Clark RKF, Radford DR, Juszczyk AS. Current trends in removable partial denture teaching in British dental schools. Br Dent J. 2011; 211:531-535
Puryer J, Woods K, Terry J, Sandy J, Ireland AJ. The confidence of undergraduate dental students when carrying out prosthodontic treatment and their perception of the quality of prosthodontic education. Eur J Dent Educ. 2018; 22:e142-e148
Turner JW, Moazzez R, Banerjee A. First impressions count. Dent Update. 2012; 39:455-471
Jacobson TE, Krol AJ. A contemporary review of the factors involved in complete denture retention, stability, and support. Part I: Retention. J Prosthet Dent. 1983; 49:5-15
Guides to Standards in Prosthetic Dentistry – Complete and Partial Dentures. Guidelines in Prosthetic and Implant Dentistry. 1996; 7-11
Pietrokovski J, Kaffe I, Arensburg B. Retromolar ridge in edentulous patients: clinical considerations. J Prosthod. 2007; 16:502-506
Ismail YH, Bowman JF. Position of the occlusal plane in natural and artificial teeth. J Prosthet Dent. 1968; 20:407-411
Jayachandran S, Ramachandran CR, Varghese R. Occlusal plane orientation: a statistical and clinical analysis in different clinical situations. J Prosthod. 2008; 17:572-575
Shetty S, Zargar NM, Shenoy K, Rekha V. Occlusal plane location in edentulous patients: a review. J Ind Prosthod Soc. 2013; 13:142-148
Neill D, Glaysher J. Identifying the denture space. J Oral Rehabil. 1982; 9:259-277
The Glossary of Prosthodontic Terms. J Prosthet Dent. 2017; 117:1-105
Jacobs RM, Brodie AG. Tonic and contractile components of the oral vestibular forces in young subjects with normal occlusion. Am J Orthod. 1966; 52:561-575
Gahan M, Walmsley A. The neutral zone impression revisited. Br Dent J. 2005; 198:269-272
Lynch CD, Allen PF. Overcoming the unstable mandibular complete denture: the neutral zone impression technique. Dent Update. 2006; 33:21-26
McCord JF, Grant AA. Prosthetics: Registration: Stage II – intermaxillary relations. Br Dent J. 2000; 188
Complete denture series part 2: tips on how to correct 10 avoidable errors Sivakumar Jayachandran Wouter Leyssen A Damien Walmsley Dental Update 2024 46:6, 707-709.
Authors
SivakumarJayachandran
MDS, BDS, AFHEA
Specialty Dentist and PhD Student, Prosthetic Dentistry, School of Dentistry, University of Birmingham, 5 Mill Pool Way, Edgbaston, Birmingham B5 7EG, UK
The first article of this series identified the common reasons for referral for complete denture patients to secondary care. With this background, this article provides general dental practitioners (GDPs) with clinical tips to avoid the common errors whilst making complete dentures.
CPD/Clinical Relevance: The use of the clinical tips may help GDPs to improve their clinical success in treating complete denture patients and, in turn, aim to avoid improper referrals to secondary care.
Article
Complete denture prosthodontics remains a difficult clinical procedure in general dental practice. This has been illustrated by the number of referrals received at Birmingham Dental Hospital for the provision of complete dentures, which are deemed ‘too complex to treat’. Changes in the dental curriculum to accommodate recent advancements in other fields of dentistry have reduced the time available for teaching complete denture prosthodontics.1 This has resulted in low confidence levels in treating patients who, in turn, are becoming frustrated with care in general dental practice.1, 2
In our previous article, the reasons for the referral of edentulous patients to Birmingham Dental Hospital were analysed. The referral letters from GDPs indicated that they were faced with a range of difficulties. The clinical records of the referred patients were reviewed and data collected. The main reasons for referring a patient to secondary care were issues with resorption of the mandibular ridge and looseness (Table 1). The group of ill-defined reasons (28%) are listed in Table 2.
Resorption lower ridge (39%)
Ill-defined reasons (28%)
Looseness (25%)
Pain (11%)
Immediate dentures (8%)
Exaggerated gag reflex (7%)
Implants (7%)
Denture rubbing
Unable to eat salad/apple
Unable to masticate
Speech problems
Unhappy with fit
Not able to tolerate any dentures
Stroke
Cheek biting
Difficulties to fit denture around mandibular tori
The aim of this article is to address the common errors that can affect success of complete dentures and to provide the clinical tips to general dental practitioners. These tips could provide a guide in avoiding common mistakes.
Error 1: Poor adaptation to the denture-bearing area
Forty-one percent of failing complete dentures assessed at our New Patient Clinics between October 2016 and March 2017 showed poor adaptation to the denture-bearing area. This may result in a rocking movement of the denture which affects stability. Information gained from patient verbal histories indicated that it is common practice to use a single impression using alginate impression material in a stock tray in general dental practice. This might provide acceptable results for patients with sufficient ridge height but often fails to capture the relevant anatomy for patients with more advanced ridge resorption.3 In practical terms, a two stage technique will assist a clinician in perfecting the adaption of a tray to those difficult ridges. A low viscosity alginate more often than not fails to capture sufficient outline of the ridges and the lingual sulcus depth for ridges (Atwood Classification V and VI). A primary cast made from a muco-displasive impression material, such as a thick mix of alginate, silicone putty impression material or impression compound, can be of help. Personalized special trays constructed from the primary cast often make it easier for the clinician to produce dentures that adapt better to the denture-bearing area.
Clinical Tip
To use primary and secondary impressions as good practice in order to record the functional sulcus depth and width
To communicate this information to the technician and thus achieve an appropriate flange width and depth in the finished denture
Error 2: Inappropriate denture extension
Many patients referred to Birmingham Dental Hospital presented with a new denture with inappropriate extensions. The dentures were either over extended or under extended in the areas listed in Table 3.
Over Extensions
Under Extensions
Anterior and buccal flanges of upper and lower dentures (especially for patients with advanced resorption patterns)
Anterior lingual flanges of lower dentures
Upper posterior buccal flanges
Disto-lingual flanges of the lower dentures
Posterior extension of lower dentures
Posterior extension of upper dentures
Anterior buccal flanges of upper dentures (for patients with limited buccal resorption eg immediate dentures)
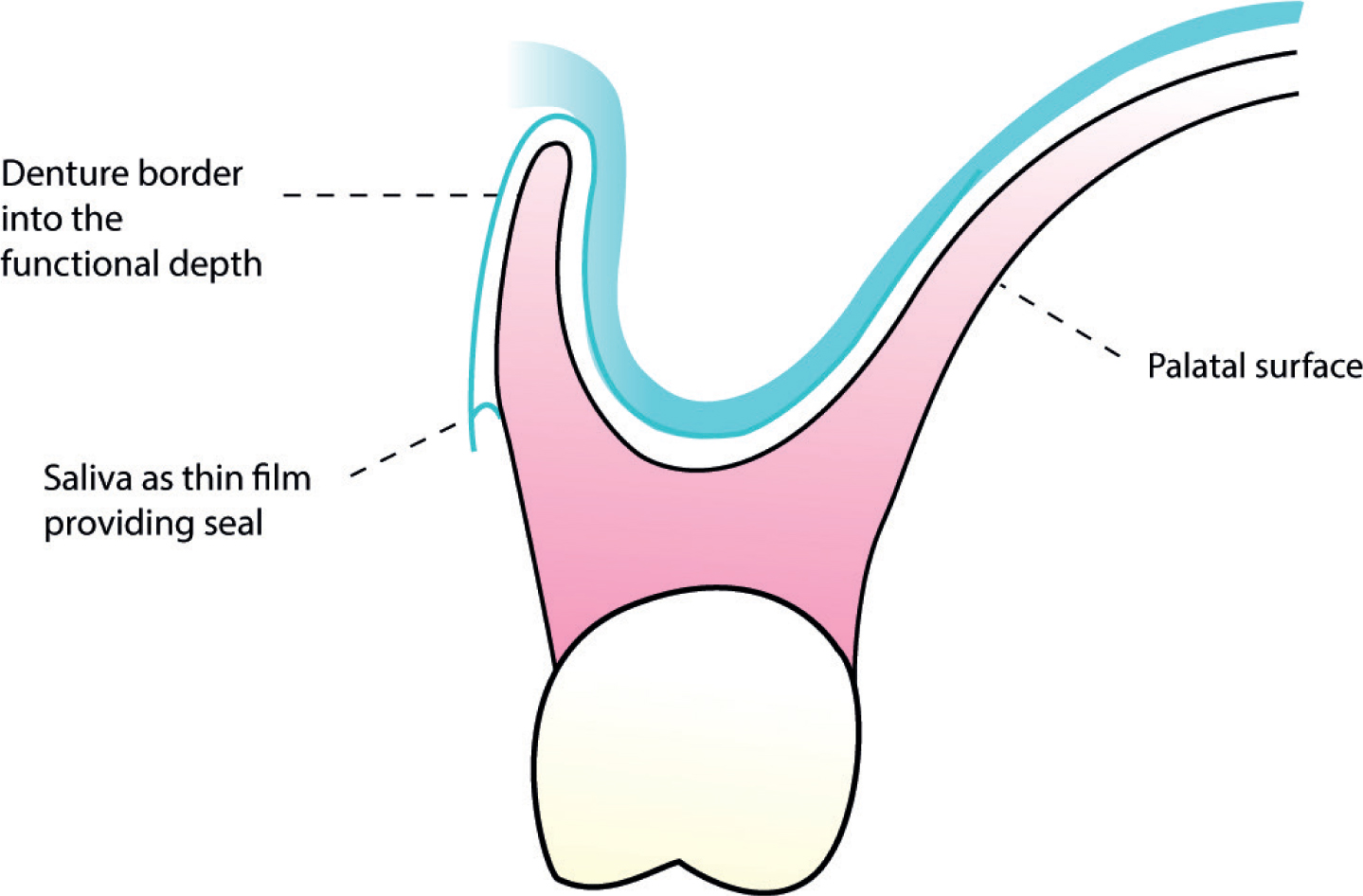
Functional depth and peripheral seal are the two common factors related to denture retention. The flanges of a denture should ideally fill the functional sulcus in terms of both the depth and the width4 (Figure 1). BSSPD Guidelines say that ‘Impressions should be boxed or the borders marked appropriately before the casts are poured to preserve an accurate record of the functional depth and width of the sulci.’5
Figure 1. Functional depth-width and denture border.
The border extensions could be adjusted and remodelled using chairside resin reline material or greenstick impression compound.
It seems to be a common occurrence to omit the labial flanges of the upper denture when providing immediate replacement dentures in general practice. An explanation could be the bulkiness of the anterior ridge and the labial fullness or difficulties capturing the sulcus during impression taking. Socket fitted dentures are favoured by technicians although, where possible, a flange should be placed to aid future retention. If subsequent dentures follow a socketed design, then the under-extension may be copied. At a later stage, when appropriate extensions are required for optimal retention, the patient may not like or tolerate these flanges. They may not like the change in appearance and the sensation that the upper lip is pushed out.
Clinical Tip
The border of the impressions can be clearly marked (Figures 2 and 3) to indicate the depth and width of the sulcus to be maintained, before sending them to the laboratory. The technician can easily transfer this to the master cast and then to the finished denture.
Figure 2. Border extension clearly marked for the attention of the dental technician (maxilla).Figure 3. Border extension clearly marked for the attention of the dental technician (mandible).
Error 3: Inadequate border relief
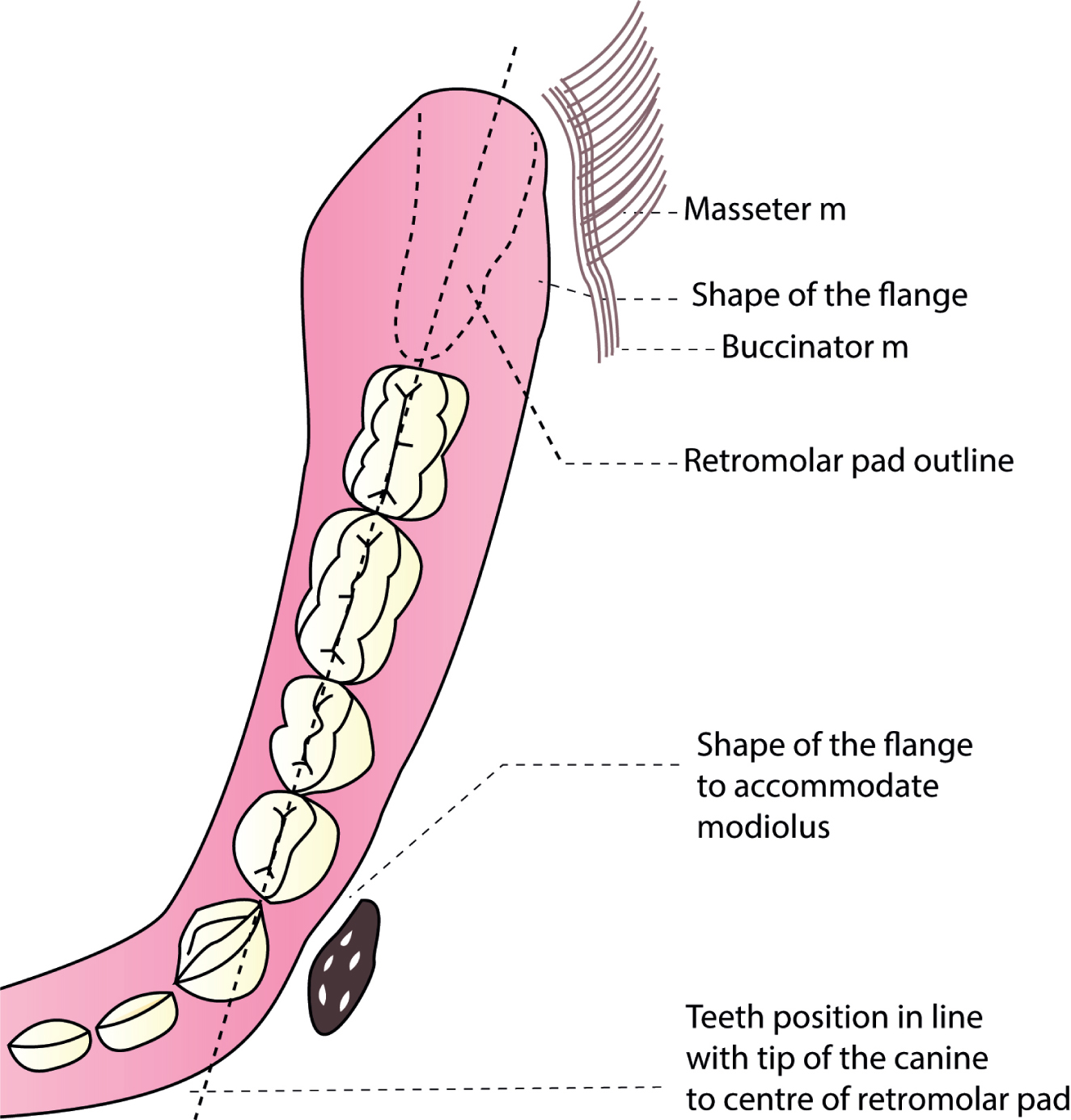
The frena and musculature around the denture periphery affect denture retention. It is advised to check the tray for overextensions and then mould the impression material to provide adequate relief in these areas at the impression stage. A common mistake is to let the technician decide on the extension, resulting in random trimming. An often-neglected area is where the masseter and buccinator muscles influence the disto-buccal border of the lower denture (Figure 4).
Figure 4. Denture extension and posterior arch form.
Error 4: Poor distal extension of the dentures
A common error diagnosed on the New Patient Clinics was upper dentures constructed short of the maxillary tuberosity/vibrating line and, for the lower dentures, the under extensions towards the retromolar pad. It is appreciated that, for certain patients, the denture design needs to deviate from the norm (severe gagging patients or large maxillary tori). However, these patients only account for low numbers.
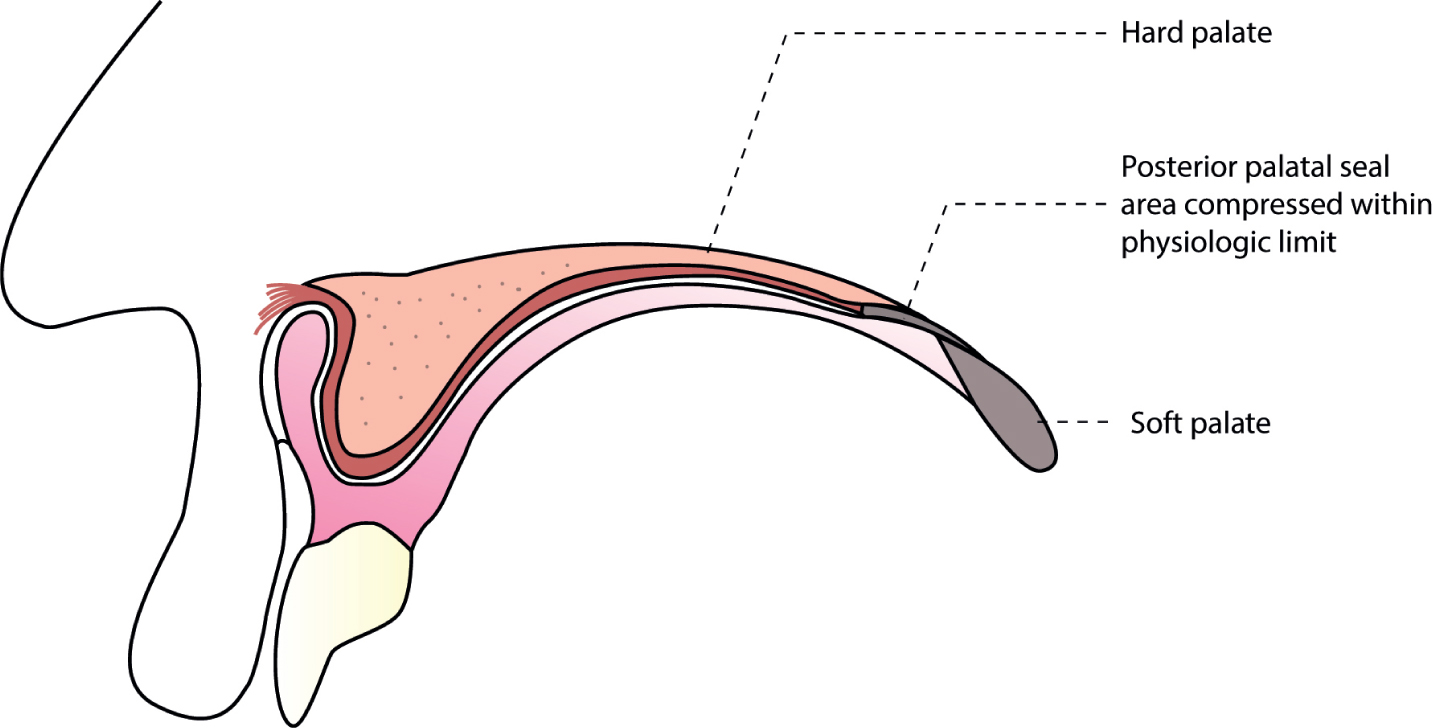
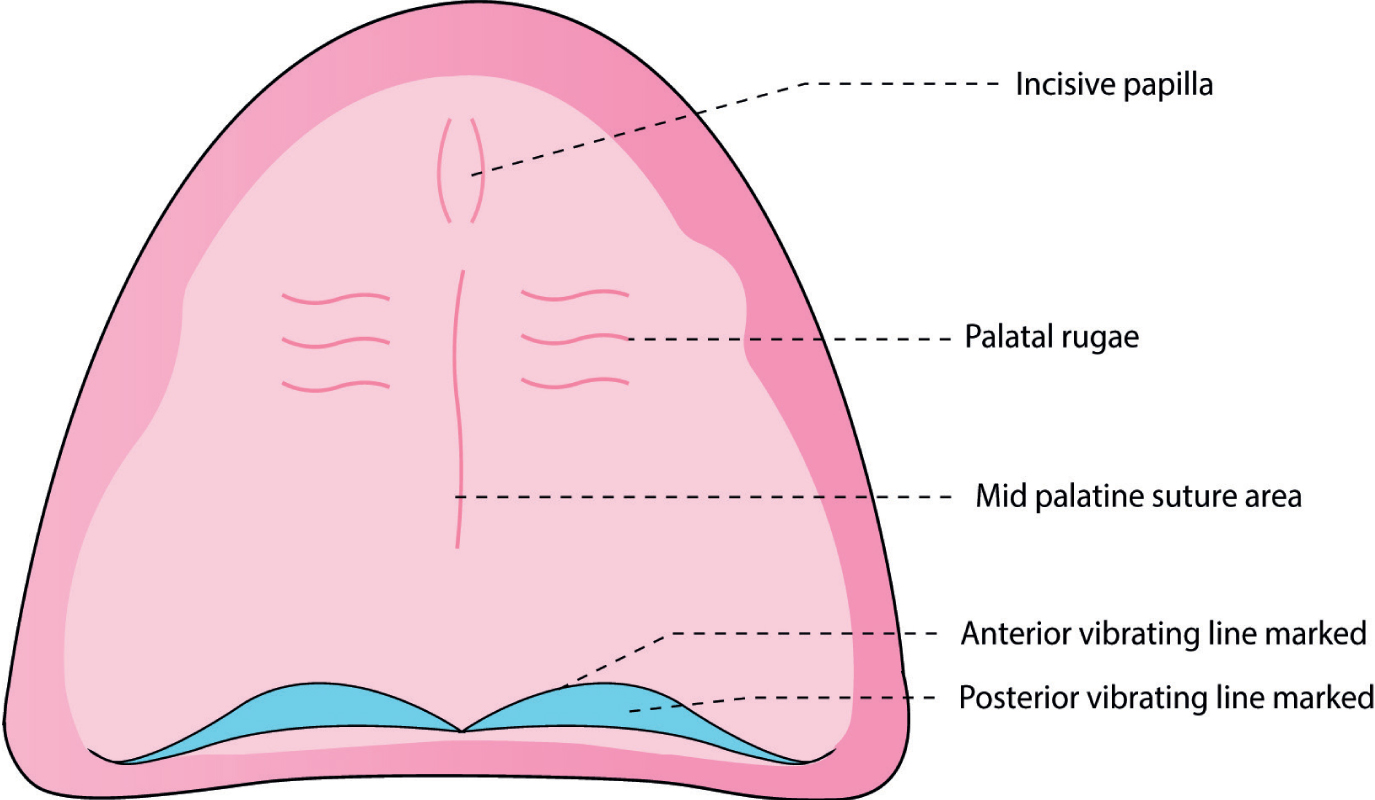
The posterior limit of the upper denture is guided by the palatal seal area. This is the area between the anterior and posterior vibrating lines. The anterior vibrating line is the imaginary line between the hard palate and the immovable part of the soft palate. The posterior vibrating line is the imaginary line at the junction of immovable and movable tissues of the soft palate. The palatal seal area can be compressed within the physiologic limit to achieve a peripheral seal (Figure 5). Scribing a cupid bow shape at this area is an acceptable technique, if the dentist is not experienced with functional recording (Figure 6). However, this needs to be done by a dentist who understands the anatomy of the area and not to be left to the technician.
Figure 5. Posterior palatal seal.Figure 6. Palatal seal illustrated on a model.
Similarly, the retromolar pad provides the standard guide for the distal extension of the lower denture. An ideal lower denture extends to cover the retromolar pad. Even a retromolar seal has been recognized by some researchers.6
Clinical Tip 3
The posterior border of the upper denture and the distal extension of the lower denture should be prescribed by the dentist. This can be marked on the impression or recorded by a functional method or scribed on the cast.
Error 5: Inclination of the occlusal plane
The stability of dentures depends partially on how the upper and lower occlusal surfaces contact during function. In the natural dentition, anterior and posterior teeth provide mutual protection. This means that, in centric position, the posterior teeth are in contact, protecting anterior teeth from over contacting, and in eccentric movements the opposite occurs. In complete dentures, this would lead to instability during eccentric movements.
Balanced or non-balanced occlusion and their evidence base is weak, as the mastication of a bolus of food will not necessarily rely on balanced occlusion. Best practice would be to reduce gross interferences in the occlusion and ensure that there are no tipping forces on the occlusion during excursive movements. Strong contacts in the anterior or posterior teeth, such as second molars, should be avoided. Whilst occlusion is important, there are other important factors that will also interact, such as the neuromuscular control of the prosthesis.
From a practical point of view, the ala tragal line will often coincide with the natural occlusal plane and is used as a guide to trim the wax rim of the upper registration block.7, 8
Clinical Tip 4
Record and communicate the inclination of the occlusal plane of the upper denture with jaw relation registration and verify this at the try in and denture insertion stage. This is because this may be missed by the technician or lost during the polymerization procedure as a mishap.
Error 6: Incorrect level of lower occlusal plane
In an effort to save time there are techniques in general practice where the occlusal record is made from a ‘squash bite’ of softened wax. Often the resulting denture succeeds due to the patient's ability to adapt rather than a particular technique. However, it will tend to produce an inaccurate recording due to distortion of the warm wax. A good occlusal record rim will have established the position and height of the rims, including the mandatory markings of the midline, high and low lip lines and canine lines; and then use a bite registration material to record the relations. This method will allow the technician to understand the future teeth size, and their position. Clear communication to the technician to use an appropriate articulator is also advised, as it has been noticed that many technicians attempt not to use an articulator or use a hinge articulator. For complete denture construction, an average value articulator will be sufficient.
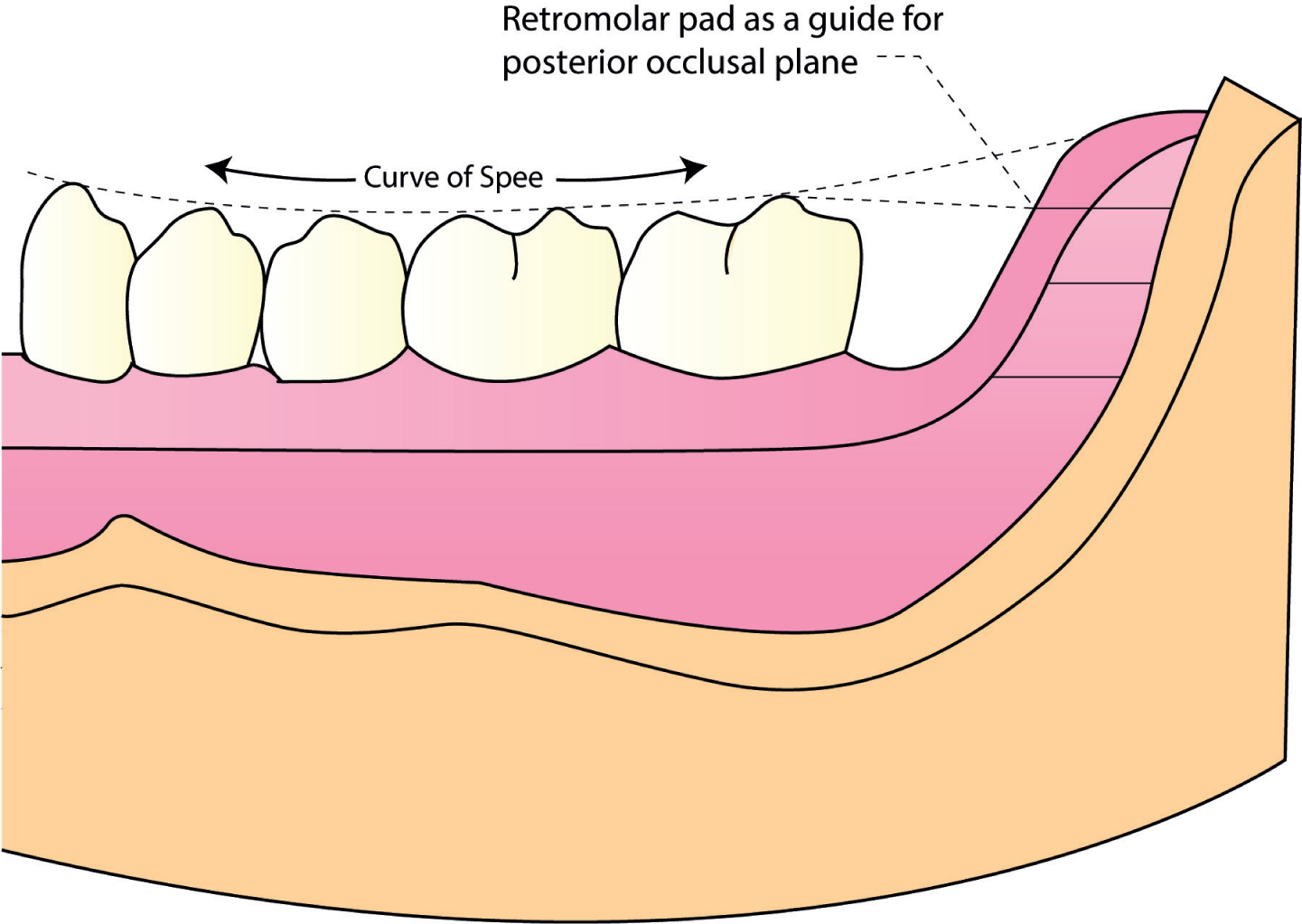
The anterior height of the occlusal plane is decided by the lip position, corner of the mouth and aesthetics. In most situations this never poses a problem as patients also actively take part in deciding the anterior height. However, the posterior height is the problem. Arranging lower posterior teeth above the level of the tongue easily displaces the denture. A practical guide is to take the retromolar pad as a reference point. Maintaining the posterior occlusal height at the junction of the anterior two thirds and posterior third of the retromolar pad has been proved to place the occlusal height in the right position in most patients7, 9 (Figure 7).
Figure 7. Posterior occlusal height.
Error 7: Teeth positioning outside of the neutral zone
The neutral zone is the area where the buccal and labial forces are balanced by the lingual muscle forces. It is important that the teeth are positioned in this neutral zone.10 The neutral zone technique may be reserved for patients with a more complex anatomy and may not be needed for every complete denture situation. However, consideration should be given to lip fullness, the activity of the modiolus, and posterior tongue space (Figure 3).
The modiolus is the area near the corner of the mouth where a group of muscles converge.11 Consideration should be given to the muscle force created in this area.12 If the teeth are placed too buccally forward, contraction of the modiolus will displace the denture. On the other hand, if the teeth are lingually positioned, the tongue space will be restricted, resulting in the lower denture being displaced during function.13, 14
Shaping the occlusion rim based on the muscle forces will provide a guide for the technician to copy similar to the actual teeth position. This can again be verified during try-in stage. A rough guide could be the midline grooves of the posterior teeth falling in line with the ridge crest.
Error 8: Improper vertical dimension
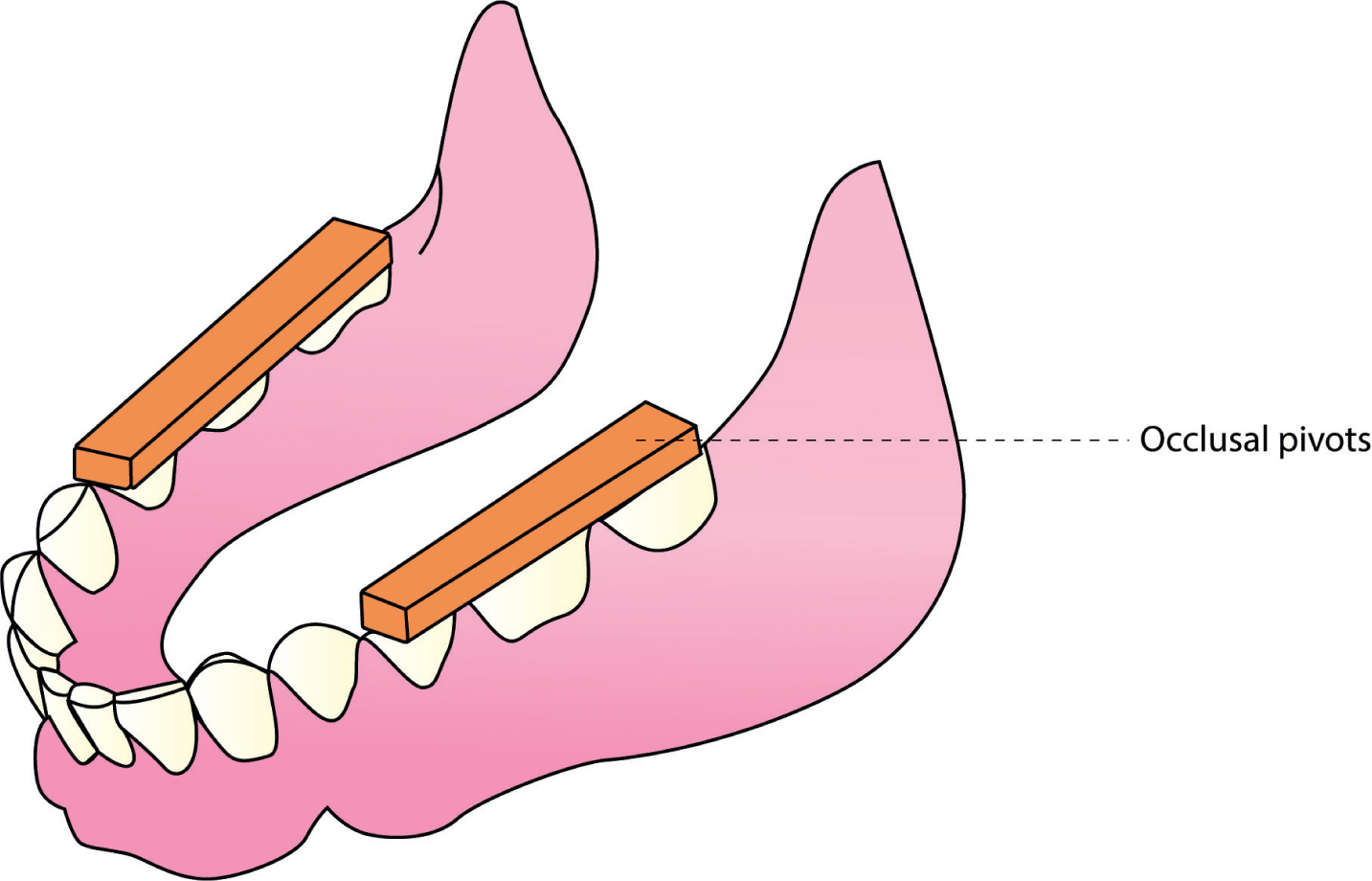
Over time, long-term denture wearers will often adapt and function with worn occlusal surfaces, overclosure and a resulting reduced vertical dimension. Careful discussion about the issues of restoring vertical height will allow the patients to be prepared for these changes (Figure 8). Use of occlusal pivots on the old denture teeth have also been advised to provide an idea of how they will feel at the end and, in turn, will improve the acceptance.
Figure 8. Resin blocks added to the posterior occlusal surfaces of the denture to increase the vertical dimension of occlusion to the biomterically acceptable height and to evaluate the acceptance of the patient.
Free-way space describes the distance between the upper and lower occlusal surfaces when the jaws are at rest position. A minimum of 2 to 4 mm of inter-occlusal clearance in the premolar area is the accepted norm.5 The most common technique taught is the use of the Willis bite gauge. The measurements can also be verified by checking the closest speaking space. Practically, this will involve the patient saying the days of the week and observing the space between the artificial teeth.
Error 9: Jaw relation registration and verification
It is generally accepted that complete dentures should be registered in RCP as it has the advantage of being reproducible.15 Errors in this registration can lead to premature contacts. This in turn will lead to loss of occlusal stability, which was diagnosed for 16 patients (22% of patients).
The occlusion rims should be shaped to establish correct height, anteroposterior position and then to be sealed using a rigid inter-occlusal recording material. This helps the technician to articulate the models and then to follow the shape of the rims to position teeth.
Error 10: Communication
Last, but not least, in our list of errors is issues with communication. Patients turn up on the New Patient Clinics disgruntled about the cost of the dentures, expectations that have not been met, duration of treatment, and other complaints that suggest communication problems. When a GDP understands the background, it is easy to assess the prognosis by identifying the patient expectations, and practical and anatomic difficulties. This then must be communicated to the patient and recorded in the patient records. This will avoid future misunderstandings and help in organizing appropriate referral to secondary care. Whilst it is appreciated that there are difficulties and often the story told by the patient may not reveal all aspects of the events, the treating dentist has an obligation to ensure that his/her note-taking accurately reflects the conversation. In a similar manner, the consulting dentist is not in a position to judge what took place with previous treatment and will diagnose the problem and look to a sensible treatment plan.
Summary
Complete denture construction is often seen as a technically demanding clinical technique. This is partly due to a decreasing edentulous population, with those patients remaining becoming more difficult to treat, often with high expectations of a positive outcome. This will lead to increasing challenges for both undergraduate and postgraduate educators who are involved in the training of clinicians undertaking treatment in this field.
This article provides some possible answers to errors diagnosed on the New Patient Clinics for patients referred for complete dentures. Although not exhaustive, these tips for the GDP may assist in the treatment of patients and help to achieve better outcomes locally.