Carter E, Yilmaz ZT, Devine M, Renton T. An update on the causes, assessment and management of third division sensory trigeminal neuropathies. Br Dent J. 2016; 220:627-635
Renton T. Oral surgery: part 4. Minimising and managing nerve injuries and other complications. Br Dent J. 2013; 215:393-399
Peñarrocha MA, Peñarrocha D, Bagán JV, Peñarrocha M. Post-traumatic trigeminal neuropathy. A study of 63 cases. Med Oral Patol Oral Cir Bucal. 2012; 17:e297-e300
Al-Ameri S, Nambiar P, Naidu M, Ngeow WC. Variation in lingual nerve course: a human cadaveric study. PLoS One. 2016; 11
Kocabiyik N, Varol A, Sencimen M, Ozan H. An unnamed branch of the lingual nerve: gingival branch. Br J Oral Maxillofac Surg. 2009; 47:214-217
Nixdorf DR, Velly AM, Alonso AA. Neurovascular pains: implications of migraine for the oral and maxillofacial surgeon. Oral Maxillofac Surg Clin North Am. 2008; 20:221-35
Hillerup S. Iatrogenic injury to oral branches of the trigeminal nerve: records of 449 cases. Clin Oral Investig. 2007; 11:133-142
Mason DA. Lingual nerve damage following lower third molar surgery. Int J Oral Maxillofac Surg. 1988; 17:290-294
Garisto GA, Gaffen AS, Lawrence HP, Tenenbaum HC, Haas DA. Occurrence of paresthesia after dental local anesthetic administration in the United States. J Am Dent Assoc. 2010; 141:836-844
Jacks SC, Zuniga JR, Turvey TA, Schalit C. A retrospective analysis of lingual nerve sensory change after mandibular bilateral sagittal split osteotomy. J Oral Maxillofac Surg. 1998; 56:700-704
Goldie SJ, Soutar DS, Shaw-Dunn J. The effect of surgical resection in the region of the retromolar trigone. J Plast Reconstr Aesthet Surg. 2006; 59:1263-1268
Zhao YF, Jia J, Jia Y. Complications associated with surgical management of ranulas. J Oral Maxillofac Surg. 2005; 63:51-54
Nahlieli O. Complications of sialendoscopy: personal experience, literature analysis, and suggestions. J Oral Maxillofac Surg. 2015; 73:75-80
Piagkou M, Demesticha T, Piagkos G, Georgios A, Panagiotis S. Lingual nerve entrapment in muscular and osseous structures. Int J Oral Sci. 2010; 2:181-189
Krmpotic-Nemanic J, Vinter I, Hat J, Jalsovec D. Mandibular neuralgia due to anatomical variations. Eur Arch Otorh. 1999; 256:205-208
Isberg AM, Isacsson G, Williams WN, Loughner BA. Lingual numbness and speech articulation deviation associated with temporomandibular joint disk displacement. Oral Surg Oral Med Oral Pathol. 1987; 64:9-14
Loughner BA, Larkin LH, Mahan PE. Nerve entrapment in the lateral pterygoid muscle. Oral Surg Oral Med Oral Pathol. 1990; 69:299-306
Schmidseder R, Scheunemann H. Nerve injury in fractures of the condylar neck. J Maxillofac Surg. 1977; 5:186-190
Griffiths H, Townend J. Anesthesia of the inferior alveolar and lingual nerves as a complication of a fractured condylar process. J Oral Maxillofac Surg. 1999; 57:77-79
Laws IM. Two unusual complications of fractured condyles. Br J Oral Surg. 1967; 5:51-59
Winter R, Munro M. Lingual and buccal nerve neuropathy in a patient in the prone position: a case report. Anesthesiology. 1989; 71:452-454
Windfuhr JP, Schlöndorff G, Sesterhenn AM, Kremer B. From the expert's office: localized neural lesions following tonsillectomy. Eur Arch Otorhinolaryngol. 2009; 266:1621-1640
McKenzie D. Injury to lingual nerves in Guillotine removal of the tonsil. Proc R Soc Med. 1924; 17:14-15
Al-Amery SM, Ngeow WC, Nambiar P, Naidu M. A pilot study on the effects of direct contact of two different surgical burs on cadaveric lingual nerve. Int J Oral Maxillofac Surg. 2018; 47:1153-1160
Hunt PR. Safety aspects of mandibular lingual surgery. J Periodontol. 1976; 47:224-229
Klasser GD, Utsman R, Epstein JB. Taste change associated with dental procedure: case report and review of the literature. J Can Dent Assoc. 2008; 74:455-461
de Koomen HA. A prosthetic view on vestibuloplasty with free mucosal graft. Int J Oral Surg. 1977; 6:38-41
Ellies LG. Altered sensation following mandibular implant surgery: a retrospective study. J Prosthet Dent. 1992; 68:664-671
Berberi A, Le Breton G, Mani J, Woimant H, Nasseh I. Lingual paresthesia following surgical placement of implants: report of a case. Int J Oral Maxillofac Implants. 1993; 8:580-582
Renton T, Thexton A, Crean SJ, Hankins M. Simplifying the assessment of the recovery from surgical injury to the lingual nerve. Br Dent J. 2006; 200:569-573
Momota Y, Kani K, Takano H, Azuma M. Cerebellopontine angle mass mimicking lingual nerve injury after dental implant placement: a case report. Aust Dent J. 2015; 60:412-415
Yamauchi Y, Ikeda M, Yamada Y, Ishiyama E, Ishiyama K, Tomita H. Dysgeusia due to an orthodontic wire: a case report. Acta Orolaryngol Suppl. 2002; 122:173-176
Mozsary PG, Middleton RA. Microsurgical reconstruction of the lingual nerve. J Oral Maxillofac Surg. 1984; 42:415-420
Peňarrocha-Diago M, Mora-Escribano E, Bagán JV, Peňarrocha-Diago M. Neoplastic trigeminal neuropathy: presentation of 7 cases. Med Oral Patol Oral Cir Bucal. 2006; 11:e106-e111
Strong MJ, Noseworthy JH. Hemiageusia, hemianaesthesia and hemiatrophy of the tongue. Can J Neurol Sci. 1986; 13:109-110
Carter RL, Tanner NSB, Clifford P, Shaw HJ. Perineural spread in squamous cell carcinomas of the head and neck: a clinicopathological study. Clin Otolaryngol Allied Sci. 1979; 4:271-281
Singh FM, Mak SY, Bonington SC. Patterns of spread of head and neck adenoid cystic carcinoma. Clin Radiol. 2015; 70:644-653
Brooks JK, Ricalde P, Nikitakis NG, Levy BA. Angioleiomyoma of the tongue. Gen Dent. 2004; 52:52-54
Lee JJ, Jung KH, Park JM, Kwon O, Kim BK. Lingual nerve palsy associated with submandibular gland carcinoma. Acta Neurol Belg. 2015; 115:439-440
Tessema B, Sulica L, Yu GP, Sessions RB. Tongue paresthesia and dysgeusia following operative microlaryngoscopy. Ann Otol Rhinol Laryngol. 2006; 115:18-22
Lang MS, Waite PD. Bilateral lingual nerve injury after laryngoscopy for intubation. J Oral Maxillofac Surg. 2001; 59:1497-1499
James FM Hypesthesia of the tongue. Anesthesiology. 1975; 42
Winter R, Munro M. Lingual and buccal nerve neuropathy in a patient in the prone position: a case report. Anesthesiology. 1989; 71:452-454
de Toledo GL, Bueno SC, Mesquita RA, Amaral MB. Complications from submental endotracheal intubation: a prospective study and literature review. Dent Traumatol. 2013; 29:197-202
Majumder S, Hopkins PM. Bilateral lingual nerve injury following the use of the laryngeal mask airway. Anaesthesia. 1998; 53:184-186
Ahmad NS, Yentis SM. Laryngeal mask airway and lingual nerve injury. Anaesthesia. 1996; 51:707-708
Renes SH, Zwart R, Scheffer GJ, Renes S. Lingual nerve injury following the use of an i-gel laryngeal mask. Anaesthesia. 2011; 66:226-227
Lewis DW, Frank LM, Toor S. Familial neck-tongue syndrome. Headache. 2003; 43:132-134
Bogduk N. An anatomical basis for the neck-tongue syndrome. J Neurol Neurosurg Psychiatry. 1981; 44:202-208
Chuah C, Mehra P. Bilateral lingual anesthesia following surgically assisted rapid palatal expansion: report of a case. J Oral Maxillofac Surg. 2005; 63:416-418
Dong Z, Bao H, Zhang L, Hua Z. Eagle's syndrome associated with lingual nerve paresthesia: a case report. J Oral Maxillofac Surg. 2014; 72:886.e1-4
Goldberg MH, Galbraith DA. Late onset of mandibular and lingual dysesthesia secondary to post-extraction infection. J Oral Surg. 1984; 58:269-271
Sadler RM, Curran T, Pryse-Phillips WE. Numbness of half of the tongue. Can J Neurol Sci. 1986; 13:107-108
Kipp DP, Goldstein BH, Weiss WW Dysesthesia after mandibular third molar surgery: a retrospective study and analysis of 1,377 surgical procedures. J Am Dent Assoc. 1980; 100:185-192
Peñarrocha M, Alfaro A, Bagán JV Idiopathic trigeminal sensory neuropathy. Int J Oral Maxillofac Surg. 1992; 50:472-476
Robinson CM, Addy L, Wylie M, Luker J, Eveson JW, Prime SS. A study of the clinical characteristics of benign trigeminal sensory neuropathy. J Oral Maxillofac Surg. 2003; 61:325-332
Harris W. Paroxysmal neuralgic tic as a sequel of trigeminal neuritis. Br Med J. 1935; 1112-1114
Fisher CM. Trigeminal sensory neuropathy. Arch Neurol. 1983; 40:591-592
Cruccu G, Pennisi EM, Antonini G, Biasiotta A, di Stefano G, La Cesa S, Leone C, Raffa S, Sommer C, Truini A. Trigeminal isolated sensory neuropathy (TISN) and FOSMN syndrome: despite a dissimilar disease course do they share common pathophysiological mechanisms?. BMC Neurol. 2014; 14 https://doi.org/10.1186/s12883-014-0248-2
Shotts RH, Porter SR, Kumar N, Scully C. Longstanding trigeminal neuropathy of nontraumatic cause. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:572-576
Silbert BI, Silbert PL. Under-recognized: inflammatory trigeminal neuropathy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013; 116:659-660
Laskin DM, Abubaker AO. Decision Making in Oral and Maxillofacial Surgery.Chicago: Quintessence Publishing Co Inc; 2007
Lingual nerve neuropathy: more than just third molar surgery and inferior alveolar nerve blocks Wei Cheong Ngeow Wen Lin Chai Dental Update 2024 46:8, 707-709.
Authors
Wei CheongNgeow
Lecturer, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Universiti Kebangsaan Malaysia (UKM), Kuala Lumpur, Malaysia
Neuropathy of the lingual nerve, when it occurs, often results from third molar surgery, or the provision of inferior alveolar nerve blocks. Investigators have reported that the anatomical location and the unpredictable course of the lingual nerve play important roles in it being affected by these procedures. However, there are many other causes of neuropathy with which most medical and dental practitioners are unfamiliar. This article briefly reviews the course of the lingual nerve, and summarizes the causes and reports of all uncommon aetiologies of neuropathy that can occur along the path of a lingual nerve. The clinical implication and management of lingual nerve neuropathy is discussed.
CPD/Clinical Relevance: The reader should appreciate the importance of accurately diagnosing lingual nerve neuropathy as it can manifest from many other dental procedures and non-dental causes, apart from routine mandibular third molar surgery and local anaesthetic injections.
Article
Peripheral nerve neuropathy is a condition where damage to a particular branch of the peripheral nerve results in weakness, numbness and/or pain in the area of innervation. A recent article has extensively reviewed neuropathy affecting the mandibular branch of the trigeminal nerve, mainly in association with ‘numb chin syndrome’.1 Based on this review, a summary of the causes of neuropathy is provided in Table 1. Neuropathy involving the lingual nerve, either alone or with other branches of the trigeminal nerve, is not commonly reported, but merits special attention. Most are iatrogenic in origin, and involve third molar surgery, dental local anaesthetic injections, intubation, ablative surgery and submandibular gland surgery. Of these, third molar surgery has been reported as the most common cause of lingual nerve injuries.2 Often, numbness is the chief complaint if the lingual nerve is injured. However, Peñarrocha et al reported that nerve injuries can be painful and this symptom affected up to 57% of their patients.3 This painful neuropathy was more often observed in older patients with neurosensory deficit.3 In contrast, younger patients reportedly had less pain and recovered faster from this symptom.3 Investigators have reported that the anatomical location and the unpredictable course of the lingual nerve is an important factor contributing to iatrogenic injury, besides the skill of the surgeons.
Iatrogenic (Surgical)
Maxillofacial surgery
Sagittal split osteotomies
Reduction and fixation of mandibular fractures
Minor oral surgery
Third molar removal
Implant placement
Anaesthetic injections
Inferior dental block
Mental block
Endodontics
Instrumentation beyond the apex
Extrusion of irrigation fluid and filling materials
Radiotherapy
Exposure to chemical agents
Trichloroethylene, stilbamidine, and allopurinol
Whiteheads varnish and oxidized cellulose polymer
Carnoy's solution
Prosthetic dentistry
Denture compression
Iatrogenic (Medical)
Medication-related osteonecrosis of the jaw (MRONJ)
Infections
Local periapical infection of teeth
Viral infections, eg herpes zoster
Syphilis and lyme disease
Osteomyelitis (acute, chronic or diffuse sclerosing)
Direct extension of a squamous cell carcinoma of the lip
Secondary neoplasms affecting the nerve, eg adenoid cystic carcinoma, colon and rectum cancer, lung cancer (small cell and non-small cell carcinoma), lymphoma (Hodgkin and non-Hodgkin), lymphosarcoma and Waldenstrom myeloma, prostate cancer, thyroid carcinoma, uterine carcinoma
Medical/Systemic pathology
Immunological disorders, eg rheumatoid arthritis, connective tissue diseases, and sarcoidosis
Cerebro-vascular accident and degenerative neurological disease, eg multiple sclerosis
Haematological disorders, eg sickle cell disease
Metabolic and endocrine disorders, eg diabetes mellitus
Idiopathic
It has been proposed that neuropathy with no underlying cause could be secondary to herpes simplex viral infections
However, there are many other causes of lingual nerve neuropathy with which most medical and dental practitioners are unfamiliar. This article aims to review and summarize the scientific literature that describes different causes of lingual nerve neuropathy, beginning from 1924 when a case of lingual nerve injury was reported to result from a non-dental procedure. The authors wish to begin by briefly reviewing the extracranial course of the lingual nerve, along which the different possible causes of injury and/or neuropathy are highlighted. Based on these causes, the mechanism of injury, the incidence (if reported), the presentation or degree of altered sensation, the intervention or management taken thereafter, and the outcome of this management are described.
The extracranial course of the lingual nerve
The lingual nerve is one of the two terminal branches of the posterior division of the mandibular nerve. It is a sensory nerve and relays general somatic afferent sensation from the mucosa of the anterior two thirds of the tongue, the sublingual mucosa, the mandibular lingual gingiva and the floor of the mouth.4 The chorda tympani nerve, a branch of the facial nerve, joins the lingual nerve medial to the lateral pterygoid muscle, after descending near the spine of the sphenoid bone. It carries special visceral afferent (taste) fibres from the anterior two thirds of the tongue and general visceral efferent (parasympathetic secretomotor) innervations to the submandibular and sublingual glands.4
Often, it has been suggested that the lingual nerve may be subjected to iatrogenic injury during dental procedures because of its course in the oral cavity. The lingual nerve runs inferiorly in an intimate relationship with the lateral pterygoid muscle in the infratemporal fossa. It usually runs deep to this muscle immediately after branching off beneath the foramen ovale.4 It may communicate with the inferior alveolar, auriculotemporal or the mylohyoid nerves at this location.4 It is gradually carried closer to the medial surface of the mandibular ramus inferiorly until it is in close relationship with the bone, just a few millimetres below and behind the junction of the vertical and horizontal rami of the mandible.4 It enters the submandibular region after passing forward and medially, inferior to the lower border of the superior constrictor muscle of the pharynx. Here, it comes into close relationship with the lower third molar.4 In 4.6% and 21.0% of the cases reported, the lingual nerve may be situated at or above the crest of bone, with some even taking a course through the retromolar pad region.4
It may give off a branch to the lingual gingivae, extending horizontally from the medial mandibular cortex at the level of the retromolar pad to mesial of the lower first molar-second premolar to supply the lingual periosteum, gingiva and mucosa that are overlying the medial alveolar process. This branch is termed the ‘collateral nerve twigs’ or ‘the gingival branch of the lingual nerve’.4,5
The lingual nerve then leaves the lingual plate from the third molar region and courses towards the tongue. At the anterior border of the hyoglossus muscle it turns around the outer side of the submandibular (Wharton's) duct to ascend into the body of the tongue, medial to this duct.4 It usually passes lateral to the submandibular duct, winds below it and then passes upwards and forwards on the medial side on its way to the surface of hyoglossus.4 At the floor of the mouth, the lingual nerve may give out branches that communicate with the mylohyoid nerve, termed the ‘mylohyoid or sublingual curl’.4 In addition, the lingual nerve may also communicate with the hypoglossal nerve on the anterior border of the hyoglossus muscle.4 More anteriorly, a gingival branch runs between the sublingual gland and the mandible to supply the lingual gingiva and adjoining sulcus.4
A review of the uncommon causes of lingual nerve neuropathy
Aside from central causes, such as migraine and degenerative neurological conditions like multiple sclerosis,1,6 extra-cranial injury or pathology affecting the lingual nerve can occur anywhere along the course and distribution described above. As stated earlier, the most commonly reported neuropathy of the lingual nerve is associated with surgical removal of impacted lower third molars,7,8 followed by the provision of inferior alveolar nerve blocks.9 Other causes include surgical procedures performed within its vicinity, such as orthognathic surgery,10 resection of the tumour at the molar trigone area11 and submandibular gland-related procedures, such as the excision of ranula and sialoendoscopy.12,13 Of course, there are many other extra-cranial causes that are not often highlighted to medical and dental practitioners. They are of interest for diagnosing a lingual nerve-related condition or symptom(s). Based on the course of the lingual nerve, these causes are as follows:
The entrapment of the lingual nerve in the infratemporal fossa;
Fracture of the condyle and retraction of the mandible;
Tonsillectomy;
Dento-alveolar surgery and treatment at the lower molar region;
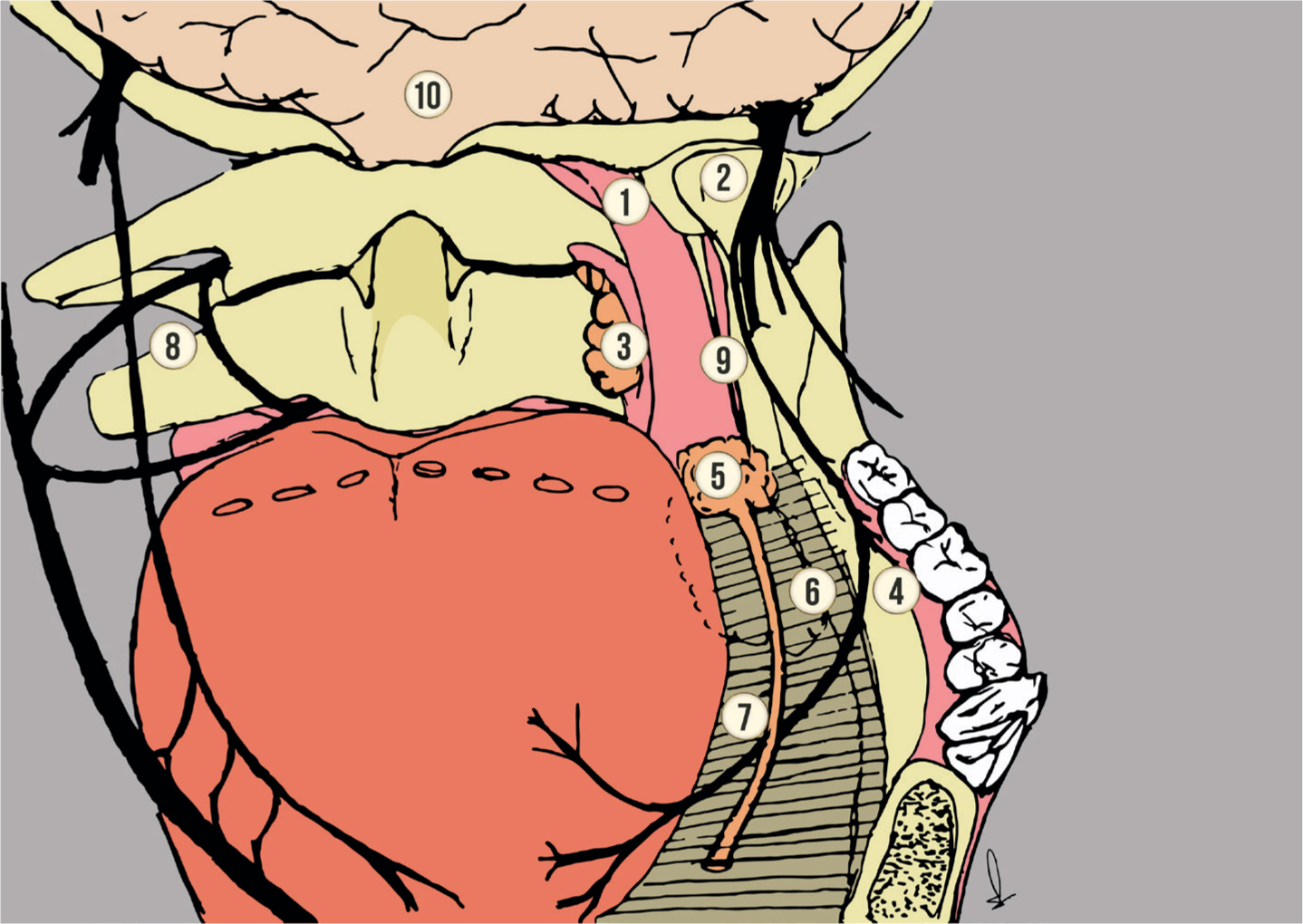
Figure 1 provides a summary of the anatomical locations where these less common causes can inflict lingual nerve neuropathy.
Figure 1. A summary of the anatomical locations where some less common causes of lingual nerve neuropathy have been reported: (1) infratemporal fossa; (2) condyle; (3) tonsil; (4) retromolar and lingual mucosa; (5) submandibular gland and duct; (6 and 7) floor of mouth; (8) cervical spine and the ansa cervicalis-ansa hypoglossi loop; (9) styloid process; and (10) the central nervous system.
1. The entrapment of the lingual nerve in the infratemporal fossa
An entrapment or compression neuropathy is nerve injury caused by pressure or mechanical irritation from anatomic structures located next to the nerve. This happens when the nerve passes through a fibro-osseous canal, or becomes impinged by an anatomic structure, such as bone, muscle or a fibrous band.14 The entrapment of the lingual nerve by the muscular and osseous structures in the infratemporal fossa is unusual but has been suggested to happen.14 The exact incidence of entrapment neuropathy is unknown. So far, all evidence of lingual nerve impingement was derived from cadaveric studies, and is hypothesized to cause lingual nerve neuropathy when no other aetiology or lesion is found.14 The anatomical sites of entrapment in the infratemporal fossa are:
The partially or completely ossified pterygo-spinous or pterygo-alar ligaments at the cranial base;
The large lamina of the lateral plate of the pterygoid process; and
The medial fibres of the anterior region of the lateral pterygoid muscle.14 In one rare report, the presence of a pterygo-spinous foramen replacing the foramen ovale was suggested to provoke trigeminal neuralgia.15 Because of compression, patients can present with neuropathy along the distribution of the lingual nerve and/or the inferior alveolar nerve, or even the auriculotemporal nerve, all of which course together with the lingual nerve in the infratemporal fossa. This neuropathy may range from anaesthesia, paraesthesia, hypoaesthesia to dysaesthesia and hyperaesthesia. In addition, it has been suggested that lingual nerve compression can also cause speech impairment.16,17
Some clinical symptoms, such as pain and ‘tightness’ felt at the temporomandibular joint area, may lead to inaccurate diagnosis of atypical facial pain or temporomandibular joint disorder, if not carefully investigated. It is important to check for the presence of pathology in the infratemporal area when such a patient complains of having altered sensation along the distribution of the lingual nerve.1 Isberg et al reported finding seven cases (3.4%) of lingual numbness and speech articulation deviation in a study of 208 patients suffering from anthrographically verified temporomandibular joint disk displacement.16 These patients, however, did not suffer from dysgeusia. Isberg et al were able to provide relief by giving local anaesthetic blocks to the auriculotemporal nerve.16 They hypothesized that the lingual nerve in the affected patients coursed through the lateral pterygoid muscle rather than being medial to it. They were able to show such features in 6.1% of cadaver dissections but did not prove the same in the symptomatic patients. Nevertheless, they suggested that ‘arthrokinetic myospasm resulting in compression’ of the lingual nerve caused this problem. The observation of lingual nerve entrapment was confirmed by Loughner et al 3 years later in a cadaveric study.17 They found three (5.8%) lingual nerves entrapped within the lateral pterygoid muscles in 52 hemi-heads and reported that the inferior alveolar and the auriculotemporal nerves were also entrapped; but the corda-tympani nerve was spared. The discovery of a lingual nerve passing through the lateral pterygoid is new as no other anatomic textbooks or journals have described such variation. However, it is yet to be proven that this variation causes lingual nerve neuropathy.
2. Fracture of the condyle and retraction of the mandible
The condyle is located close to the foramen ovale, the opening where the mandibular division of the trigeminal nerve exits the skull. Further inferiorly, the lingual nerve lies adjacent to the muscular attachment of the condyle, ie the lateral pteryoid muscles, before entering the pterygomandibular space. Because of the shape of the mandible, the temporomandibular joint and the condyle are susceptible to injury following trauma to the lower jaw. To date, at least three cases of fractured condyle with reported lingual nerve neuropathy were found.18,19,20 Schmidseder and Scheunemann reported a prevalence of 0.4% lingual nerve neuropathy in their series of 237 condylar neck fractures.18 In all cases, the lingual nerve was not the sole nerve affected. Griffiths and Townend reported that the inferior alveolar nerve was affected as well, but with no dysgeusia.19 Their patient sustained a medially displaced fracture of the condyle that impinged onto the foramen ovale. The symptoms of trismus and lingual and inferior alveolar nerves neuropathy resolved following open reduction and internal fixation that returned the fractured condyle to its original position. In a different case, Laws reported the involvement of two additional nerves, namely the long buccal and the auriculotemporal nerves.20 Numbness at the site innervated by these nerves resolved gradually without surgical intervention to the fractured condyle. Laws observed that anaesthesia did not appear for some hours after the accident, suggesting that nerve compression was caused by oedema and haemorrhage.20 Besides branches of trigeminal nerves, the facial nerve and the corda tympani nerve were reported to be affected too, but neuropathy resolved with time.18 As fracture to the condyle can occasionally be missed when the patient's occlusion remains intact, appropriate radiographs should be taken when a patient complains of trigeminal nerve neuropathy following trauma. The resolution of the lingual nerve neuropathy in such a situation depends on the extent of nerve compression. So far only one case has been reported to benefit from open reduction and internal fixation of the fractured condyle.19
Besides a fractured condyle, prolonged retraction of the mandible has been reported to result in lingual nerve neuropathy. Winter and Munro reported a case of lingual and buccal nerves neuropathy happening after general anaesthesia.21 They hypothesized that these nerves received compressive tension arising from the retraction of the mandible due to the prone position adopted.21 They speculated that lingual nerve neuropathy could also possibly have occurred when the lingual nerve was compressed between the lateral and medial pterygoid muscles. This neuropathy gradually resolved by the fourth week post-operative without any medical or surgical treatment. Fortunately, this is a rare event and no additional case has been reported since then.
3. Tonsillectomy
Tonsillectomy is a surgical procedure performed at the tonsillar region, a site which is a distance away from the course of the lingual nerve. Nevertheless there are reports of lingual nerve neuropathy following tonsillectomy.22 From a retrospective study of expert reports written for malpractice claims together with a literature review, Windfuhr et al suggested that neuropathy following tonsillectomy was underreported.22 They found 4 cases of solitary lingual nerve injury, and 8 cases of combined injury (7 with the glossopharyngeal nerve; 1 with the hypoglossal nerve) following tonsillectomy in a series of 648 patients. This gives a prevalence of 1.85%. All affected patients were female, and all injuries were treated conservatively. Two of the patients were children, with one sustaining permanent injury to the lingual nerve as a result of direct surgical trauma of a guillotine procedure.23 Forty-two percent of these cases involved bilateral tongue symptoms, usually affecting the glossopharyngeal nerve as well. Overall, more than half (58%) of the nerve injuries were permanent in nature. Cases with transient neurosensory disturbance resolved between 2 weeks and 4 months and, in cases of solitary lingual nerve injury, complete recovery was observed in only 1 case.
Windfuhr et al suspected that pressure and stretching was the cause of lingual nerve injury, but did not describe in detail the mechanism of injury.22 Nevertheless, Windfuhr et al emphasized that careful intubation, as well as careful insertion of the mouth gag and avoidance of inadequate pressure/forced head extension, will reduce the risk of lingual (and also hypoglossal) nerve injury.22 Based on this review, perhaps patients who are about to undergo tonsillectomy should be forewarned of the potential risk of post-operative neurosensory disturbance within the oral and pharyngeal region.
4. Dento-alveolar surgery and treatment at the lower molar region
It has been reported that 75% of the annual incidence of lingual nerve injury is attributable to the surgical removal of the lower third molars.24 Many reports have discussed the causes for this, with many attributing it to the elevation and retraction of a lingual flap.2,8 Fortunately, 88–90% of the neuropathy reported were transient in nature.8 Because of this risk, the buccal access technique is advocated as it shall avoid the lingual nerve altogether. However, it remains possible for patients to experience more permanent injury if a drill is applied distal to the third molar, especially in combination with the lingual guttering technique.24 Such an approach may inflict direct injury and a recent study has shown that the severity of injury depended on the speed and type of drill used.24 Because it is a direct injury, surgical repair may be necessary, unlike in cases of lingual flap retraction.
Apart from third molar surgery, periodontal, pre-prosthetic and implant surgery, when performed in the vicinity of the lingual nerve, may result in neurosensory disturbance.25,26,27,28,29 For more than 40 years, periodontists have been cautioned against raising a lingual flap for the purpose of rendering periodontal therapy to the lingual site of the lower molars and the interdental bone out of fear of getting too close to this nerve.25 Yet, there is a report of a 66-year-old man who suffered from taste change several weeks after a combined oral surgical and periodontal procedure. In particular, he received surgical incisions involving the sulcular, buccal and palatal tissues in the mandibular posterior regions to allow access for thorough debridement and recontouring of the residual osseous defects in these areas. Treatment with zinc supplements 450 mg/day partially improved his symptom but normal taste sensation did not return.26 Most researchers reported that the lower third molar site is the location where the lingual nerve is most superficially located, with between 20–62% being in contact with the lingual cortical plate.4 In between 4.6% and 21.0% of cases, the lingual nerve may be situated at or above the crest of bone.4 In 0.15% to 1.5% of cases, this nerve is situated at the retromolar pad region.4 While dental surgeons are often cautioned on the vulnerability of this site during third molar surgeries, there are no statistics that describe the prevalence of neuropathy resulting from other surgical procedures, such as periodontal surgery, pre-prosthetic and implant surgery. Kocabiyik et al suggested that neurosensory disturbance on the lingual gingival tissue alone is related to manipulation of the mucoperiostal flap containing the ‘collateral nerve twigs’ or ‘the gingival branch of the lingual nerve’, which in most cases can be confused with paraesthesia of the main lingual nerve trunk.5 Regardless of the types of procedure, any suspected or known surgical injury to the lingual nerve should be explored and repaired immediately. Otherwise, observation should include measuring the initial size of neuropathic area and assessing for the lack of mechanosensory function. Both parameters can be prognostic of poor outcome and the lack of improvement after 3 months may be an indicator for surgical exploration.30
A study by de Koomen 40 years ago showed that up to 39% of patients experienced altered sensation after vestibuloplasty procedures, especially in cases that involved deepening the floor of the mouth.27 The latter procedure routinely involves elevating a full-thickness flap over the lingual gingiva and mucosa. Two-thirds of his patients experienced altered sensation at the area of lingual nerve innervations.27 Besides stating that these cases deserved serious attention, de Koomen did not report if these patients received any medical or surgical therapy for the symptom.27 Fortunately, these procedures are no longer a routine procedure in pre-prosthetic dentistry.
Although uncommon, there have been reports indicative of lingual nerve injury following dental implant placement.28,29 In one report, two molar implants were found to have protruded to the lingual site when a computed tomography (CT) scan was performed following a complaint of post-operative numbness. The scan suggested that the apices of the implant were pressing onto the lingual nerve traversing beneath the mucosa. Fortunately, this symptom resolved completely 2 months after the removal of these implants.29 Collectively, implant-related injury made up between 14% and 16% of all trigeminal nerve injuries involved in dental implant treatment.27 Ellies, in a retrospective study, reported that 11 (5.2%) of 212 patients surveyed experienced altered sensation in the tongue, with 10 being transient in nature following implant placement anterior to the mental foramen.28 Only one patient had persistent change following surgical implant operation posterior to the mental foramen. His survey, however, did not determine the cause of numbness or whether these patients received any kind of treatment for the neuropathy. Nevertheless, he cautioned that extra care should be exercised when working at the posterior mandible. A subsequent report at a different centre suggested that lingual nerve neuropathy may originate from the inferior alveolar nerve blocks instead of surgical trauma.28 Recently, a case of lingual nerve neuropathy that results from the presence of a cerebellopontine angle mass, but mimicking implant-related injury, has been reported.31 This misdiagnosis arises as neuropathy of the lingual nerve happened immediately after implant placement. The patient developed ipsilateral numb lip 7 months later, which led to the discovery of a cerebellopontine angle mass using magnetic resonance imaging.
There were two other types of dental treatment that have been cited to cause lingual nerve neuropathy, namely orthodontics and prosthetic dentistry. The prevalence of such occurrences has not been reported, and so far they have been presented as case reports. A rare case of numbness and dysgeusia affecting a 14-year-old Japanese female due to orthodontic wire mishap has been reported. The cause was a wire that became dislodged while she was having a meal and penetrated into the retromolar trigone. The symptoms lasted for about 10 days but resolved immediately after the wire was repositioned. The authors postulated two possible mechanisms for this problem, namely, direct mechanical compression of the lingual nerve by the penetrating wire, and impairment of local circulation caused by oedema in the surrounding tissues following trauma.32 Instead, Mozsary and Middleton reported of surgically relieving an elderly patient of a gradual loss of sensation that occurred over a period of 3 months.33 She had been wearing the same complete lower denture for 18 years. Apparently over time, because of prolonged friction, her denture base caused excessive tissue hyperplasia and scarring that entrapped the lingual nerve. The symptom disappeared after the lingual nerve was surgically relieved from the entrapment.
5. Tumour invasion and perineural spread
Neuropathy of neoplastic origin accounts for a small percentage of trigeminal neuropathies, even less for those affecting the lingual nerve alone. Nevertheless, it is an important cause that needs meticulous investigation as numbness at the tributaries of the trigeminal nerve may be the first manifestation of a primary tumour, perineural spread or metastatic relapse.1 Lingual nerve neuropathy may result from nerve compression or from perineural invasion where tumour cell invades in, around, and through the nerve. The prevalence of such occurrence has not been reported, and most cases presented in the literature were case reports. Nevertheless, it is important to rule out the presence of neoplastic lesions in patients complaining of numbness of undetermined origin.34 Peňarrocha-Diago et al reported three patients with trigeminal neuropathic pain who were treated initially as a having facial pain disorder because of misdiagnosis.34 In contrast, Strong and Noseworthy reported a case with neurological presentation of hemiageusia, hemianaesthesia and hemiatrophy of the tongue with dysphagia and dysgeusia that was almost missed because the squamous cell carcinoma was hidden in the submandibular fossa.35 Some pathology of the head and neck, such as squamous cell carcinoma (SCC), adenocarcinoma and adenoid cystic carcinoma (ACC) have been known to cause altered sensation of the tongue.35,36 Perineural invasion accounts for 24% of SCC and 50% of ACC, with the tongue, floor of the mouth and retromolar trigone being the sites of tumour invasion in cases involving the lingual nerve.35,36,37 In the case of SCC, neurosensory disturbance occurs early in the disease. Carter et al reported that 79% of patients with histologically confirmed perineural spread reported either hypoaesthesia, dysaesthesia and referred pain.36 Perineural spread was more likely to occur with large moderate or poorly differentiated carcinomas that show local invasion and lymph node metastases.36 Less common cause of neuropathy includes angioleiomyoma of the tongue, which has been reported by Brooks et al.38 Their patient sought treatment for a painless, bi-lobed rubbery mass of 10 years' duration on the dorsal aspect. This tumour caused occasional episodes of numbness. Unfortunately, no definitive outcome was reported as the patient was lost to follow-up, with a complete surgical excision of the tumour not performed.
A case of compressive pressure causing tongue numbness originating from a submandibular gland tumour has recently been reported by Lee et al.39 This tumour (carcinoma ex pleomorphic adenoma) was found using CT scan when MRI failed to find the source of symptom that lasted over 2 months. This case exemplifies that meticulous examinations and investigations are mandatory when lingual nerve neuropathy is of a suspicious nature. Appropriate referral to the oral medicine specialist, neurologist and/or oral and maxillofacial surgeon should be made instantly when no local cause can be identified. It is not advisable to label any unknown case of neurosensory disturbance as idiopathic trigeminal sensory neuropathy before exhausting all means of investigations (see last section on Idiopathic trigeminal sensory neuropathy).
Endolaryngeal microsurgery or suspended laryngoscopy is a technique used in diagnostic and operative laryngology, where the surgeons insert rigid instruments and examine a benign vocal cord lesion by using a microscope. To do so, they have to secure a straight path using a laryngoscope with its blade secured on a suspender and placed against the tongue base. This technique allows the surgeons to use both hands freely to perform microsurgical procedures while being supported on a stable operating platform.40 Several cases of lingual nerve neuropathy have been reported to result from endolaryngeal microsurgery (suspended laryngoscopy).40 A few of them involved the corda tympani nerve as well, causing the patient to suffer from dysgeusia and numbness of the tongue. The prevalence for this complication has been reported to range from 0.3% to 18%, but all neurosensory disturbance was transient in nature, with no intervention needed.40 In such cases, the part of the nerve that was subjected to compression was located either adjacent to the third molar or at the site where it travelled over the hyoglossus muscles and on the surface of genioglossus muscles deep to mylohyoid muscles.40 The prevalence of neurosensory disturbance seems to be associated with the duration of the surgery and the gender of the patients. Female patients were 5.5 times more likely to develop neurosensory disturbance than male patients,40 due to the fact that the design of the laryngoscope does not make allowance for the smaller female oral cavity and pharynx. Although this is an otorhinolaryngology-related complication, the dental surgeons may be consulted to rule out any other potential intra-oral causes. Hence, the ability to understand and relate the risk of this procedure to lingual nerve neuropathy is very important.
7. Intubation
General anaesthetic intubation has been reported to cause lingual nerve neuropathy in anaesthesiology literatures for over 45 years. Procedures implicated include routine/difficult laryngoscopy,41 face mask ventilation,42 orotracheal intubation,43 submental endotracheal intubation44 and the use of laryngeal (inflatable and noninflatable cuff) masks.45,46,47 All lingual nerve neuropathy has been associated with temporary compression of the lingual nerve along its course from the anterior pharynx to the lateral border of the tongue. Because this is a neuropraxia, the symptom was transient in nature, lasting between several days to several weeks. Excessive cuff pressure, anterior displacement of the mandible, prolonged mandibular retraction and cricoid pressure have been cited as some possible mechanism of compression during intubation.43 As for the use of inflatable cuffed laryngeal mask, the location of the proximal base of the mask just under the tongue might allow the cuff to compress the lingual nerve as it lies on the inner aspect of the mandible.45 Ahmad and Yentis suggested that compression can occur on the nerve distal to its gingival branch.46 A non-inflatable-cuffed laryngeal mask such as the i-gel laryngeal mask was used to fit the perilaryngeal and hypopharyngeal structures anatomically, however, failed to prevent lingual nerve compression from happening.47 Patients usually reported this symptom to the anaesthesiologists but, if they were to undergo mandibular third molar removal or any other surgery within the vicinity of the course of the lingual nerve under general anaesthesia, it would be difficult to determine the exact origin of lingual nerve neuropathy. In such cases, the altered sensation may be of general anaesthetic origin or surgically related. As oral and maxillofacial surgeons and occasionally hospital-based dental practitioners may subject their patients to undergo dental procedures under general anaesthesia, they may consider forewarning their patients that there may be a risk of lingual nerve compression that results from intubation.
8. The neck-tongue syndrome
The neck-tongue syndrome is an unusual phenomenon where patients suffer from unilateral stabbing pain at the upper neck or occipital region with simultaneous ipsilateral numbness of the tongue triggered by a sharp turning of the neck.48 The give-away sign is that it is only exaggerated by sudden rotation of the head and neck. The prevalence of this syndrome is unknown. Most cases cited in the literature were case reports and it has been reported to happen in normal patients as well as those with osteoarthritis, degenerative spondylosis and ankylosing spondylitis. It can be precipitated by prolonged poor sitting posture. One group of investigators suggested that this syndrome has an autosomal dominant inheritance pattern.49 The neck-tongue syndrome is primarily attributed to problems with the C2 nerve root, with the most likely cause being related to an abnormal subluxation of one lateral atlanto-axial joint with compression of the C2 ventral ramus during head turning.50 Anatomy dissection has shown that the C2 ventral and dorsal roots unite to form a short spinal nerve which divided into a dorsal and a ventral ramus. This series of nerves lies dorsal to the lateral atlanto-axial joint. The C2 ventral ramus courses transversely across the lateral atlanto-axial joint and, along its course, gives off from its ventral surface articular branches to the joint. The elements of the C2 nerves which are susceptible to bony impingement are the C2 dorsal root ganglion and the C2 ventral ramus. The ganglion may be compressed between the posterior arch of the atlas and the superior articular process of the axis, during combined extension and rotation. C2 ventral rami which cross the margin of the lateral atlanto-axial joint may be stretched over the edge of the atlanteal or axial articular process, during rotation of the atlas.50
As a result, compression to the nociceptive fibres of the C2 nerve root results in occipital pain. Studies have shown that the C2 nerve root contains proprioceptive afferent fibres from the tongue. These tongue proprioceptive fibres travel through an afferent loop involving the hypoglossal-lingual-cervical (C1-C3) fibres pathway called the ansa cervicalis-ansa hypoglossi loop. In addition, tongue proprioceptive fibres can also pass through the C1 and C3 nerve roots. Hence, compression of the tongue proprioceptive fibres in the C2 nerve root will result in tongue numbness.48 This syndrome can be treated conservatively or surgically.48 Surgical resection of the injured nerves in severe cases may only provide partial symptomatic relief.48 The neck-tongue syndrome has hardly been reported in dental literatures, yet dental surgeons should be aware of it.
9. Other miscellaneous local causes
Surgically-assisted rapid palatal expansion (SARPE),51 Eagle's syndrome,52 post third molar surgical infection,53 sialolithiasis54 and chronic sialoadenitis33 have all been reported to cause lingual nerve paraesthesia. They were presented in the literature as case reports, hence the prevalence is unknown. Nevertheless, they should become one of the differential diagnoses for lingual nerve neuropathy, although rare, and are placed lower in the surgical sieve ranking. The first cause is surgically related, while the last four causes are associated with the presence of pathology or an infection.
Surgically-assisted rapid palatal expansion (SARPE) is an effective surgical procedure performed to correct transverse maxillary deficiency in skeletally matured individuals.51 The case of interest here reportedly concerns numbness of both sides of the tongue of a 29-year old white male, which started on the 5th post-operative day. Chuah and Mehra postulated that some unusual event may have occurred to the lingual nerve at close proximity to the pterygoid plates in the pterygomaxillary region.51 Two possible mechanisms suggested were direct injury during pterygomaxillary osteotomies, and nerve compression from a haematoma in the pterygomaxillary region, which became displaced laterally when the patient performed manual expansion of the maxilla. This symptom was treated conservatively and resolved completely only by the 87th day post-operation.
Eagle's syndrome is characterized by various symptoms that include throat pain, pharyngeal foreign body sensation, dysphagia, referred otalgia, headache and neck and throat pain exacerbated by head rotation. Dong et al reported a case of a 59-year-old male with a 81.7 mm long giant styloid process, who suffered from hemitongue paraesthesia for over a decade.52 His left neck pain that previously radiated to the temporal and posterior cervical regions, together with the numb tongue, resolved after surgical removal of this elongated styloid process. So far, this is the only case of Eagle's syndrome that has been reported also to cause compression of the lingual nerve.
Late onset of neurosensory disturbance after third molar surgery has been defined as neuropathy that occurs between 1 day to 1 week post-operatively.55 This symptom is uncommon and has been related to oedema, trauma or post-operative infection. Kipp et al were among the first to report such presentation and, since then, there are many similar reports affecting the inferior alveolar nerve, but not the lingual nerve.55 So far, only Goldberg and Galbraith had reported one case that affected the lingual nerve alone.53 In this case, the patient began to experience sudden onset of anaesthesia of the right side of the tongue together with swelling and pain on the fifth post-operative day. Pressure over the lingual surface of the mandible inferior to the surgical area produced intense pain that radiated to her tongue. The infected socket was treated with irrigation and penicillin. By the eleventh post-operative day, all signs of infection had resolved, but lingual anaesthesia persisted. There was diminished sensation over her right tongue even after one year post-operation. They suggested inflammation and oedema of the neural sheath as the cause of lingual nerve neuropathy.
Sialolithiasis and chronic sialoadenitis are both pathologies that affect the salivary gland where, in the former, a calcified mass or calculus forms either within the salivary gland or, more commonly, in its duct. When the gland becomes infected, sialoadenitis sets in. Sialoadenitis can happen with or without the presence of a sialolith. At least two cases of lingual nerve neuropathy have been attributed to sialolithiasis.54 In one of these cases, the patient reported experiencing periodic hemilingual numbness that occurred approximately once every 2–3 weeks. The attacks were associated with a sensation of ‘fullness’ in the left submandibular region. A sialolith was discovered radiographically and was surgically removed. The authors hypothesized that intermittent obstruction of the submandibular duct by the sialolith led to proximal dilatation of the duct and submandibular gland with compression of the lingual nerve, hence the numb tongue sensation.54 Intermittent paraesthesia of the tongue has also been reported in a case of chronic sialoadenitis of the submandibular gland. The lingual nerve was reported to be embedded in scar, and symptoms resolved when the gland was removed surgically.33 As can be observed, the causes described under this category is uncommon and have been reported only as case reports.
Idiopathic or benign trigeminal sensory neuropathy is a rare disorder characterized by transient sensory disturbances (usually paraesthesia and/or anaesthesia) in the areas innervated by one or more branches of the trigeminal nerve, in the absence of other clinical features.56,57 It was first described in 1935 when Harris reported 3 cases from 853 trigeminal neuralgia patients who suffered rapid or sudden onset of complete numbness of one side of the face, eye, forehead, lips, jaws and tongue.58 The duration of the numbness varied from a few weeks to four years, but in each case the anaesthesia felt passed off completely, to be succeeded by paroxysmal trigeminal neuralgia of the same nerves. According to Fisher, pain (but not neuralgia) is present during the initial stages of the disease in approximately one-third of the cases.59 The association with trigeminal neuralgia has not been reported in recent literatures, but instead there appears to be an association with Facial-Onset Sensory Motor Neuronopathy (FOSMN), which is a malignant life-threatening condition.56,60 In general, there are three clinical subgroups of idiopathic trigeminal sensory neuropathy, the boundaries of which are not clearly defined, with diagnosis arrived at only after excluding all other possible causes, as outlined in this review. The three clinical subgroups of idiopathic trigeminal sensory neuropathy are:56,57
An acute primary form (acute idiopathic TSN);
A chronic form associated with connective tissue disease; and
A chronic idiopathic form.
The give-away symptom is the fact that abnormal sensation can begin in the lips or tongue but, after a few days, spread throughout the entire (bilateral) side of the face. In such a situation, cranial base tumour or a neoplasm of the trigeminal ganglion must be excluded.59 Shotts et al reported that only one-third of their patients had no underlying pathological problem.61 The remaining patients had distant malignancy (as described under ‘Tumour invasion and perineural spread’) or connective tissue disorder. Symptom-wise, one study reported that 70% of their patients presented with continuous facial numbness, with the remainder of patients experiencing intermittent symptom.57 Robinson et al found that these patients could be grouped into those with a connective tissue disorder, neurologic disease, psychologic problems, or a medical history of unknown significance.57 Of course the presence of these disorders makes arriving at a definitive diagnosis difficult. These patients should therefore be subjected to an array of investigations that include clinical assessment of cranial nerves, appropriate radiologic, and relevant haematologic and serologic investigations. Additional autoantibody essays to detect connective tissue disease may be undertaken if necessary. Histopathologic examination of lesion and labial gland tissue may also be done when appropriate.60,61 As lingual nerve neuropathy can be an early symptom of this condition, patients are best referred to an orofacial pain expert or a neurologist, if all common and uncommon causes outlined in this review have been ruled out.
Lastly, Silbert and Silbert reported an inflammatory type of trigeminal neuropathy which they compared to inflammatory brachial plexopathy (neuralgic amyotrophy or Parsonage-Turner syndrome).62 They suggested that this inflammatory trigeminal neuropathy is an important, but as yet under recognized, differential diagnosis for post-operative neurological symptoms in the dental setting. They reported of a case of a patient who developed numbness to the left tongue and lip immediately after surgical removal of all her third molars under general anaesthesia. The symptoms become worse on the third post-operative day, turning into allodynia that was exacerbated by movement of the jaw and tongue. Trismus set in by the fifth day. The patient's symptoms of discomfort became increasingly severe and, around the fourteenth day, the dysaesthesia and allodynia spread further to involve the left upper palate. Symptoms persisted and, at approximately 3 weeks post-operatively, she was commenced on prednisolone. Magnetic resonance imaging (MRI) performed a week later showed the presence of a small localized haematoma adjacent to the left mandibular foramen. She was subsequently referred to an orofacial pain specialist. Partial symptomatic improvement was achieved by a higher dose of prednisolone and pregabalin. Silbert and Silbert were of the opinion that the evolving neurological symptoms are the key to recognizing the diagnosis as inflammatory trigeminal neuropathy rather than an iatrogenic injury.62 They argued that iatrogenic injury will manifest early and improve with time, whereas inflammatory trigeminal neuropathy manifests the other way round. Worse, as observed in their case, another branch of the trigeminal nerve became involved with time. This suggested that the change was an immune-mediated condition but this cannot explain why it was unilateral.
Conclusion
In summary, lingual nerve neuropathy takes a sinister turn when a non-surgically-related cause can potentially be the aetiology. Some of these causes are benign, as in the case of post anaesthesia numbness and some types of idiopathic trigeminal sensory neuropathy. Others, such as tumour invasion and perineural spread of cancer, can be a very serious problem. Medical and dental practitioners should include these less common aetiologies in their differential diagnosis of lingual nerve neuropathy before diagnosing a patient's symptoms as an idiopathic trigeminal sensory neuropathy.
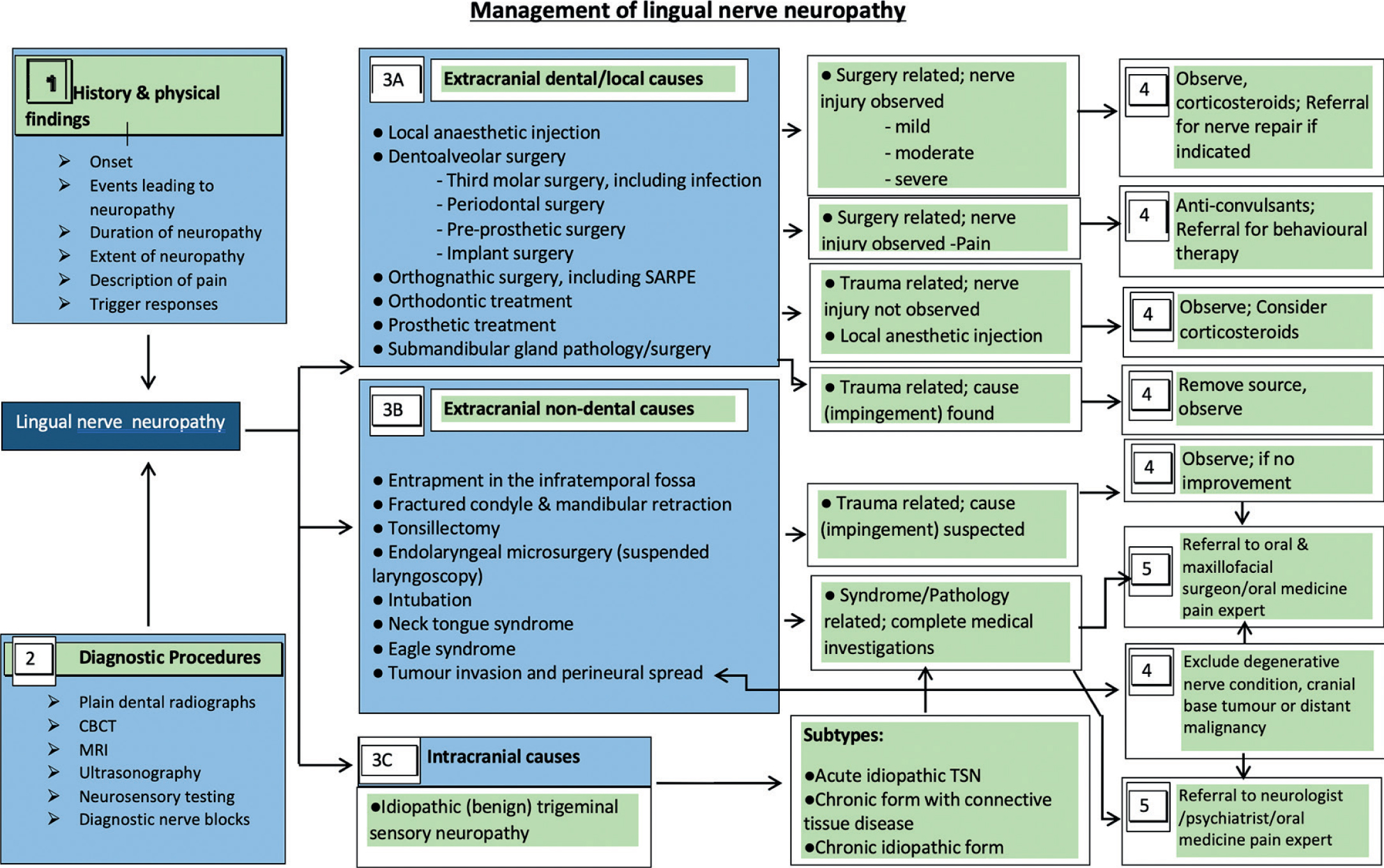
To end this review, a comprehensive algorithm for the diagnosis/management of lingual neuropathies to aid readers in decision-making, is provided (Figure 2).63 In essence, the current literatures advocates that any suspected or known surgical injury to the lingual nerve should be explored and repaired immediately. In less obvious cases, observation is recommended once neoplastic causes have been ruled out. Observation should include measuring the initial size of neuropathic area and looking out for changes in mechanosensory function. A consistent size and a lack of mechanosensory function are prognostic of poor outcome. Any lack of improvement after 3 months may be an indicator for surgical exploration.30 Having said so, pain caused by nerve injury does not normally respond to surgery, and may instead benefit from medical and behavioural therapy. Recommending surgery for these patients is ill advised.
Figure 2. A comprehensive algorithm for the diagnosis/management of lingual neuropathies adapted and modified from Decision Making in Oral and Maxillofacial Surgery63 to provide a guide to assist readers in making clinical decisions.