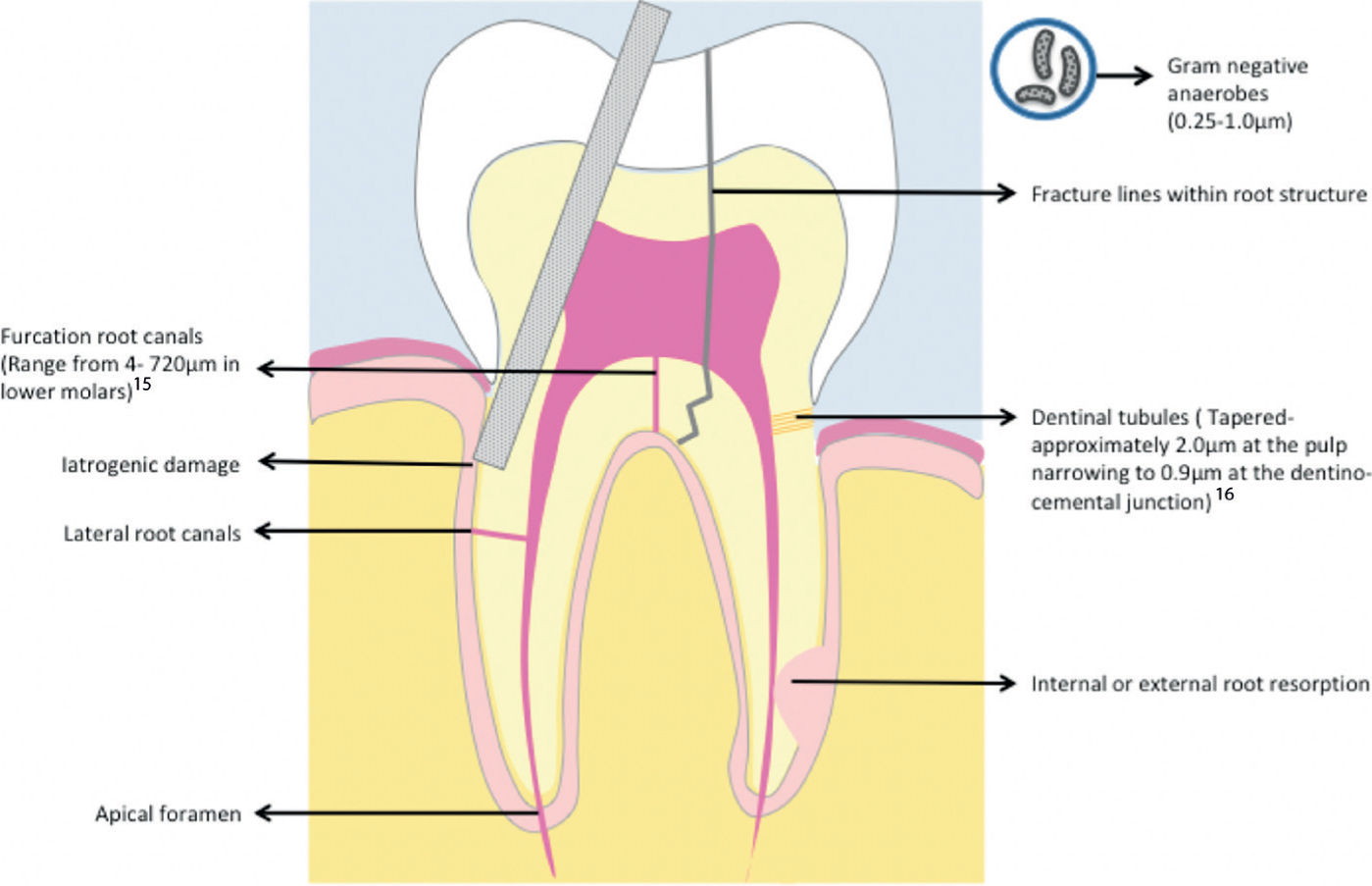
Endodontic lesions are thought to be polymicrobial yet less complex than periodontal lesions. Infected pulpal tissue has evidence of prominent anaerobic species that are similar to those seen in periodontal lesions, for example, Fusobacterium, Porphyromonas and Prevotella species.6,7,8 There is a close anatomical relationship between the root canal system and the periodontal environment (Figure 1). The periodontal tissues and the dental pulp are integrally linked together with communication possible via:9
Apical foramen;
Dentine tubules;
Lateral root canals;
Furcation root canals;
Fracture lines within root structure;
Iatrogenic damage.
Figure 1. Some of the potential pathways of communication between pulp and periodontium.
Lateral and accessory canals form during root development, often due to a break in the root sheath caused by the presence of periodontal vessels during the calcification stage. After development, they often become blocked or reduced in size. Some may remain patent, serving as additional pathways for the neurovascular supply of a tooth.
Accessory canals can be found all along the root and within the furcation, but the majority apically.10 De Deus found that 27% of 1140 extracted teeth had accessory canals, with molars most likely to have them, followed by premolars, then incisors and canines.11 This has been corroborated by various authors, with furcal canals present in 20−60% of molars,12 which are more likely to be patent.
There is ample evidence indicating that infection of the pulp can communicate with the periodontium at locations other than the apex of the tooth.13 In examining 100 teeth, Kirkham found that 23 had one or two accessory canals and, in two of these, the accessory canal was located in a periodontal pocket.14 Such lateral and accessory canals can act as pathways through which bacteria and toxic substances can be transported to the periodontium and induce inflammation. Clinically, teeth with furcation involvement and moderate bone loss should be assessed endodontically in case of infection via this route.
It must be remembered that, when a tooth has an apical abscess, drainage may occur through the gingival margin creating a communication, rather than draining through a juxta-apical sinus (Figure 1).
2. Periodontal effects on the pulpal tissues
Periodontal disease has a number of anaerobic bacteria associated with it including: Aggregatibacter actinomycetemcomitans (Aa), Porphyromonas gingivalis, Tannerella forsythia, Treponema denticola, and Prevotella intermedia, amongst others.
The question of whether or not plaque-induced periodontal disease may cause pulp tissue alteration is controversial. In recent years, observations have indicated that chronic periodontal disease induces or mediates pathological alterations in the tissue of dental pulp.17,18,19 Inflammatory cell infiltrate and tissue necrosis have been observed in the pulp adjacent to lateral canals and apical foramina, associated with infected periodontal pockets or exposure to the oral cavity due to recession.9,20,21 Secondary dentine formation in the root canal area has also been regarded as the result of pathologic pulp tissue reactions to periodontal disease.
On the other hand, it has been considered that periodontal disease, regardless of severity and plaque accumulation on root surfaces, does not affect the dental pulp.22 Pathologic pulp tissue alterations in periodontally sound teeth occurred as often as periodontally infected teeth, and it was concluded that the status of the periodontium does not exert any great influence on the pulp.23 No correlation has been confirmed between the severity of periodontal disease and the presence, or absence, of pulpal pathosis.24
The controversy is potentially attributable to the difficulty in accessing suitable control material, in which pathological pulp tissue alterations unrelated to periodontal destruction can be studied.
Patients who have been treated and maintained for chronic periodontal disease are likely to have been subjected to multiple treatments, some of which are now regarded as historic, and it is not uncommon to observe iatrogenic damage on exposed root surfaces from multiple root surface treatments. Handscalers (when sharp) remove more hard tissue and cementum than ultrasonic debridement or air polishing treatments, further compromising pulpal protection over time by decreased dentine width and potentially more lateral canal exposure.
3. How joint lesions occur
Endo-periodontal lesions are a result of communications between the pulpal and periodontal tissues through the routes described above, allowing transfer of microbial flora and by-products of the biofilm25 (Table 1). When two separate lesions meet on the same tooth a joint lesion is created. The literature suggests that, regardless of the lesion originating from the periodontal or endodontic tissues, or as a result of concomitant disease processes affecting the same tooth, the bacteria involved are comparable.1,12
Endodontic Disease
Potential Communications
Periodontal Disease
Polymicrobial
Apical foramen
Polymicrobal
Associated bacterial species:
Fusobacterium species
Porphyromonas species
Prevotella species
Dentine tubules
Associated bacterial species:
Aggregatibacter actinomycetemcomitans (Aa)
Porphyromonas gingivalis
Tannerella forsythia
Treponema denticola
Prevotella intermedia
Lateral root canals
Furcation root canals
Fracture lines within root structure
Root resorption
Iatrogenic damage
Classification
The classification of EPLs clinically informs the rationale behind the therapeutic strategy and treatment sequencing.
Historically, there have been numerous attempts to classify EPLs, often concentrating on the pathogenesis of the lesion, aiming to increase the efficacy of treatment provided by attempting to identify the primary source of infection. In reality, trying to identify the primary aetiology of such lesions is challenging, often impossible.
The AAP/EFP world workshop proposed a new classification system based upon current disease presentation using the signs and symptoms available which have a direct impact upon prognosis and management. This includes the assessment of the presence of fractures and perforations, whether it is a periodontitis patient, and the full extent of the periodontal tissue destruction around the tooth in question.
Table 2 shows the new classification of EPLs, adapted from Papapanou et al.1 The clinician must first determine whether the EPL is associated with damage to the root structure, iatrogenic or otherwise. Such lesions will usually have a poor prognosis and a restorability assessment is prudent to decide whether the tooth can be preserved.
Endo-periodontal lesion with root damage
Root fracture or cracking
Root canal or pulp chamber perforation
External root resorption
Endo-periodontal lesion without root damage
EPL in a periodontitis patient
Grade 1 – narrow deep periodontal pocket in 1 tooth surface
Grade 2 – wide deep periodontal pocket in 1 tooth surface
Grade 3 – deep periodontal pockets in >1 tooth surface
EPL in a non-periodontitis patient
Grade 1 – narrow deep periodontal pocket in 1 tooth surface
Grade 2 – wide deep periodontal pocket in 1 tooth surface
Grade 3 – deep periodontal pockets in >1 tooth surface
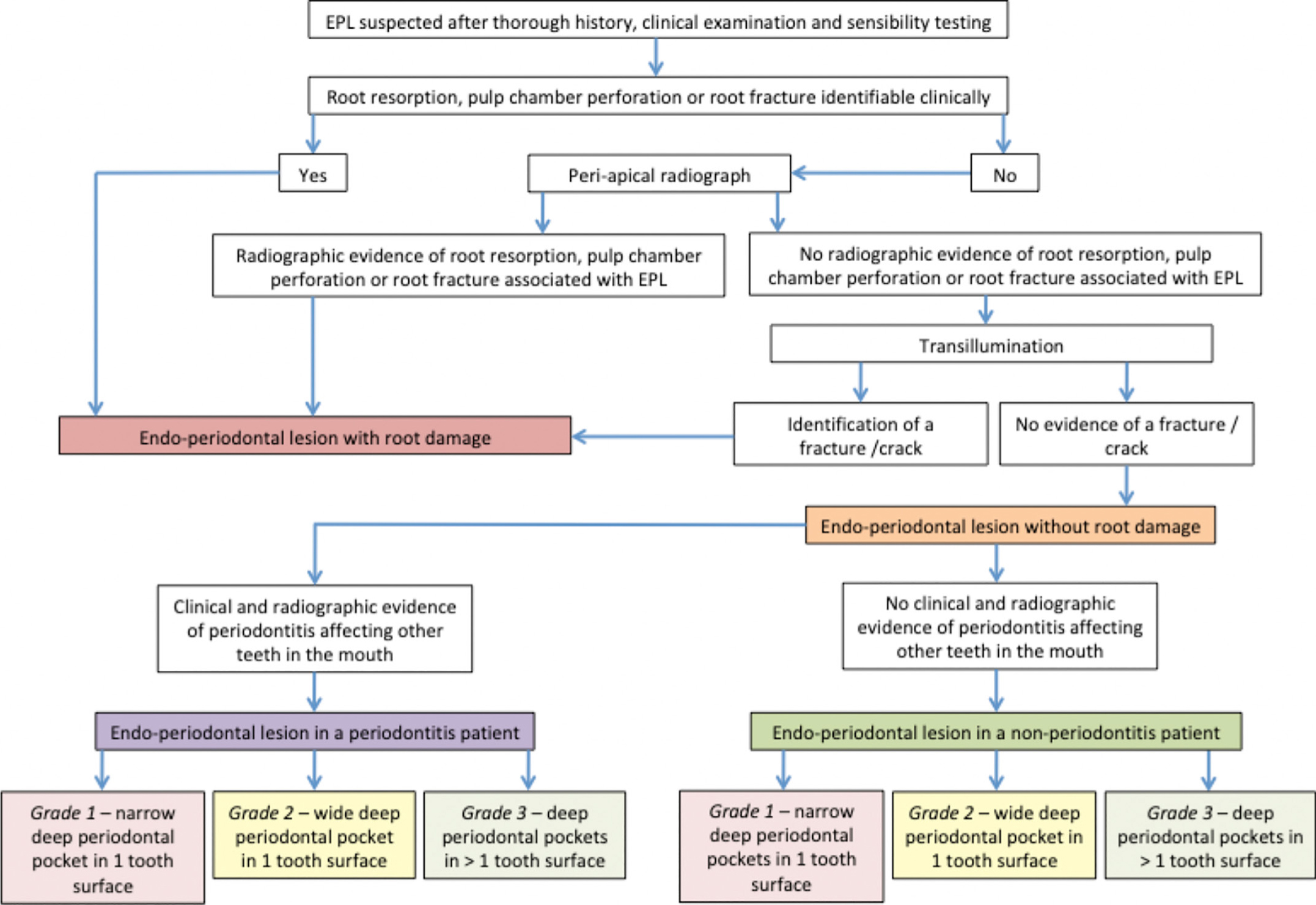
If there is no structural damage, clinicians must next determine whether they are dealing with a periodontitis patient or not. The lesion is then graded 1, 2 or 3, depending on the morphology of the periodontal pocket in the EPL. Figure 2 shows a flowchart to help clinicians arrive at a diagnosis based upon this classification system.
Figure 2. Flowchart to demonstrate systematic approach to achieve diagnosis based on new classification.
Following this systematic methodology to establish a diagnosis will help provide clarity and consistency within a clinician's approach when determining prognosis and subsequently managing the EPL.
Clinical assessment of EPLs
The clinical presentation of an EPL can differ considerably, depending upon the aetiology behind the lesion. For example, in acute forms such as in recent trauma or an iatrogenic event, the patient may present with abscess and associated pain. In contrast, chronic lesions may present as an asymptomatic EPL, which developed over a longer period of time in a periodontitis patient.5
The clinician's assessment of an EPL should include the following aspects detailed below and in Figure 2.
The clinician is advised to take a detailed history to include:
Localization of pain;
Pain on biting and previous pain experiences from the tooth;
Bitter/unpleasant taste due to suppuration/bleeding;
Previous trauma to the tooth;
Previous endodontic treatment to the tooth;
Any periodontal treatment history.
Extra-oral examination should assess for signs of systemic infection, including:
Probing pocket depth around tooth in question including judgement on whether a narrow or wide pocket is present;
Buccal and oral soft tissue palpation and presence of swellings, sinus tracts and/or suppuration;
Mobility assessment;
Percussion test;
Presence of root grooves and furcations;
Signs of root fracture or perforations of the tooth structure;
Crown or gingival discoloration;
Assessment of occlusion and identification of occlusal trauma affecting the tooth (fremitus).
Assessing for root structure damage is particularly important, and is the first step in the diagnostic process as referred to above. The findings outlined by Herrera et al indicate that the usual causes of root structural damage were because of:5
Iatrogenic root, pulp or furcation perforation (either during endodontic instrumentation or post preparation);
Root fracture or cracking (either externally from trauma or due to post preparation, placement or removal);
External root resorption (usually secondary to trauma) or internal root resorption communicating with the periodontal ligament;
Pulp necrosis (due to trauma) draining through the periodontal tissues.
Special tests should follow once a provisional diagnosis is made. This should include:
A periapical radiograph;
Sensibility testing with thermal and electric tests to account for the sensitivity and specificity of both tests.
This is detailed later in this paper.
Aspects of the radiograph to assess
Aspects of the radiograph to assess include:
General bone levels;
Presence of localized deeper bone loss towards the apex (often referred to as ‘J-shaped’), or within the root furcation(s);
Deep caries or restoration;
Signs of fractures or perforations, either laterally or through the pulp chamber floor;
Root resorption processes.
Radiographically, depending on the avenue of fistulation, different degrees of bone loss may be evident. Lesions of primary endodontic and periodontal origin are clinically and radiographically very similar.
Sensibility testing
The presence of a periodontal pocket reaching, or close to, the apex combined with a negative or altered response to sensibility testing have been identified as primary signs of EPLs within the new classification.1,5
Sensibility tests are surrogate tests for tooth vitality and may be able to differentiate between pulpal and periodontal diseases. However, a false positive response might be elicited, with available tests particularly in cases of multi-rooted teeth that may have partial pulp necrosis. Similarly, a false negative response may be elicited in teeth with significant sclerosis of the pulpal environment or substantial in/direct restorations. In primary periodontal disease, the pulp is more likely to be responsive to sensibility testing than with primary endodontic disease.
It is important to carry out sensibility testing on teeth affected by primary periodontal disease, particularly when there are deep pockets and recession affecting them, due to the risk of exposing potential communications to the pulp.
Anecdotally, altered and unreliable responses to sensibility testing can occur around such teeth, presumably due to the neurovascular system becoming bathed in inflammatory substances. Where testing is inconclusive, it can be useful to provide a course of non-surgical periodontal treatment first and reassess the tooth in question at review to make a final decision on whether endodontic therapy is required.
Prognosis
The current diagnosis and classification system is also beneficial in assessing the prognosis of affected teeth, rather than identifying the primary source of infection, which is often difficult and does not affect the management or prognosis of the tooth.5 Clinicians need to be confident in assessing prognosis of teeth as this informs the decision whether to retain or extract the tooth.
Three main prognostic groups for a tooth with an EPL have been suggested.5 These are as follows:
Hopeless;
Poor;
Favourable.
There are a number of factors that can affect the prognosis associated with such teeth. These factors include the extent of the periodontal destruction around the tooth and the presence and severity of any periodontal disease affecting the rest of the dentition. EPLs arising from iatrogenic or traumatic events are usually considered of hopeless prognosis.5
There are a number of other factors to consider when assessing prognosis. These include the patient's healing response and the effectiveness of the patient's self-care and professional maintenance regimen. The success rate and longevity of a treatment and restorations provided also impacts on the overall prognosis of a tooth with an EPL.
For example, if iatrogenic damage such as a perforation is the primary cause of the EPL, it is important to consider that the presence of a perforation can reduce the success of non-surgical root canal therapy by 54% on average. However, this is size and position dependent.27
Management recommendations
The main factors to be considered when planning the management for EPLs are the pulp vitality of the tooth affected, as well as the type and the extent of the periodontal defect.
Occlusal trauma, such as fremitus on lateral or protrusive movements, should be identified and eliminated to reduce the risk of exacerbating the already inflamed periodontium. Sometimes it is not possible to eliminate such forces fully and splinting of the tooth to the adjacent teeth is indicated. Splinting of the teeth may also be indicated to carry out an accurate occlusal adjustment, particularly if the tooth/teeth are mobile. Splinting has a place within the treatment of such lesions, especially if it will improve patient comfort and function.28
In primary endodontic disease the pulp is often necrotic and infected; clinically these lesions may appear concurrently with drainage from the gingival sulcus area/sinus and possible swelling in the buccal attached gingiva. When there is drainage the patient may be asymptomatic.29
If a lesion is diagnosed and treated as primary endodontic disease due to lack of evidence of plaque-induced periodontitis, and there is soft tissue healing on clinical probing and bony healing radiographically, a valid retrospective diagnosis can be made. In the absence of adequate healing, further periodontal treatment is indicated.
Order of treatment
Primary endodontic disease with secondary periodontal involvement should be first treated endodontically, reviewed after three months and only then should periodontal therapy be considered. This sequence of treatment allows sufficient time for initial tissue healing and better assessment of the periodontal condition. It also reduces the potential risk of introducing bacteria and their by-products during the initial healing phase. The periodontal healing can be adversely affected by aggressive removal of the periodontal ligament and underlying cementum during interim periodontal therapy.
Primary periodontal disease with secondary endodontic or a true combined lesion requires both endodontic and periodontal treatment. The success rate of the endo-periodontal lesions without a concomitant regenerative procedure has been reported to range from 27%−37%.30 This is significantly lower than the reported success rate of 93% with conventional orthograde root canal therapy.31 A long junctional epithelium formation over the dehisced root surface has been suggested to be a contributing factor for the poor therapeutic prognosis.32 It has also been demonstrated that intra-pulpal infection tends to promote epithelial down growth along a denuded dentine surface.
It is accepted that non-surgical management of EPLs should be undertaken as a primary course of treatment. The response to the primary course of treatment should be reviewed and a decision made as to whether the tooth would benefit from a surgical approach following failure to achieve resolution.
The surgical approach will be dependent upon the remaining clinical signs and symptoms and the reassessed prognosis of the tooth, balanced against the tooth's strategic importance. It is necessary to consider whether tooth removal and subsequent replacement would be more appropriate.
The following case will demonstrate use of the new classification and processes highlighted above to come to a diagnosis and treatment strategy for successful management of an EPL.
Case example
This case involves a 35-year-old male who presented with a history of recurrent infections affecting his posterior teeth with current pain from the UL6. He was a non-smoker, medically fit and well and his oral hygiene was adequate. The clinical findings are summarized in Tables 3 and 4 and Figures 3 and 4.
Extra-oral Assessment
Fever or malaise
NAD
Facial swelling
NAD
Lymphadenopathy
NAD
General screening for periodontitis
Localized periodontitis –Stage IVGrade C
Intra-oral Assessment
Pocketing
10 mm wide pocketing around distal UL6 (2 sites) with bleeding on probing Periodontal pocketing associated with other posterior teeth
Soft tissues
Fluctuant swelling with associated sinus in the buccal aspect UL6
Mobility
No mobility
Percussion test
NAD
Presence of root grooves/furcations
F1 involvement UL6 buccally
Signs of root fracture/perforation/root resorption
NAD
Crown or gingival discoloration
NAD
Sensibility testing (ethyl chloride and EPT)
UL6 – positive
Occlusal assessment including identification of occlusal trauma
NAD
Radiographic assessment
General bone levels
Localized bone loss around posterior teeth
Localized bony defects
Specifically localized deep vertical bone defect extending to the apex of the disto-buccal root UL6
Deep caries/restorations
Small occlusal restoration
Signs of fractures or perforations, either laterally or through the pulp chamber floor
Following the new classification, this case would be classified as EPL without root damage in a periodontitis patient (Grade 3). The patient's first phase of treatment was a non-surgical phase that included:
Oral hygiene education.
In this case, given the lateral periodontal abscess associated with the UL6 and the periodontal pocketing around the patient's other posterior teeth and that the tooth was responding positively to sensibility testing at first, it was considered that the EPL was primarily periodontal in nature. The first line treatment was therefore non-surgical periodontal therapy (NSPT), including full mouth debridement under local anaesthetic, in order to drain the abscess via the periodontium and stabilize the other periodontally involved sites. The patient attended an oral hygiene education review after one month, then post-treatment records were taken after three months to assess for healing and stabilization. It was evident at this point that there was considerable recession affecting the disto-buccal root of the UL6 and that this tooth was now not responsive to sensibility testing. The rest of the dentition had stabilized.
Non-surgical root canal treatment was then initiated on UL6, including a bulk fill composite plug in the disto-buccal canal to aid future surgical intervention. The occlusion was designed with no guidance on the UL6.
Following the initial non-surgical phase, the buccal swelling associated with the UL6 resolved (Figures 5 and 6).
Figure 5. Clinical presentation following non-surgical phase of treatment.Figure 6. Post-operative radiograph following non-surgical root canal treatment UL6. Demonstrates composite plug in the disto-buccal canal.
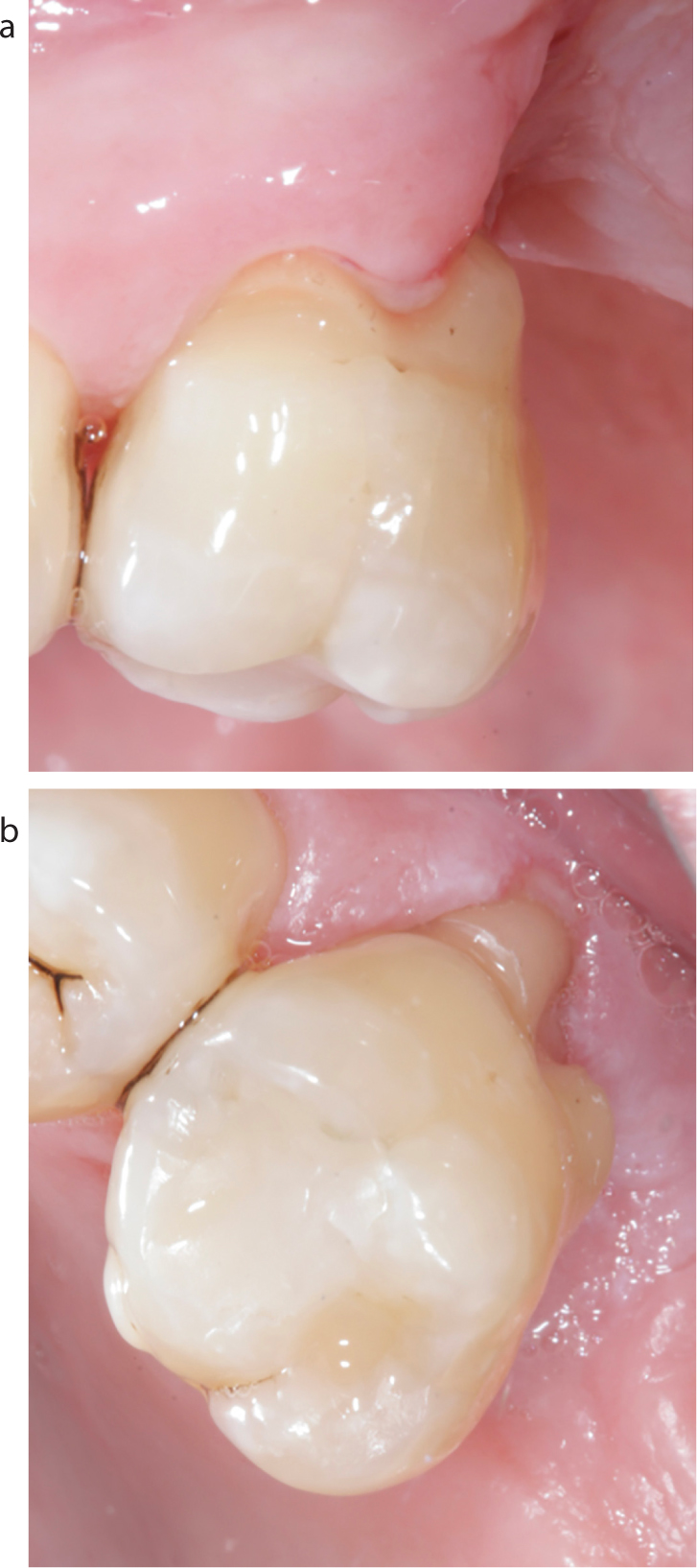
Following a successful non-surgical phase, the patient required a surgical phase to resect the disto-buccal root to improve cleansability. Short-term follow-up shows stability of the periodontal tissues (Figures 7 and 8). The patient will require ongoing periodontal maintenance with his general dental practitioner. This will include periodic review of the tooth, clinically and radiographically, with non-surgical periodontal therapy as required, as well as support with home-care advice on maintaining an excellent level of oral hygiene to prevent plaque accumulation.
Figure 7. (a, b) Post-operative presentation following surgical phase to resect the disto-buccal root.Figure 8. Radiograph after root resection of disto-buccal root UL6.
Conclusions
The treatment of EPLs is complex and has a poorer prognosis than treating a tooth with a singular bacterial infection of the periodontium or endodontic space alone. Assessment of the salvageability of the tooth, within the context of the whole oral health, needs to be assessed before embarking on complex care, with a guarded long-term prognosis. There are successful outcomes to be achieved in treating and retaining these teeth, with a combination of non-surgical and surgical treatments, as outlined. A comprehensive and realistic conversation needs to take place with the patient as part of the consent process, exploring salvage versus extraction and replacement options and documenting the inherent risks and benefits of each solution. It remains a valid option to treat EPLs after careful assessment and appropriate case selection.