
Article

Cavity design is an important consideration in direct restorative dentistry: readers will be aware from their own clinical experience that large cavities fail more readily than small and that large cavities, especially in premolar teeth, may predispose to cusp fracture. Readers will also be aware that minimal non-retentive cavity design is really only possible using adhesive techniques and that recent improvements in dentine bonding agents have facilitated this.1
However, readers may not be aware of the work of a pioneer in minimal cavity design, Professor Richard Elderton, who first proposed a ‘new look at cavity design’ in a paper published in 1979.2 This was long before the era of adhesive dentistry, yet Elderton proposed serious deviations from GV Black's cavity designs and was roundly criticized for so doing in some quarters, as I recall. Yet his arguments had a basis in truth, as he stated that ‘a sizeable proportion of restorations at that time were found to fail in a few years', adding that ‘Black and generations of authors have erroneously led their readers to assume that the treatment that they prescribe would be successful in the long term’. He added that ‘teeth are small and their treatment requires attention to detail’.2
Ten years on, in an issue of Dental Update on ‘Dentistry in the year 2000’, Elderton published a paper on novel cavity designs.3 The first section of his paper was titled ‘Time to review cavity design’, the second ‘The move towards smaller cavities’. Readers can guess the premise for the article, minimally interventive cavities! He also added that there was no justification for extension for prevention. Among the cavity designs which he published were those illustrated in Figure 1 (published as in the original publication).3 These are undoubtedly minimal, but I have reservations with regard to whether the very narrow isthmus and occlusal design would actually work with amalgam. It required approximal grooves in the dentine of a Class II for retention. It would work with an adhesive resin composite, as was noted towards the end of the paper.
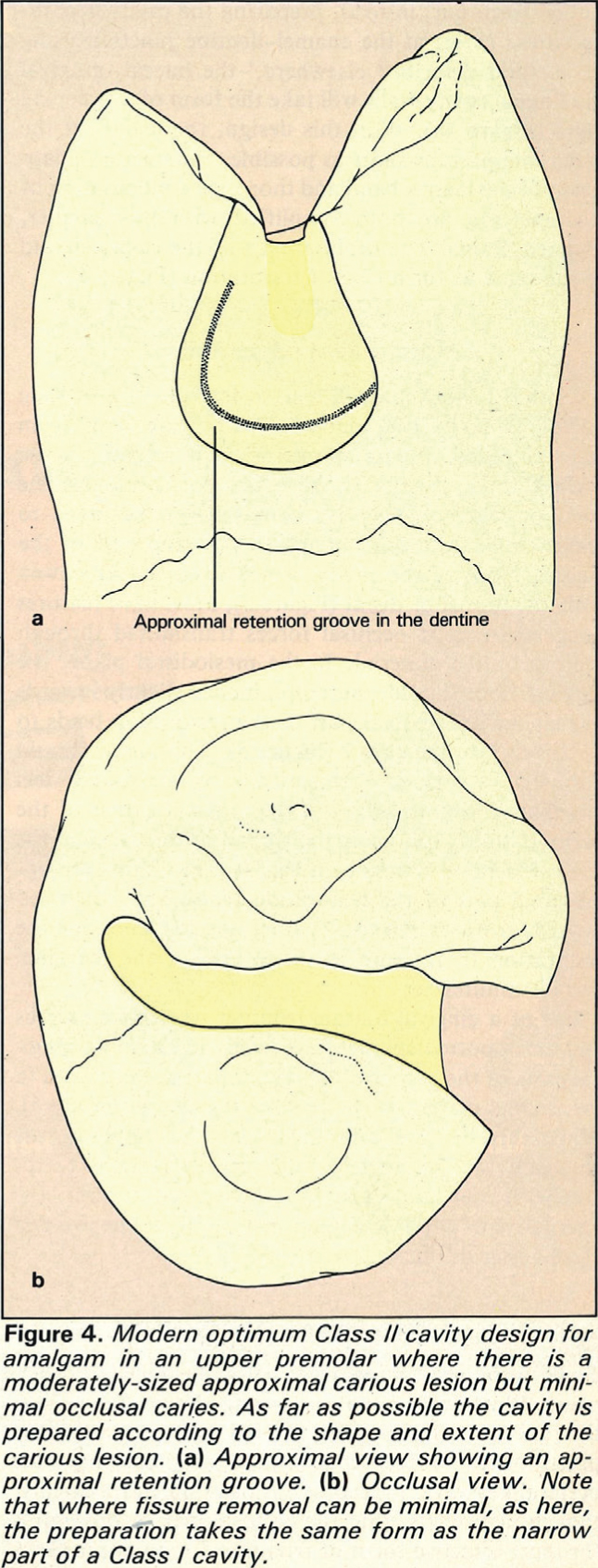
This paper, which should remain prescribed reading for all modern dentists but was published too early for the Dental Update website (which extends back 20 years) paved the way to a new look at cavity design.3 The message was clear – we should always be thinking of ways to reduce loss of tooth substance during cavity preparation (even if still using amalgam). In that regard, amalgam bonding could be considered, but the placement of grooves or slots within the interproximal box will help retain a minimal amalgam Class II in a maxillary second premolar tooth, as it did for one of my patients for 15 years (Figure 2). The interproximal grooves, however, present a risk of pulpal exposure if too deep, a risk that adhesive dentistry does not pose.
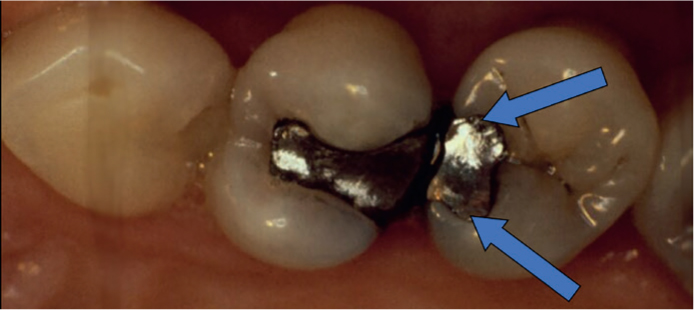
The Minimata Agreement, with its ban on amalgam in the under 15s, should embrace the concept of minimal cavity design for Class I and II restorations, because this can only really be done using adhesive techniques. Despite the work, 20 years ago, of Nordbo and colleagues,4 there remains a need for high quality cohort studies in the survival/success of restorations placed in mini Class II cavity designs. Only then will we know if the work of Richard Elderton, on the dangers of unnecessarily cutting extensive cavities, can produce successful, contemporary-design, minimal restorations in posterior teeth. However, even without such research, all readers will sense that keeping cavities as small as possible in ‘small teeth’ is bound to be a good thing, with an example of such a cavity being exhibited in a recent Dental Update publication.5 And, for those readers still wedded to amalgam for reasons of funding or personal preference (which results of a recent publication have indicated applies to circa 50% of restorations in posterior teeth in the UK6), there is always the minimal option illustrated in Figure 2 which does not destroy the strength of a premolar tooth in the way that a conventional cavity might.
Richard Elderton's work was 20 years ahead of its time, given that few embraced the concepts at the time of publication. His cavity concepts are an example to all of us who are faced with cutting cavities in teeth – keep the cavity as small as possible, whatever the material! Or better still, embrace prevention, then we might not have to cut the cavity at all!
Finally, readers will, I hope, have read the first pages on Dental Update's efforts to have readers advise other readers of events, good and bad, in the feature ‘I learnt about dentistry from that’, the concept being similar to the open reporting culture of the airline industry. I would be grateful for others to respond to this anonymous reporting of events so that we can all learn from them.