Weerheijm KL, Duggal M, Mejàre I, Papagiannoulis L, Koch G, Martens LC Judgement criteria for molar incisor hypomineralisation (MIH) in epidemiologic studies: a summary of the European meeting on MIH held in Athens, 2003. Eur J Paediatr Dent. 2003; 4:110-113
Silva MJ, Scurrah KJ, Craig JM, Manton DJ, Kilpatrick N. Etiology of molar incisor hypomineralization – a systematic review. Community Dent Oral Epidemiol. 2016; 44:342-353
Vieira AR, Kup E. On the etiology of molar-incisor hypomineralization. Caries Res. 2016; 50:166-169
Butler PM. Comparison of the development of the second deciduous molar and first permanent molar in man. Arch Oral Biol. 1967; 12:1245-1260
Tourino LF, Corrêa-Faria P, Ferreira RC, Bendo CB, Zarzar PM, Vale MP. Association between molar incisor hypomineralization in schoolchildren and both prenatal and postnatal factors: a population-based study. PLoS One. 2016; 11
Negre-Barber A, Montiel-Company JM, Boronat-Catalá M, Catalá-Pizarro M, Almerich-Silla JM. Hypomineralized second primary molars as predictor of molar incisor hypomineralization. Sci Rep. 2016; 6
Negre-Barber A, Montiel-Company JM, Catalá-Pizarro M, Almerich-Silla JM. Degree of severity of molar incisor hypomineralization and its relation to dental caries. Sci Rep. 2018; 8
Dantas-Neta NB, Moura LF, Cruz PF, Moura MS, Paiva SM, Martins CC Impact of molar-incisor hypomineralization on oral health-related quality of life in schoolchildren. Braz Oral Res. 2016; 30
Elhennawy K, Schwendicke F. Managing molar-incisor hypomineralization: a systematic review. J Dent. 2016; 55:16-24
Elhennawy K, Jost-Brinkmann PG, Manton DJ, Paris S, Schwendicke F. Managing molars with severe molar-incisor hypomineralization: a cost-effectiveness analysis within German healthcare. J Dent. 2017; 63:65-71
Souza JF, Jeremias F, Costa-Silva CM, Santos-Pinto L, Zuanon ACC, Cordeiro RCL. Aetiology of molar-incisor hypomineralisation (MIH) in Brazilian children. Eur Arch Paediatr Dent. 2013; 14:233-238
Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013; (7)
Fragelli CM, Souza JF, Jeremias F, Cordeiro ReC, Santos-Pinto L. Molar incisor hypomineralization (MIH): conservative treatment management to restore affected teeth. Braz Oral Res. 2015; 29:1-7
Temilola OD, Folayan MO, Oyedele T. The prevalence and pattern of deciduous molar hypomineralization and molar-incisor hypomineralization in children from a suburban population in Nigeria. BMC Oral Health. 2015; 15
Elfrink ME, Veerkamp JS, Aartman IH, Moll HA, Ten Cate JM. Validity of scoring caries and primary molar hypomineralization (DMH) on intraoral photographs. Eur Arch Paediatr Dent. 2009; 10:5-10
Kopycka-Kedzierawski DT, Meyerowitz C, Litaker MS, Heft MW, Tasgaonkar N, Day MR Management of dentin hypersensitivity by practitioners in the National Dental Practice-Based Research Network. J Am Dent Assoc. 2017; 148:728-736
Lygidakis NA, Wong F, Jälevik B, Vierrou AM, Alaluusua S, Espelid I. Best Clinical Practice Guidance for clinicians dealing with children presenting with Molar-Incisor-Hypomineralisation (MIH): an EAPD Policy Document. Eur Arch Paediatr Dent. 2010; 11:75-81
Najeeb S, Khurshid Z, Zafar MS, Khan AS, Zohaib S, Martí JM Modifications in glass ionomer cements: nano-sized fillers and bioactive nanoceramics. Int J Mol Sci. 2016; 17 https://doi.org/10.3390/ijms17071134.20
Grossi JA, Cabral RN, Ribeiro APD, Leal SC. Glass hybrid restorations as an alternative for restoring hypomineralized molars in the ART model. BMC Oral Health. 2018; 18
Ashima G, Sarabjot KB, Gauba K, Mittal HC. Zirconia crowns for rehabilitation of decayed primary incisors: an esthetic alternative. J Clin Pediatr Dent. 2014; 39:18-22
Clark L, Wells MH, Harris EF, Lou J. Comparison of amount of primary tooth reduction required for anterior and posterior zirconia and stainless steel crowns. Pediatr Dent. 2016; 38:42-46
Innes N, Evans D, Hall N. The Hall Technique for managing carious primary molars. Dent Update. 2009; 36:472-478
Innes NP, Evans DJ, Stirrups DR. The Hall Technique; a randomized controlled clinical trial of a novel method of managing carious primary molars in general dental practice: acceptability of the technique and outcomes at 23 months. BMC Oral Health. 2007; 7
Seale NS, Randall R. The use of stainless steel crowns: a systematic literature review. Pediatr Dent. 2015; 37:145-160
Williams JK, Gowans AJ. Hypomineralised first permanent molars and the orthodontist. Eur J Paediatr Dent. 2003; 4:129-132
Jälevik B, Möller M. Evaluation of spontaneous space closure and development of permanent dentition after extraction of hypomineralized permanent first molars. Int J Paediatr Dent. 2007; 17:328-335
Alexander SA, Askari M, Lewis P. The premature loss of primary first molars: space loss to molar occlusal relationships and facial patterns. Angle Orthod. 2015; 85:218-223
Treatment options for deciduous molar hypomineralization: a report of three cases Yasmy Quintero Manuel Restrepo Jenny Angélica Saldarriaga Alexandra Saldarriaga Lourdes Santos-Pinto Dental Update 2024 46:6, 707-709.
Authors
YasmyQuintero
DDS
PhD student at São Paulo State University (UNESP), School of Dentistry, Araraquara, Brazil
Deciduous molar hypomineralization (DMH) is an enamel defect of systemic and multifactorial origin that affects the second deciduous molar. Currently, its treatment is based on guidelines for Molar Incisor Hypomineralization (MIH), a disturbance that affects permanent molars and may or may not be associated with permanent incisors. To date, there are no guidelines for DMH. Therefore, three different therapeutic approaches are presented to treat DMH, emphasizing the relevance of early diagnosis, differential diagnosis and treatment options, and tailored to take into account each patient's and parents' specific needs, as well as the involved tooth, severity of DMH, patients' symptoms and behaviour.
CPD/Clinical Relevance: To understand the clinical implications of DMH since the diagnosis and delayed treatment of this enamel alteration could have important complications in both the primary and permanent dentition.
Article
Deciduous Molar Hypomineralization (DMH) is an enamel defect of multifactorial origin that affects 1 to 4 second deciduous molars, and may be associated with canines and first deciduous molars.1 Similar to Molar Incisor Hypomineralization (MIH), which affects enamel in 1 to 4 first permanent molars, and occasionally permanent incisors, enamel affected by DMH presents demarcated opacities that vary from white to yellowish or brownish colour, affecting part or all tooth surfaces. A typical feature of the affected teeth is an asymmetrical appearance, with one molar being severely affected while the contralateral tooth is unaffected.2
The aetiology of DMH and MIH is not fully understood, and the currently available scientific evidence is insufficient to establish causality.3, 4 The formation of the second deciduous molar, the first permanent molar, and the permanent incisor, which is initiated before birth and occurs between the first and third year of life, can be affected by environmental factors, including common childhood diseases, long-term breastfeeding and respiratory tract problems during the third trimester of pregnancy to up to three years of age.5, 6 Since the development of the second primary molars and first permanent molars overlap in time, a possible association between DMH and MIH has been previously proposed.6 While this association is not clear, children with DMH are 4 to 5 times more likely to present with MIH.7 Since the eruption of the second deciduous molar occurs approximately 4 years before the eruption of the first permanent molar, DMH could be a predictor of MIH.7
Depending on the extent and severity of the opacities, hypomineralized teeth may exhibit dental sensitivity, post-eruptive fractures, dental caries lesions, atypical restorations and exodontia,2, 8 which may interfere with a patient's quality of life.9 Treatment options range from non-surgical treatment, including diet control, remineralizing agents and micro-invasive procedures, to invasive treatments with composite resin, steel crowns and exodontias.10 The elected treatment should consider a patient's age, severity of hypomineralization, symptoms, treatment cost-benefit ratio, and a patient's and parents' expectations.11
Although there are no specific guidelines for the management of DMH, current treatment follows the same recommendations established for MIH, where maintaining deciduous tooth integrity is important as it contributes to proper bone development, mastication, phonation, occlusion and aesthetics in paediatric patients. Thus, the objective of this report is to present three DMH cases, and to describe the individual treatment implemented based on severity of disease and type of patient.
Case reports
Three paediatric patients diagnosed with DMH were treated at the IPS CES Sabaneta Clinic (Colombia). The biological parents provided signed informed consent, and were administered a structured questionnaire12 addressing issues of pregnancy and the child's early life (Table 1). For each case, treatment was designed taking into consideration age, disease severity, family's socio-economic conditions, patient's behaviour and parents' expectations. Clinical assessment was performed with artificial light, and complementary diagnostic aids if required.
Medical History
Prenatal
Perinatal
Postnatal
Not reported
Maternal hypoxia
Allergic conjunctivitis treated with olopatadine
Amoxicillin and iboprufen during fourth gestational month after exodontia of third molarAcetyl salicylic acid for miscarriage risk from week 0–34
Complicated birth, neonatal hypoxia
Bronchiolitis at 1 month of age
Use of salbutamol inhaler
Recurrent acute respiratory tract infections
Fever
Use of antihistamines from 6–18 months of age
Streptococcal stomatitis at 1st year of age
Amoxicillin
Progesterone from threat of miscarraige from weeks 10–32
Low birthweight
Acute respiratory disease treated with amoxicillin and clavulanic acid
Fever
Chronic allergic rhinitis controlled with antihistamine
Case 1
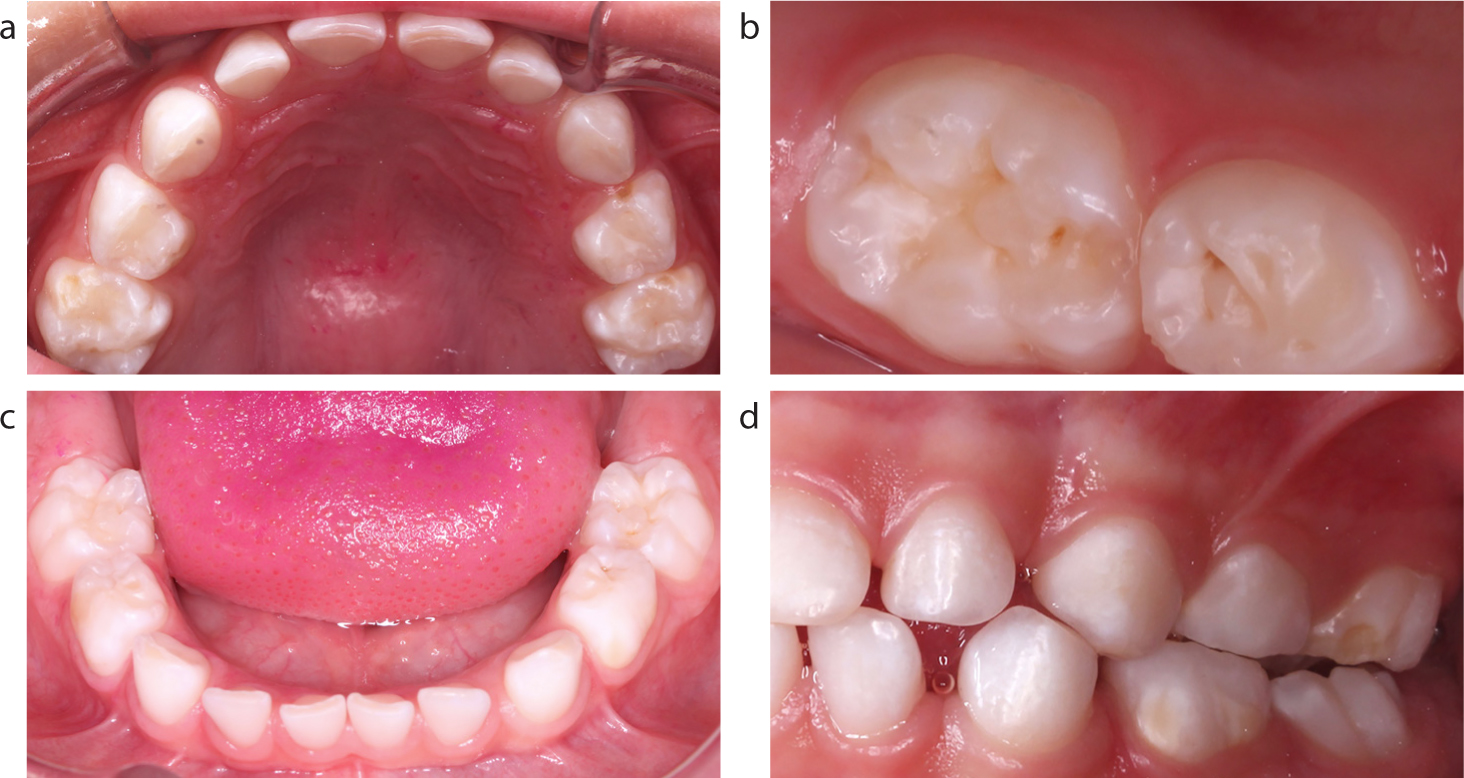
A 4-year-old male patient presented to the paediatric dentistry clinic because his parents were concerned about white spots on his teeth. Dental examination revealed hypomineralization in the upper and lower deciduous molars and canines, characteristic of mild DMH (Figure 1). URE had a fractured vestibular surface with slight enamel loss that could be cleaned easily, avoiding accumulation of dental biofilm, and without compromising tooth function or sensitivity. Therefore, this case was classified as mild HMD.
Figure 1. Case 1: Non-surgical treatment of mild DMH. (a–c) Mild DMH on teeth URE, ULC, LLD, LLE, LRD and (d) demarcated opacity with loss of structure in the vestibular surface of ULE.
A non-surgical treatment focusing on control of risk factors, such as consumption of carbohydrates and brushing with 1,450 ppm fluoridated toothpaste, was implemented. In addition, dental prophylaxis with rubber cup and prophylactic paste (Proquident, Envigado, Colombia), as well as application of fluoride varnish (Duraphat® Colgate, New York, USA), were part of this patient's treatment plan; the application of fluoride was carried out as a risk control measure for dental caries.13 Screening was performed every three months. At the first control appointment, no enamel fracture was observed in the affected tooth.
Case 2
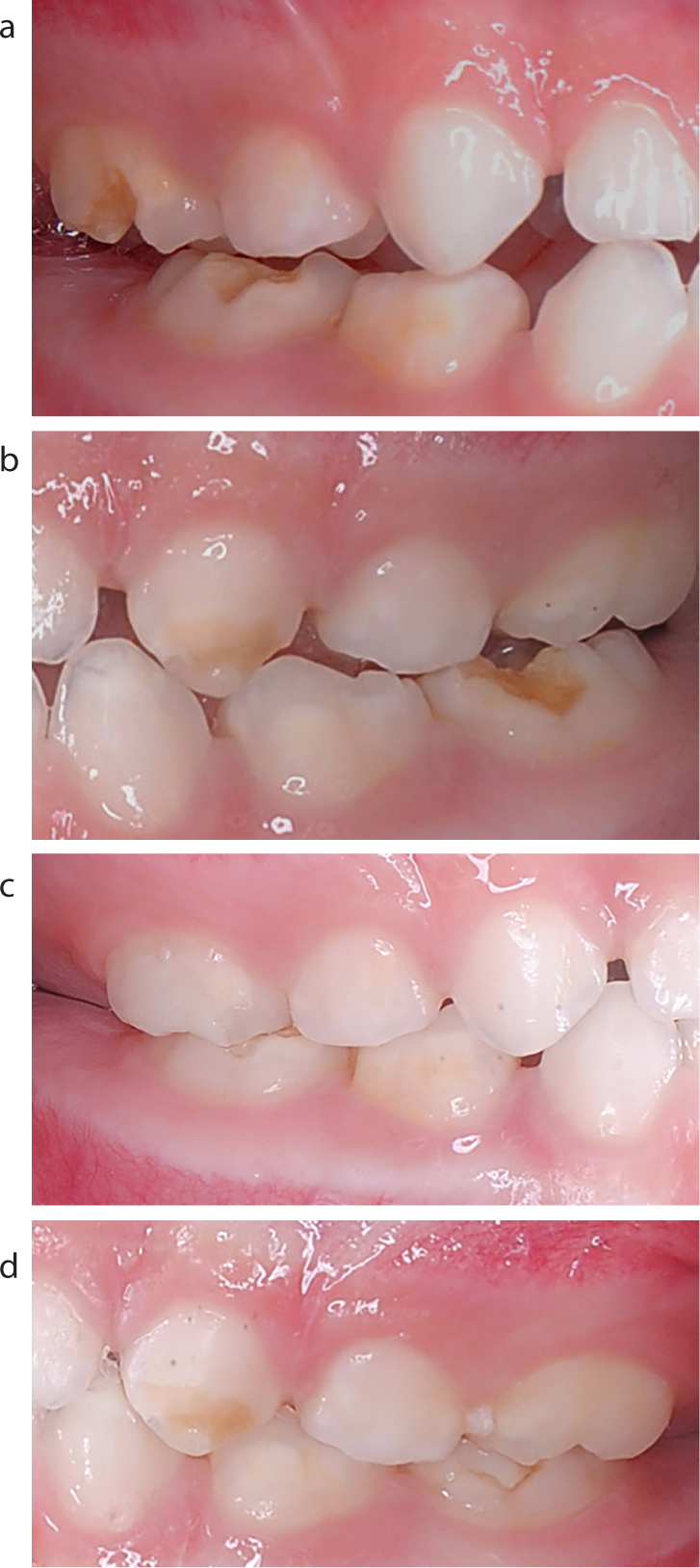
A 4-year-old male patient, presenting negative behaviour, active nail and solid structure biting habits, loss of tooth structure in teeth URE, LLE and LRE, and with dentinal sensitivity, was diagnosed with severe DMH in deciduous molars and canines (Figures 2a, b).
Figure 2. Case 2: Non-surgical and surgical treatment of severe DMH. (a) White, demarcated opacities, without loss of dental structure in vestibular surface were identified in teeth URD, URC, LRC, and LRD and (b) ULC, ULE, LLE, LLD and LLC were non-surgically treated. Severe DMH demarcated opacities and enamel loss in (a) URE, LRE and (b) LLE were surgically treated with nano-filled resin-modified glass ionomer cement (c, d).
For this patient, treatment was aimed at preserving his dental structure, relieving symptoms, and improving his behaviour. Initially, a non-surgical treatment, as described for Case 1, was implemented (Figures 2a, b). Teeth with loss of dental structure (URE, LLE, and LRE) were temporarily restored (Figures 2c, d) with nano-filled, resin-modified, glass nanoionomer cement (Ketac™ N100, 3M ESPE, New York, USA) following manufacturer's instructions.
During the follow-up period, while temporary restorations of teeth URE, LLE, and LRE were found fractured at every visit, there was no compromise of the remaining dental structure. Additionally, the parents were informed that the dental sensitivity had significantly decreased. After six months of follow-up, his symptoms had improved and the remaining dental structure was intact.
Case 3
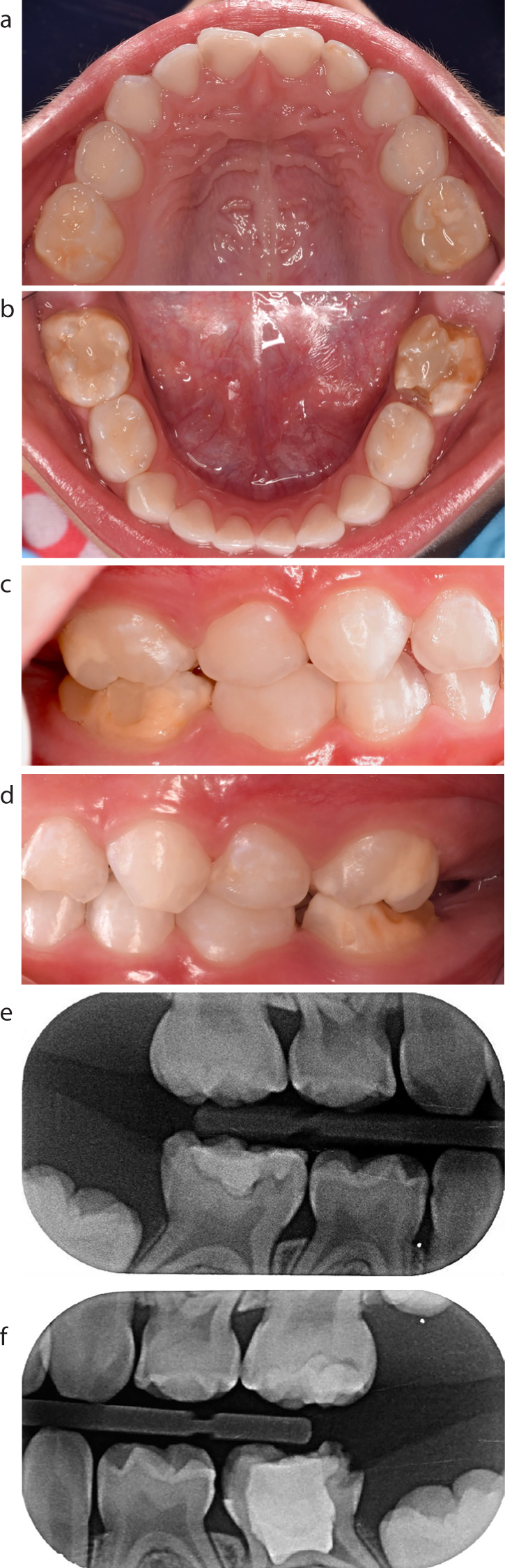
A 5-year-old female patient was brought to our dental clinic with her parents complaining that she had a ‘really ugly tooth, the filling is always falling off, it hurts, and it's breaking’. The parents and the patient attended the consultation requesting a treatment with durability and high aesthetics. The patient had a dental history of pulpotomy on tooth LLE (Figure 3b). The patient complained of hypersensitivity and that it was difficult to brush teeth and eat. Nonetheless, she presented with positive behaviour. Based on clinical and radiological findings (Figure 3e, 3f), this patient was diagnosed with severe DMH (Figure 3a–d).
Figure 3. Case 3: Severe DMH. (a) Minimal restoration of occlusal and palatal surface of ULE. (b, c) Fractured restoration with loss of structure, with white and brown opacities on LLE and LRE. (a-d) White and yellow opacity without loss of structure on URE, URC, ULC, ULD, ULD, LLD, LLD, LRD and LRC. (e, f) Initial interproximal radiograph, initial dental caries distal surface LLD and LRC, initial dental caries mesial LLD.
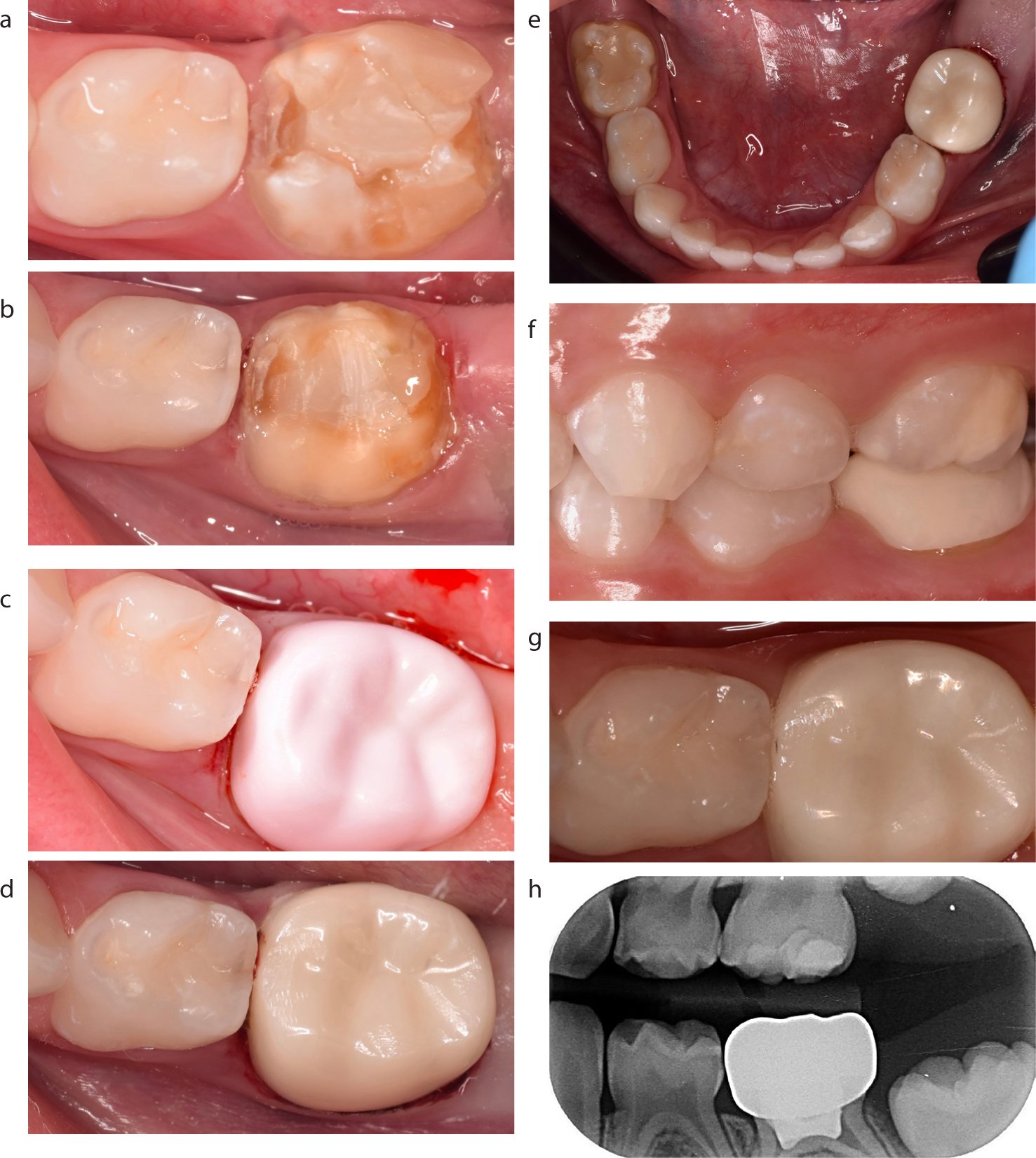
For this patient, an initial non-surgical preventive treatment for teeth without dental structure loss was implemented, as described for the previous cases (Figures 3a, b). Teeth ULE and LRE presented moderate enamel loss that was restored with glass ionomer cement (Ketac™ Molar Easymix, 3M ESPE, New York, USA), as described by Fragelli et al.14 As shown in Figure 4a, a zirconia dental crown (NuSmile®, Houston, USA) was used on tooth LLE. Topical anaesthesia (Garhocaína®, Bogotá, Colombia) was applied for 2 minutes on the buccal mucosa sulcus, and local anaesthetic using lidocaine with 2% epinephrine (New Stetic®, Antioquia, Colombia). Subsequently, the crown was prepared with a high-speed diamond bur (Jota®, Switzerland) by initially grinding 0.5 mm from the buccal and lingual cusps, followed by 0.5 mm deep buccal and lingual cuts, and proximal surface reduction of 1.5 mm performed with a black line diamond bur.
Figure 4. Case 3: Severe DMH treated using a zirconia crown. (a) Severe DMH on LLE. (b) Dental preparations. (c) Zirconia crown tried in with pink pigment and (d) cemented. (e–g) Clinical and radiological follow-up after 6 months of zirconia crown cementation. (h) Radiograph shows caries progression in LLD.
Scuffs were levelled and occlusal fit was verified by performing the pink pigment test (Figure 4c). The shoulder of the finish line was removed with a green-line diamond bur, extending the preparation to the sub-gingival level in a knife-edge configuration. Next, the crown was cemented with resin-modified glass ionomer cement (RelyXTM Luting 3M®, Sao Paulo, Brazil) following manufacturer's instructions (Figure 4d).
At 6-month (Figure 4) and 1-year (Figure 5) clinical and radiological follow-up, the crown on LLE showed proper adaptation, periodontal integrity, and no changes in structure or colour. Furthermore, no alterations were observed in antagonist teeth. The distal surface of LLD (Figure 4h) showed progression of dental caries without surface cavitation, so that education measures were increased. During the one-year follow-up, the eruption of the lower left first permanent molar with white opacity without loss of tooth structure was observed (Figures 5a–c). On the distal occlusal surface of LLD, progression of dental caries was found, with cavitation of the surface; this was restored with adhesive material and habits of diet and toothbrushing were reinforced.
Figure 5. Case 3: Severe DMH – zirconia crown on LLE. (a–c) Clinical and radiological follow-up after one year of zirconia crown cementation. Eruption of the lower left first permanent molar with white opacity without loss of tooth structure.
Discussion
Hypomineralization is a condition that may lead to clinical, functional and aesthetic discomfort, as well as to a greater need for dental treatment, particularly in severe cases. The prevalence DMH ranges from 4.6%15 to 21.8%.16 Currently, there are no clinical guidelines describing treatment options for DMH, making its treatment challenging for the general and paediatric dentist, and possibly leading to under- or over-treatment of teeth affected by DMH.
Treatment of hypomineralization of deciduous and permanent teeth is a clinical challenge. In addition to taking into account severity, symptoms, dental age, cost-benefit, and patients' expectations,3 choice of treatment must also consider patients' behaviour. Furthermore, the majority of research on hypomineralization treatment options is usually done on permanent teeth,10 and those results have been extrapolated to deciduous teeth.
The recommended guidelines for MIH10 were applied for the patient presenting with mild DMH (Case 1). Educational measures for parents and patient were prioritized, aiming to motivate and raise awareness of the importance of proper oral hygiene and eating habits. As a complementary measure, 5% fluoride varnish was applied. The use of this product in patients with hypomineralization is intended to increase calcium and fluoride ion release, control hypersensitivity,17 and control development of dental carious lesions.13
For severe DMH cases, implementation of health promotion and sugar control is recommended, together with preventive or minimally invasive restorations through the use of occlusal sealants, glass ionomer cement restoration, resin composites, steel crowns, exodontias, and/or orthodontic treatment.18 Cases 2 and 3 (Figures 2 and 4) presented deciduous molars with severe lesions. However, three factors determined the final choice of treatment: reason for consultation, patient's and parents' expectations of treatment, and patient behaviour.
For the patient described in Case 2 (severe DMH), nano-filled, resin-modified, glass ionomer cement was used since, in addition to having conventional glass ionomer cement properties, it has been shown to exhibit proper physical and mechanical properties19 which, in this case, were required given the severity and location of the lesions (Figures 2a and b). In addition, those teeth had a history of unsuccessful restoration using high-viscosity glass ionomer cement, hence the need for an adhesive material. The restoration with glass ionomer cement was made temporarily for the purpose of preserving the molar20 while seeking a more positive patient behavioural response.
The patient described in Case 3, with severe DMH on tooth LLE, presented with pain, loss of structure, recurrent failure of adhesive restoration and aesthetic concern was expressed by the parents. In this context, a more invasive approach was taken in order to reduce the number of interventions and to improve aesthetics. Therefore, the treatment included a preformed zirconia crown, which is considered a simple and effective treatment that shows good long-term benefits.21 Compared to other commercially available brands, NuSmile® requires less tooth reduction.22 On the other hand, this technique removes fragile dental tissue, leaving the remaining dental structure in optimal condition. After one year of follow-up, the parents and the patient were satisfied with the treatment and, in addition, periodontal integrity, marginal adaptation, occlusal fit and colour stability were observed during clinical evaluation. Nonetheless, further longitudinal studies are required in order to evaluate this type of treatment, as well as its cost-benefit ratio for DMH treatment.
For molars severely affected by DMH with dental sensitivity, post-eruptive fractures and/or dental caries lesions affecting more than two surfaces, stainless steel crowns are one of the treatment options. The ‘Hall technique’ is a non-invasive approach, in which an appropriately sized steel crown is seated on the tooth by digital pressure and cemented with glass ionomer cement, without prior use of local anaesthesia, tissue removal (carious or hypomineralized) or tooth preparation.23 Despite the clinical and biological benefits of this method,24, 25 and having been offered to parents as the first treatment option of the patients described in Cases 2 and 3, it was not accepted due to unfavourable aesthetics.
For severe MIH cases, in which considerable structure loss is evidenced, exodontia is a treatment option at an ideal age. Elhennawy and colleagues argue that, in these cases, the approach presents an adequate cost-benefit ratio, since preserving teeth with severe defects would increase costs for patients in the long run and it would be more effective to perform an extraction and implement an early orthodontic treatment.11 However, any extraction of a permanent first molar should consider the ideal dental age for this to be performed, which has been recommended between 8.5 and 9 years of age,26 to allow the migration of the second permanent molars in the position of the first permanent molar to establish an ‘acceptable’ occlusion,27 and orthodontic treatment may not be necessary.
For severe cases in deciduous teeth, exodontia may also be a choice of treatment. However, the implications of the premature loss of the second deciduous molar, and the occlusal, skeletal, functional and behavioral consequences should be considered.
Finally, the importance of early diagnosis of DMH and differential diagnosis with other enamel defects and dental caries is emphasized, as well as the need for providing patients and parents with the necessary education and awareness to establish a conservative treatment plan, for which it is necessary to establish clinical guidelines that consider symptoms, severity, cost-benefit ratio and patient behaviour.28
Conclusions
Choice of treatment for teeth with DMH should take into account the individual condition of each patient and of each tooth, as well as parents' needs and expectations.
Treatment plans for all DMH cases, regardless of severity, should include health promotion and education measures for the control of this disorder
Restorative treatment with nano-filled, resin-modified, glass ionomer cement is a minimally invasive procedure that allows temporary restoration of teeth with mild DMH defects.
Zirconia crown is an option for treatment of severe DMH cases when adhesive procedures fail or are not indicated, as well as when resistance, durability, and aesthetics are required.