Wilson NHF, Burke FJT, Brunton PA, Creanor S, Hosey M-T, Manocci F. Dental practice in the UK in 2015/2016 Part 2: Aspects of direct restorations, bleaching, endodontics and paediatric dentistry. Br Dent J. 2019; 226:110-114
Brocklehurst P, Hoare Z. How to design a randomised controlled trial. Br Dent J. 2017; 222:721-725
Burke FJT. End of the road for the randomised controlled trial in restorative dentistry?. Dent Update. 2017; 44:806-808
Alcaraz MGR, Veitz-Keenan A, Sahrmann P, Schmidlin PR, Davis D, Iheozor-Ejifor Z. Direct composite resin fillings versus amalgam fillings for permanent or adult permanent teeth. Cochrane Database Syst Rev. 2014; (3)
Norman RD, Wright JS, Rydberg RD, Felkner LL. A five-year study comparing a posterior composite resin and an amalgam. J Prosthet Dent. 1990; 64:523-529
Letzel H. Survival rates and reasons for failure of posterior composite restorations in a multicentre clinical trial. J Dent. 1989; 17:S10-S17
Cunningham J, Mair LH, Foster MA, Ireland RS. Clinical evaluation of three posterior composite and two amalgam restorative materials. Br Dent J. 1990; 169:319-327
Opdam NJM, Bronkhorst EM, Roeters J, Loomans BAC. A retrospective clinical study on longevity of posterior composite and amalgam restorations. Dent Mater. 2007; 23
Opdam NJM, Bronkhorst EM, Loomans BAC, Huysmans M-C DNJM. 12 year survival of composite vs amalgam restorations. J Dent Res. 2010; 89:1063-1067
Laske M, Opdam NJM, Bronkhorst EM, Braspenning JCC, Huysmans M-C DNJM. Longevity of direct restorations in Dutch dental practices: descriptive study out of a practice-based network. J Dent. 2016; 46:12-17
Naghipur S, Pesun I, Nowalowski A, Kim A. Twelve-year survival of 2-surface composite resin and amalgam premolar restorations placed by dental students. J Prosthet Dent. 2016; 116:336-339
Bernardo M, Luis H, Martin MD, Leroux BG, Rue T, Leitao J, DeRouen TA. Survival and reasons for failure of amalgam versus composite restorations placed in a randomised controlled trial. J Am Dent Assoc. 2007; 138:775-783
Kopperud SE, Tweit AB, Gaarden T, Sandvik L, Espelid I. Longevity of posterior dental restorations and reasons for failure. Eur J Oral Sci. 2012; 120:539-548
Bogacki RE, Hunt RJ, del Aguila M, Smith WR. Survival analysis of posterior restorations using an insurance claims database. Oper Dent. 2002; 27:488-492
Palotie U, Eronen AK, Vehkalahti F, Vehkalahti MM. Longevity of 2- and 3-surface restorations in posterior teeth of 25-to 30-year-olds attending a Public Dental Service a 13-year observation. J Dent. 2017; 62:13-17
van de Sande FH, Rodolpho PA, Basso GR, Patias R, da Rosa QF, Demarco FF, Opdam NJ, Cenci MS. 18-year survival of posterior composite resin restorations with and without glass ionomer cement as base. Dent Mater. 2015; 31:669-675
van de Sande FH, Opdam NJ, Rodolpho PA, Correa MB, Demarco FF, Cenci MS. Patient risk factors' influence on survival of posterior composites. J Dent Res. 2013; 92:(7 Suppl)78S-83S
Lempel E, Toth A, Fabian T, Krajczar K, Szalma J. Retrospective evaluation of posterior direct composite restorations: 10-year findings. Dent Mater. 2015; 31:115-122
Pallesen U, van Dijken JW, Halken J, Hallonsten AL, Hoigaard R. A prospective 8-year follow-up of posterior resin composite restorations in permanent teeth of children and adolescents in Public Dental Health Service: reasons for replacement. Clin Oral Investig. 2014; 18:819-827
Pallesen U, van Dijken JW, Halken J, Hallonsten AL, Hoigaard R. Longevity of posterior resin composite restorations in permanent teeth in Public Dental Health Service: a prospective 8 years follow up. J Dent. 2013; 41:297-306
Baldissera RA, Correa MB, Schuch HS, Collares K, Nascimento GG, Jardim PS, Moraes RR, Opdam NJ, Demarco FF. Are there universal restorative composites for anterior and posterior teeth?. J Dent. 2013; 41:1027-1035
Da Rosa Rodolpho PA, Donassollo TA, Cenci MS, Loguercio AD, Moraes RR, Bronkhorst EM, Opdam NJ, Demarco FF. 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater. 2011; 27:955-963
da Rosa Rodolpho PA, Cenci MS, Donassollo TA, Loguercio AD, Demarco FF. A clinical evaluation of posterior composite restorations: 17-year findings. J Dent. 2006; 34:427-435
Opdam NJ, Bronkhorst EM, Roeters JM, Loomans BA. Longevity and reasons for failure of sandwich and total-etch posterior composite resin restorations. J Adhes Dent. 2007; 9:469-475
Opdam N, van de Sande F, Bronkhorst E, Cenci M, Bottenberg P, Pallesen U Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res. 2014; 93:943-949
Demarco FF, Correa MB, Cenci MS, Moraes RR, Opdam NJ. Longevity of posterior composite restorations: not only a matter of materials. Dent Mater. 2012; 28:87-101
Astvaldsdottir A, Daerhamn J, van Dijken JWV, Naimi-Akbar A, Sandborgh-Englund G, Tranieus S, Nilsson M. Longevity of posterior resin composite restorations in adults a systematic review. J Dent. 2015; 43:934-954
Beck F, Lettner S, Graf A, Bitriol B, Dumitrescu N, Bauer P, Moritz A, Schedle A. Survival of direct resin restorations in posterior teeth within a 19-year period (1996–2015): A meta-analysis of prospective studies. Dent Mater. 2015; 31:958-985
Moraschini V, Fai CK, Alto RM, dos Santos GO. Amalgam and resin composite longevity of posterior restorations: a systematic review and meta-analysis. J Dent. 2015; 43:1043-1050
da Viega AMA, Cunha AC, Ferriera DMTP, da Silva Fidalgo TK, Chianca TK, Reis KR, Maia LC. Longevity of direct and indirect resin composite restorations in permanent posterior teeth: a systematic review and meta-analysis. J Dent. 2016; 54:1-12
Alvanforoush N, Palamara J, Wong RH, Burrow MF. Comparison between published clinical success of direct resin composite restorations in vital posterior teeth in 1995–2005 and 2006–2016 periods. Aust Dent J. 2017; 62:132-145
Burke FJT, Lucarotti PSK. The ultimate guide to restoration longevity in England and Wales. Part 10: Key findings from a 10 million restoration dataset. Br Dent J. 2018; 225:1011-1018
Nordbo H, Leirskar J, von der Fehr FR. Saucer-shaped cavity preparations for posterior approximal resin composite restorations: observations up to 10 years. Quintessence Int. 1998; 29
Tobi H, Kreulen CM, Vondeling H, van Amerongen WE. Cost-effectiveness of composite resins and amalgam in the replacement of amalgam Class II restorations. Community Dent Oral Epidemiol. 1999; 27:137-143
Periera CT, Albuquerque E, Barbosa S, Lopes L, Calazas F, Manns S Clinical time and post-operative sensitivity using bulk fill composites with Universal adhesives. J Dent Res. 2018; 97:(Spec Iss B)
Hickel R, Roulet JF, Bayne S, Heintze SD, Mjör IA, Peters M Recommendations for conducting controlled clinical studies of dental restorative materials. Update and clinical examples. Clin Oral Investig. 2010; 14:349-366
Survival rates of resin composite restorations in loadbearing situations in posterior teeth F J Trevor Burke Louis Mackenzie Adrian CC Shortall Dental Update 2024 46:6, 707-709.
The use of resin composite for routine restoration of cavities in posterior teeth is now commonplace, and will increase further following the Minamata Agreement and patient requests for tooth-coloured restorations in their posterior teeth. It is therefore relevant to evaluate the published survival rates of such restorations. A Medline search identified 144 possible studies, this being reduced to 24 when inclusion criteria were introduced. Of these, ten directly compared amalgam and composite, eight were cohort studies, and six were systematic reviews. It was concluded that posterior composites may provide restorations of satisfactory longevity and with survival rates generally similar to those published on amalgam restorations. However, the ability of the operator in placing the restoration may have a profound effect.
CPD/Clinical Relevance: With the increasing use of composite for restorations in posterior teeth, it is relevant to note that these may provide good rates for survival.
Article
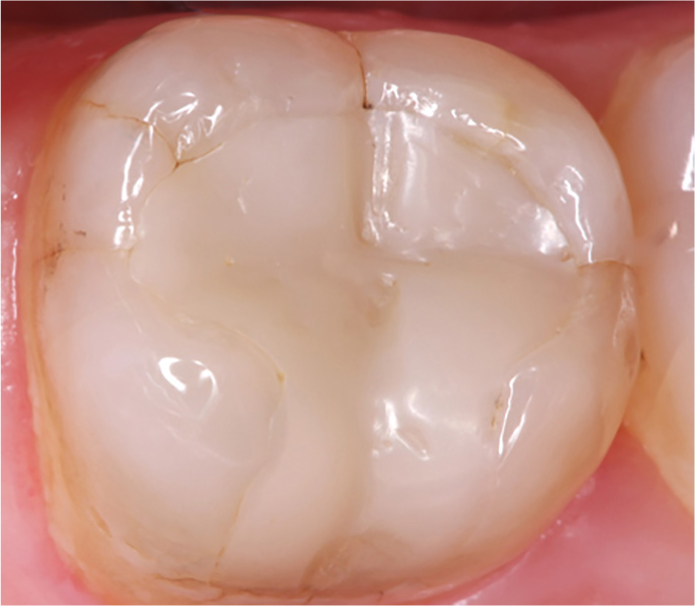
Resin composite has been an alternative material to dental amalgam since the first dedicated ‘posterior composite’ material Occlusin™ (ICI Dental, Macclesfield, UK) was introduced in 1985. More recently, resin composite has become a central component of direct restorative dentistry, as a result of increasing popularity among patients because of the good aesthetics of resin composite restorations (Figure 1),1 and given patient concerns relating to the use of a mercury-containing product.2 The increasing use of resin composite materials in posterior teeth (hitherto termed ‘posterior composites’) has been given added impetus, after July 2017, when the use of amalgam was banned for use in primary teeth and for children under the age of 15 years of age and in pregnant and lactating women.3 In addition, results of questionnaire-based research in the UK in 2015 has indicated that respondents placed almost as many ‘posterior composites’ in molar teeth in Class II cavities as amalgams for the first time (48% composite vs 52% amalgam).4 For these reasons, it is therefore considered relevant to review the survival rates of resin composite restorations placed in posterior teeth in loadbearing situations.
Figure 1. Posterior composite restoration demonstrating good aesthetics after 15 years.
Investigating success rates of restorations
Randomized Clinical Controlled Trials (RCCTs) have been considered to be the ‘gold standard’ for assessment of the clinical performance of restorations by Brocklehurst and Hoare,5 these workers adding that ‘there are significant challenges when designing such complex studies’, and ‘there is an increasing need for high-quality evidence from primary dental care’. It has also been noted that RCCTs are few in restorative dentistry.6 In addition, the Cochrane review has been considered the ‘gold standard’ for systematic reviews, but these suffer from the small number of RCCTs in restorative dentistry. For example, in the most recent Cochrane study on posterior composites, published in 2014,7 the reviewers located seven RCCTs, but five were published in or before 1990 and the other two, while they were well designed RCCTs, were studies of amalgam vs composite in posterior teeth in 921 children under the age of 12 years. It may therefore be considered that these are not typical of the clinical situations where the majority of dental restorations for adult patients, worldwide, are placed, namely, general dental practice. The authors concluded that amalgam fillings had lower failure rates than composite fillings, but Burke6 considered that that conclusion cannot be justified because the research was on restorations in children and that the other papers were from a previous ‘generation’ of dental materials (bonding agents and resin composite). The authors add, rather strangely dismissing their findings, that ‘some materials may no longer be in use or have been replaced by products with better physical properties’.
It was therefore suggested that future Cochrane reviews and, indeed, all future systematic reviews on restoration survival in restorative dentistry, should include well-designed cohort studies which evaluate large numbers of restorations, and/or long duration, simply because there are more of these than well-designed RCCTs.6
This narrative review will therefore seek to identify broadly-based studies in which amalgam and resin composite restorations for adult patients are compared over a minimum period of five years and will also include cohort studies for adult patients, where possible from general dental practice, in which more than 250 restorations are followed for a minimum period of five years (Table 1). It should be added that success with ‘posterior composites’ is dependent also upon the operator's knowledge of, and familiarity with, the various technique sensitivities which have been described by Mackenzie and colleagues.8
Studies comparing amalgam and resin composite restorations placed for adult patients in loadbearing situations in posterior teeth, for a minimum of 5 years
Cohort studies evaluating >250 resin composite restorations placed for patients over the age of 13 years in loadbearing situations in posterior teeth for a minimum of 5 years
Retrospective and prospective studies included
Systematic reviews included
Methods
An OVID Medline and Epub Ahead of Print Search was carried out with the title ‘Survival of composite restorations in posterior teeth’ – English language articles 1990–2018. In addition, the references from selected papers were searched in order to ensure as complete a coverage of the subject as possible.
Studies including amalgam and composite restorations
An early RCCT in restorative dentistry is that comparing the first dedicated posterior composite restorative, Occlusin™ (developed by ICI when they had a Dental Division) vs amalgam9, 10 but, by the time they reported the findings at five years, the composite material had changed, so this work may be regarded as a pointer to the amalgam vs composite debate, rather than strong evidence.
At the time when tooth-coloured materials had become available for placing in posterior teeth, a large three-year study in Liverpool was published in 1990.11 This was funded by the Department of Health in the UK, perhaps so that they could establish the acceptability (or otherwise) of such products, by way of an RCCT of two amalgams and three composites, with 605 restorations placed at baseline. The results indicated that two composite materials performed better than the third and there were more mechanical failures in the amalgam group, while failures in the composite group were more likely to be biological in nature. Despite the overall results being relatively positive,11 with no significant difference in the number of failures in the amalgam group and the composite group, the Department of Health did not agree to permit placement of composite restorations in posterior teeth.
Opdam and colleagues, in a practice-based study, first evaluated the 10-year survival of composite vs amalgam restorations,12 following this with the 12-year evaluation.13On a dataset of 912 amalgam restorations and 1,955 composite restorations, at the 10-year evaluation, composites and amalgam restorations performed similarly, with the survival of amalgam restorations being 79.2% at 10 years (ie an AFR of 2.1%) and composite 82.2% (ie an AFR of 1.8%), not statistically different: however, at the 12-year evaluation, the composite restorations were performing two percentage points better in low caries risk patients.13
Laske and colleagues,14 using a large retrospective database established in The Netherlands (358,548 restorations in 75,556 patients, with restorations being placed by 67 general dental practitioners (GDPs)), found that the AFR of composites was 4.4%, amalgam 5.1%, and glass ionomer (GI) 11.1%. These workers also established a large discrepancy in the performance of different GDPs, with the AFR varying between 2.3% and 7.9%, the mean being 4.6% at 10 years. Composite showed higher survival rates than amalgam, while the age of the patient, gender, number of surfaces, operator, tooth type and endodontically treated teeth, significantly influenced survival for both materials.
The performance of two-surface resin composite and amalgam restorations placed in premolars by dental students in Manitoba, Canada, was assessed at 12 years.15Initially, 1,695 composite and 1,125 amalgam restorations were placed: at 12 years, the survival probability of composite restorations was 86% and that of amalgam restorations was 91.5%, this difference being statistically significant. The authors concluded that both composite resin and amalgam restorations had acceptable success rates and similar failure modes, with recurrent caries being the most common reason for failure.
Bernardo and co-workers,16 in a randomized controlled trial, assessed a total of 1,748 amalgam and composite restorations placed at baseline: these were followed for seven years. The results indicated that the survival rate of the amalgam restorations was 94.4%, that of the composite restorations being 85.5%. Secondary caries was the main reason for failure in both materials, but was 3.5 times greater in the composite group: the authors concluded that the amalgam restorations ‘did better’ than composite restorations, with this difference being accentuated in large restorations with more than three surfaces involved.
Kopperud and co-workers17 carried out an extensive study in Norway, with a total of 4,030 Class II restorations being assessed at an average follow-up time of 4.6 years. The median age of the patients was 15 years: 81.5% of the restorations were composites, 4.6% amalgam, 12.7% compomer and 1.2% glass ionomer. Overall, 61.6% of restorations were successful, with a mean AFR of 2.9% for resin composite and 1.6% for amalgam. Saucer-shaped cavity preparations appeared to predispose to reduced survival of the resin composite restorations.
Bogacki et al18 analysed a large US-based insurance database, with a total of 207,558 amalgam and 93,195 composite restorations in two-surface cavities in posterior teeth followed for between 36 and 44 months. The results indicated that the probability of survival was slightly higher for amalgam. The authors concluded that ‘composite fared almost as well as amalgam’ and that dentists should advise their patients that ‘composite might not last as long as amalgam in a posterior tooth, but is a good alternative to amalgam’.
Most recently, Palotie et al19have analysed a large practice-based dataset in Finland, which included a total of 5,542 two- and three-surface composite and amalgam restorations. These were followed ‘indirectly’ from 2002 until 2015, with the results indicating that median survival time of two-surface composites was greater than three-surface restorations, and restorations in premolars performed better than those in molars. The authors concluded that long term posterior composite and amalgam multi-surface restorations perform ‘quite similarly’ in molars, but that the three-surface restoration was ‘a challenge for both materials’.
It is not possible to compare the results of the above studies directly due to their heterogeneity, but the conclusion which may be gleaned is that resin composite restorations have survival rates similar to amalgam when placed in loadbearing situations in posterior teeth, with composite being superior to amalgam in two studies, worse in two and with four of the papers which directly compared resin composite with amalgam being equivocal in their findings. There is obviously a need for a RCCT examining survival of amalgam and resin composite but the authors are dubious that this will ever happen.
Composite-only studies
The following studies have been identified:
Van de Sande and colleagues20 investigated a dataset of one dental practice and used it to retrieve data retrospectively. The presence or absence of an intermediate layer of glass-ionomer cement (GIC) was the main factor under analysis, considering survival, annual failure rate and types of failure as outcomes. Other investigated factors were: patient gender, jaw, tooth, number of restored surfaces and composite. A total of 632 restorations in 97 patients were investigated. AFRs up to 18 years were 1.9% and 2.1% for restorations with and without a GIC base, respectively. In restorations with GIC base, fracture was the predominant reason for failure, corresponding to 57.8% of total failures. The authors concluded that the presence of a glass-ionomer cement base did not affect the survival of resin-composite restorations in the investigated sample and that acceptable annual failure rates after 18 years can be achieved with both techniques. In a related study,21 in which risk factors associated with failure were evaluated when they assessed 306 posterior composite restorations in 44 patients after 10 to 18 years, caries risk was assessed and signs of parafunction recorded. In total, 30% of the restorations failed, of which 82% were found in patients with one or two risk factors. Secondary caries was the main reason for failure within high caries-risk patients, whereas fracture was the main reason in ‘occlusal-stress-risk’ patients. Tooth type, arch and pulpal status significantly affected restoration survival. It could therefore be considered appropriate to appraise patients of these risk factors when discussing their treatment.
Lempel and co-workers,22 in a 10-year retrospective study, investigated the longevity of Class II restorations using four similar microhybrid resin composites. Data were collected from patient records. Those patients who received a posterior restoration between 2001 and 2003, and who still visited the clinical practice for regular assessment visits, were included. A total of 225 adult patients (86 males, 139 females) with 701 restorations were evaluated by two operators using the well-recognized criteria. A failure rate of 2.1% was detected. The mode of failures included restoration fracture, secondary caries and endodontic treatment. There was a higher probability of failure in three-surface than in two-surface restorations, this rate being similar when molars and premolars were compared. The most frequent, but clinically acceptable deficiency, was marginal discoloration. The authors concluded that all materials showed acceptable clinical durability in Class II restorations during the 10-year follow-up period, with an overall survival rate of 97.8%, although two materials performed better than the others. AFR was 0.2%.
Pallesen and colleagues23 investigated reasons for replacement and repair of posterior composite restorations placed in permanent teeth of adolescents attending Public Dental Health Service in Denmark. All posterior composite restorations placed consecutively by 115 dentists over a period of 4 years were evaluated at baseline and at 8 years. The endpoint of each restoration was defined when repair or replacement was performed. A total of 4,355 restorations were included. Replacements comprised 406 restorations and repairs 125 restorations. The cumulative survival rate at 8 years was 84%. Failed restorations were most frequently seen due to secondary caries (57%), post-operative sensitivity (10%) and fracture (6%). It is interesting to note that older dentists showed a lower proportion of replaced restorations due to secondary caries than younger dentists. The authors concluded that posterior composite restorations in adolescents performed in general practice showed a good durability with AFR of 2%. More teeth with post-operative sensitivity and a shorter longevity of restorations were observed when a base material was used. An earlier study24 from the same group produced a similar failure rate.
Baldissera and co-workers25 evaluated, in a retrospective longitudinal clinical study, the longevity up to 20 years of posterior restorations placed using three ‘universal’ composites and of anterior restorations placed with two ‘universal’ composites placed in 90 patients in a private practice in Brazil. The results indicated that, in the first 10 years, almost 95% of the restorations were satisfactory, showing increased failure rate thereafter. AFRs varied between 0.3% and 2.5%, with slightly better performance for anterior restorations. Fracture (posterior) and aesthetics (anterior) were the main reasons for failure. The authors concluded that their study provided evidence that anterior and posterior restorations placed with ‘universal’ composites may have excellent long-term clinical performance.
In an interesting practice-based study from Brazil,26 patient records from one practice were analysed. Continually attending patients with at least two posterior composite restorations placed between 1986 and 1990, and still attending the practice (after 22 years) for regular assessment appointments, were invited to attend for an evaluation of their restorations using scientific criteria. A total of 362 restorations (121 Class I, 241 Class II) placed using a closed sandwich technique were evaluated by 2 operators, with 110 failures being detected. Two different composites with regard to filler characteristics and material properties were used: ‘midfilled’ and ‘minifilled’. Similar survival rates for both composites were observed during the full period of observation and there was higher probability of failure in molars and for multi-surface restorations. The authors concluded that both evaluated composites showed good clinical performance over 22 years with 1.5% (midfilled) and 2.2% (minifilled) annual failure rate. This study is a continuation of a similar evaluation at 17 years in which there were 98 failures among the 282 restorations assessed.27 They concluded that the performance of the material was acceptable after that time and that the probability of failure was higher in molar teeth, Class II and larger restorations.
Opdam and co-workers28 investigated the longevity and reasons for failure of Class II posterior composite restorations (PCRs) placed with or without a lining of glass-ionomer cement. A total of 458 Class II PCRs placed in 248 patients by two dentists in a general practice between 1988 and 1997 were retrospectively examined via the patient files. The restorations were placed either with a total-etch technique or with a RMGI lining placed on the dentine. A restoration was clinically acceptable when ‘still in function and acceptable’ at the last check-up visit. Caries risk for each patient was estimated by the treating clinician. A total of 376 total-etch posterior composites and 82 posterior composites with a lining were investigated. After 9 years, survival percentages of 88.1% for total-etch restorations (AFR 1.3%) and 70.5% (AFR 4%) for restorations with an RMGI lining were found. Predominantly, failures started occurring after 3 to 4 years of clinical service. Results indicated that the presence of a lining and high risk for caries significantly increased the failure rate of the restorations. On the other hand, van de Sande and colleagues20 have reported that the presence of a glass-ionomer cement base did not affect the survival of resin-composite restorations in the investigated sample. They concluded that acceptable AFRs after 18 years can be achieved with both techniques, leading to the perspective that an intermediate layer, placed during an interim treatment, may be maintained without clinical detriment, but no improvement in survival should be expected based on such measures.
Opdam et al29 investigated the survival, over a five-year period, of posterior resin composite restorations placed by students at the University of Nijmegen, The Netherlands. Class I and II resin composite restorations placed by second to fourth year dental students were evaluated. Patients attended the dental school every 6 months for a check-up during which all restorations were checked on their clinical acceptability. In case of replacement or repair of a restoration, this was registered in the patient's record. From each record, the survival time and reasons for failure of resin composite restorations were gathered. A total of 703 posterior composite restorations in 382 patients were evaluated. At 5 years, 560 of the 703 restorations were still considered to be ‘clinically acceptable’. A total of 49 restorations were considered as ‘functionally present’, of which 44 were restored with a crown and four had received a new restoration adjacent to the existing restoration without its removal, while 94 restorations had failed. The survival rate of the restorations was 87% at 5 years, resulting in an AFR of 2.8%. The authors concluded that dental students are able to place resin composite restorations in posterior teeth with an acceptable mean annual failure rate.
Results
A total of 144 studies fulfilled the initial search criteria. However, when the results were re-assessed with regard to the inclusion criteria, studies relating to primary teeth, ART, CAD-CAM, composite inlays/onlays, fibre-reinforced composite, resin-modified glass ionomer (RMGI), composite crowns, sealant restorations, preventive resin restorations, and core build-ups were excluded. The number of studies finally included was 24.
Where the data permit, the authors will calculate the Annual Failure Rate (AFR), as a readily understandable and comparable means of determining survival of restorations, this being the overall failure rate over the time of the particular study divided by the number of years for which the restorations were assessed.
The conclusion gleaned from the above cohort studies is that resin composite restorations have acceptable survival rates when placed in loadbearing situations in posterior teeth, with AFRs generally within the range 2% to 3%, which the authors consider to be compatible with successful clinical practice. However, the relevance of the presence of a glass-ionomer base is not clear as it does not appear to increase the AFR in all the identified studies. This may be a matter for individual clinicians to consider, based upon the risk factors of their patients.
Systematic reviews
Opdam and colleagues30 published a systematic review of the posterior composite literature in 2014. They included 1,551 papers, of which 25 met their inclusion criteria and with 12 authors agreeing to provide raw data. Their data indicated that, of a total of 2,816 restorations included, 569 had failed. A liner or base in glass ionomer had a negative effect on survival and the AFR was 2.4% at 10 years. Interestingly, these workers found that the reasons for failure of restorations at year 1 was very different from year 6, with need for endodontic treatment being most prevalent at year 1 and caries the highest reason for failure at year 6, indicating the need for studies of long duration.
Demarco and colleagues31 searched the dental literature looking for clinical trials investigating posterior composite restorations over periods of at least 5 years published between 1996 and 2011. The search resulted in 34 selected studies, with 90% of the clinical studies indicating that annual failure rates between 1% and 3% can be achieved with Class I and II posterior composite restorations, depending on several factors, such as tooth type and location, operator, socioeconomic and demographic elements. The main reasons for failure in the long term were secondary caries, related to the individual caries risk, and fracture, related to the presence of a lining or the strength of the material used, as well as patient factors such as bruxism. Repair was considered a viable alternative to replacement, and it can increase significantly the functional longevity of restorations. The results therefore indicated that a long survival rate for posterior composite restorations can be expected provided that patient, operator and materials factors are optimized when the restorations are performed.
Astvaldsdottir et al,32 in their systematic review, set narrow inclusion factors, namely prospective clinical trials, minimum four years' duration and 40 restorations per experimental group. They read 93 articles in full, of which 18 met inclusion criteria but 10 were excluded because of risk of bias, therefore 8 were included. Of these, survival rate at 4 years was 93% and 91% at 5 years, 88% at 9 years, ie AFR was 1.3%. The most common reason for failure was secondary caries (n = 31), tooth fracture (n = 15) and the authors concluded ‘that the overall survival proportions of posterior resin composite restorations is high’.
Beck and colleagues,33 in an extensive study, identified 88 prospective studies (published between 1996 and 2015) for analysis, with observation times of 1–17 years, but with most studies ranging from 1–4 years, and 11 lasting 10 years or more. The mean AFR was 1.5% for short-term studies, rising to 2.0% for long-term studies. The researchers found no significant difference relating to whether rubber dam was used/not used, the bonding agent ‘generation’ or composite material used: operator was a statistically significant variable, as also was patients' oral hygiene. Interestingly, these workers found that the failure rate decreased when the study recall rate increased, explaining this by the assumption that a study population which is more compliant and attends for recall regularly may also be motivated to maintain good oral hygiene and have lower caries risk.
Moraschini and co-workers34 carried out a systematic review/meta-analysis, including RCCTs, controlled clinical trials and prospective/retrospective cohort studies in their work. Eligibility criteria for inclusion were clinical trials of minimum 12 months' duration, comparing failure rates of Class I and II amalgam and composite restorations. Of 938 titles, 21 studies were included for careful reading, after which a further 13 studies were excluded, leaving eight. The authors concluded that the results ‘suggest that posterior composite resin restorations still have less longevity and a greater incidence of secondary caries than amalgam restorations', but noting no difference in fracture of restorations in the two materials. They add that ‘the data in this review should be interpreted with caution due to the inclusion of only two RCCTs. The present authors note that four of the included papers were published more than 20 years ago (ie unlikely to be representative of current materials), and one, published in 2007, was a cross-sectional radiographic survey.
Da Viega and co-workers35 conducted a systematic review/meta-analysis, including RCCTS comparing the clinical performance of direct and indirect resin composite restorations in Class I and II cavities with a minimum of two years' follow up. They initially included 912 articles, but eventually included nine. The authors concluded that there was no difference in clinical longevity of direct and indirect resin composite restorations, adding that ‘it seems more reasonable to suggest that direct restorations should be given preference to indirect, since the former require less effort and cost’.
The conclusion gleaned from the above systematic reviews is that resin composite restorations have acceptable survival rates when placed in loadbearing situations in posterior teeth, with AFRs generally within the range 2% to 3%. Risk factors for premature failure include patients at high risk of caries and the presence of a liner or base beneath the resin composite restoration.
Discussion
This narrative review has sought to identify publications which can provide meaningful information about the survival of posterior composites, as these restorations are being increasingly placed, worldwide. A high proportion of the included cohort studies on posterior composite have involved restorations placed in general dental practice, with the authors considering that this may enhance the relevance of the findings. In addition, three of the papers which directly compared amalgam with composite were also set in the general dental practice arena. While the inclusion criteria stated ‘adult patients’, two studies have been included22, 23 in which the posterior composite restorations were placed in adolescents. The authors consider that these are relevant, firstly because of the large numbers of restorations assessed at over five years in a primary care environment, but also because it may be considered that, if restorations can survive in this potentially challenging group of patients (for factors such as high caries diet and challenging patient co-operation), then they should perform at least as well in older patients.
It may therefore be concluded that posterior composite restorations may provide restorations of satisfactory survival, with two papers17, 34 of those identified in which amalgam and composite are directly compared, having posterior composite restorations which performed less well than amalgam. However, the authors consider that the number of amalgam restorations in one study17was so small as to preclude meaningful analysis while, in the other,34the authors advised that the results should be interpreted with caution.
The papers which were selected were considered to be those which had relevance to clinical practice but which presented large numbers of restorations, assessed over periods of more than five years. In this regard, survival of restorations at one year only produce ‘evidence’ relating to the catastrophic failure of restorations, and the systematic review by Opdam et al has demonstrated that long-term data are essential.30
Annual failure rates of posterior composite restorations may be considered to provide restorations of satisfactory longevity. Risk factors, such as high caries susceptibility, large restorations (particularly in molars) have been particularly identified. In the present study, posterior composite restorations were found to have an AFR of between 1.3% and 3.0%, which the authors consider to be compatible with successful clinical practice. However, it is interesting to note that Alvanforoush and colleagues36 did not identify any improvement in performance of posterior composite restorations during the two time periods, 1995–2005 and 2006–2016, despite what many clinicians, anecdotally, might have considered improvements in the materials that they use. The overall rates of failure showed little difference, but the causes showed a notable change. This is believed to be a reflection of increased use of composites for larger restorations and possibly changes of material characteristics. This has also been observed in analysis of a 10 million dataset of restorations placed in England and Wales, with no improvement noted in any form of restoration between 1990 and 2006.37
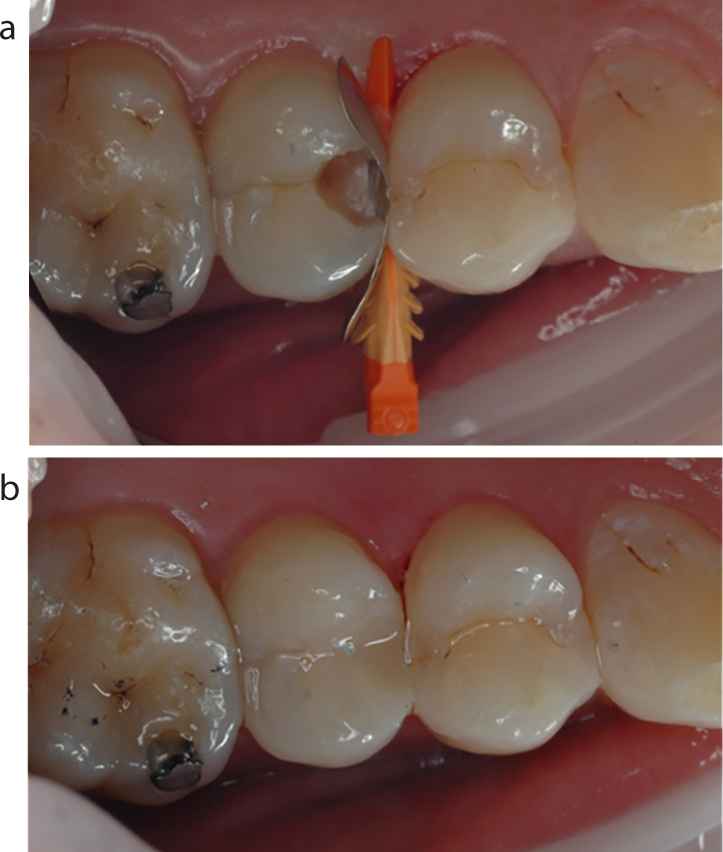
It may be considered that a majority of the restorations placed in the included studies used traditional cavities which included an occlusal lock/key, rather than the mini-saucer shaped cavities (Figure 2), which may be considered appropriate when using adhesive techniques. There is, however, a paucity of work on such cavities although, in the paper by Pallesen and colleagues,23 they state that the cavity design utilized was that which allowed minimal removal of tooth substance, as was appropriate to the ingress of caries. Those workers reported an overall AFR of 2.0%, so it may be considered that such cavity designs are appropriate. On the other hand, Kopperud and co-workers17 considered that ‘saucer-shaped cavity preparations appeared to predispose to reduced survival of the resin composite restorations’. However, the early work of Nordbo et al,38 who followed saucer-shaped cavities restored with resin composite, concluded that ‘the saucer-shaped resin composite restoration represents a viable treatment modality for small cavities, and that the time may have come to include it in dental curricula as a routine operative treatment for small Class II lesions’, a positive endorsement. Further research is therefore indicated on these minimal cavity designs and, in particular, their effect on the fracture resistance of teeth, especially premolars when compared with traditional cavity designs.
Figure 2.
(a) A mini saucer-shaped cavity design which is appropriate to adhesive restorative technology. (b) Cavity in (a) restored using Filtek Bulk Fill Restorative (3M).
However, despite their successful survival data, as identified in this review, posterior composites may not be cost-effective, because they take longer to place.1 In this regard, Tobi and colleagues39 assessed this, as part of a larger randomized clinical trial, looking at effectiveness and treatment costs for 73 composite and amalgam Class II posterior restorations. The results indicated that replacing an amalgam Class II restoration with another amalgam is associated with lower costs than replacing with a composite resin. However, the difference in cost-effectiveness between posterior composites and amalgam restorations may be minimized when using new bulk fill restorative materials which may be placed in increments of up to 5 mm, by recently-introduced adhesives which are quick to place and by increasing experience and skill of practitioners using these materials. In this regard, results from a recent research abstract40 from the London meeting of the International Association for Dental Research have indicated that bulk fill composites may indeed be placed faster than conventional composites in posterior teeth.
While it has been considered that the RCCT is the ‘gold standard’ for comparing two different interventions, these are few, hence the dependence upon cohort studies and systematic reviews in this review. A group of renowned experts in restorative dentistry, co-ordinated by Reinhart Hickel, have published recommendations for the conduct of controlled clinical studies of restorative dental materials.41 They stated that ‘there are many publications on clinical studies but, in most cases, it is impossible to analyse and compare results. This is largely due to inadequate design, insufficient reporting on restoration placements, inadmissible pooling of different groups'. While all of this is true, this study has attempted to calculate AFRs as a readily understandable means of understanding whether restorations are successful or not.
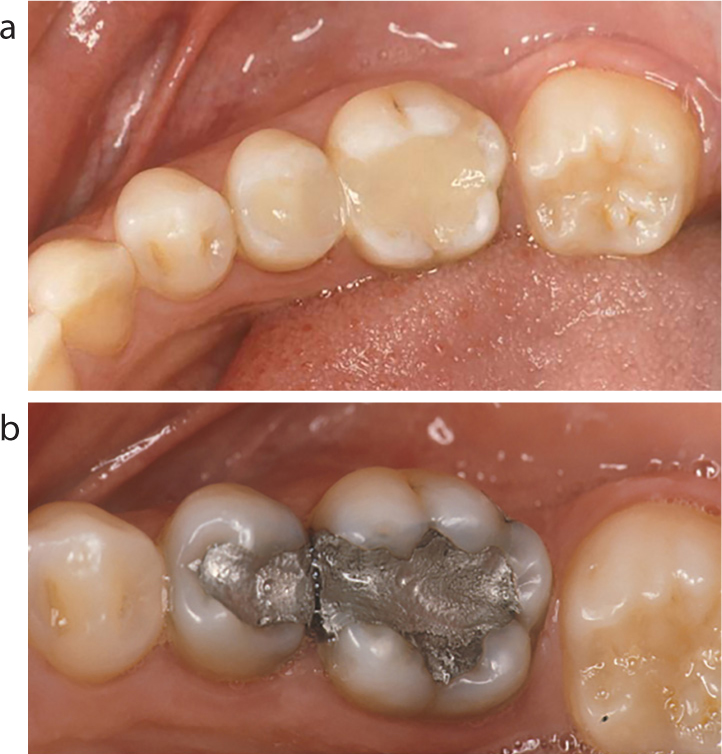
Clinicians reading the present work will all have an aspiration as to the longevity of restorations that they place on a daily basis, so will be able to understand whether AFRs published in the literature are satisfactory or not. In this regard, while it is essential that clinicians have knowledge of the research publications relating to the treatment which they are carrying out, data from the clinician's own clinical practice may be considered valuable when communicating with patients, who may better understand survival rates quoted by their dentist from his/her own practice as opposed to the research literature. In the first author's practice, he followed up many of the restorations which he had placed at periods of up to 10 years (examples being presented in Figures 3, 4 and 5), building up an objective assessment of how well (or not) his restorations were performing. However, it is suggested that this is not good enough today, and that clinicians should be encouraged to adapt the computer system in their practice to record survival data, this surely being the ultimate in meaningful data when discussing possible treatments with their patients.
Figure 3.
(a) Class II restorations in a hybrid composite, at 3 years. (b) The restorations in (a) replaced defective amalgam restorations which were causing interproximal food stagnation.Figure 4. Occlusin™ (ICI) restorations at 10 years: there is some wear apparent on the occlusal restorations at LR67. The dense white colour of these restorations was as a result of a radio-opaque barium-glass filler.Figure 5. Cusp-replacement restorations at LL67 performing satisfactorily at 10 years (photographed in 1996). Some possible wear towards the buccal aspect of the restoration in LL6.
Finally, the authors are aware that some colleagues still have significant problems with posterior composites. It is suggested that, factors influencing longevity of posterior composites are many, but could include those listed below:
Time factors – posterior composites need time to place satisfactorily;
Remuneration system/financial considerations – state funded systems may not be considered to provide adequate remuneration for the time costs of placing posterior composite restorations;
Poor/inconsistent teaching – may confuse clinicians;
Poorly equipped practices – a clinician who decides to place posterior composites for a majority of patients needs to be equipped with the correct materials and matrix systems;8
Poor reputation – some practitioners may still suspect that the wear resistance of composite materials is inadequate, when such difficulties were overcome in the 1990s;
Limited access to postgraduate courses and wide variation in opinion;
Difficulties with isolation – the clinician needs to become adept at rubber dam placement or to be aware of retraction systems such as Optragate® (Ivoclar-Vivadent);
Confusion regarding adhesives, linings, bases;
A confusingly wide range of materials – best to adopt those which have research which suggests that they are appropriate.
Conclusions
The conclusion, based upon this review, is that posterior composites may provide restorations of satisfactory longevity and with survival rates generally similar to those published on amalgam restorations, previously considered as the ‘gold standard’. This review has demonstrated that there is clinical evidence to back up these statements. However, the ability of the operator in placing the restoration may have a profound effect, as several studies have demonstrated. In this regard, practitioners who have not had experience in placing posterior composite restorations in dental school need to be prepared to attend practical continuing education courses if they are not convinced about their skills and success rates with posterior composites, particularly in restoring extensive cavities.