Mitchell L. Introduction to Orthodontics, 4th edn. Oxford: Oxford University Press; 2013
Counihan K, Al-Awhadi EA, Butler J. Guidelines for the assessment of the impacted maxillary canine. Dent Update. 2013; 40:770-777
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994; 64:250-256
Millet D, Welbury R. Clinical Problem Solving in Orthodontic and Paedriatric Dentistry, 2nd edn. Oxford: Churchill Livingstone (Elsevier); 2010
Patel D, Taylor NG. Are patients with impacted canines being referred too late?. Br Dent J. 2016; 221:561-564
Isaacson KG, Thom AR, Atack NE, Horner K, Whaites E. Orthodontic Radiography Guidelines, 4th edn. : British Orthodontic Society; 2015
McIntyre GT. Managing the maxillary canine: 1. Diagnosis, localization and interceptive treatment. Ortho Update. 2008; 1:7-15
Hunter SB. Treatment of the unerupted maxillary canine. Part 1 Preliminary considerations and surgical methods. Br Dent J. 1983; 154:294-296
Orton HS, Garvey MT, Pearson MH. Extrusion of the ectopic maxillary canine using a lower removable appliance. Am J Orthod. 1995; 107:349-359
Husain J, Burden D, McSherry P. Royal College of Surgeons Guideline on the Management of the Palatally Ectopic Maxillary Canine. 2016;
Becker A. Orthodontic Treatment of Impacted Teeth, 3rd edn. Chichester: Wiley-Blackwell; 2012
Power S, Short M. An investigation into the response of palatally displaced canines and an assessment of the factors contributing to favourable eruption. J Orthod. 1993; 20:217-223
Patel J, Rahman S, Spencer RJ. Searching for buried treasure: a review of palatally ectopic canines. Ortho Update. 2008; 1:53-58
Ericson S, Kurol J. Resorption of incisors after ectopic eruption of maxillary canines: a CT study. Angle Orthod. 2000; 70:415-423
Hassan T, Nute SJ. An audit of referral practice for patients with impacted palatal canines and the impact of referral guidelines. Br Dent J. 2006; 200:493-496
Clinical audit: the importance of early detection and referral of impacted maxillary canines Oluwatoyin Aiyegbusi Sukbir Nandra Dental Update 2024 46:5, 707-709.
Authors
OluwatoyinAiyegbusi
BDS, MFDS RCSGlas
Oral Maxillofacial Surgery, Restorative and Special Care Dentistry at Royal Preston Hospital
A retrospective clinical audit was conducted to analyse referrals for impacted maxillary canines received by the Orthodontic Department of Queen Elizabeth Hospital, Kings Lynn. The primary aim of the audit was to determine if patients with impacted maxillary canines were referred at the appropriate age of 12 or under, as required by the Royal College of Surgeons of England guidelines and, secondly, to determine if appropriate radiographs were taken in patients aged 10 and over, as recommended by British Orthodontic Society Radiography guidelines. The results indicate that there is a significant shortfall in meeting the 100% standards set for both clinical guidelines.
CPD/Clinical Relevance: This article highlights the importance of timely referral of suspected impacted maxillary canines and explores the potential consequences to both patient and practitioner of failing to refer patients by the appropriate age.
Article
Permanent maxillary canines begin development high in the maxilla at age 4 to 5 months and crown formation is complete by age 6.1 The canines should be palpable in the buccal sulcus by age 10. At age 11 to 12, it is expected that the maxillary canines should have erupted into their final position; this generally occurs earlier in females than males.2
If a maxillary canine is impacted, there will be failure of its eruption into the maxillary arch. Maxillary canines are the second most commonly impacted teeth after lower third molars, and this affects up to 2% of the general population, with a 2:1 male to female ratio.2 Impacted maxillary canines are often associated with other dental anomalies, such as peg-shaped lateral incisors.3 The cause of canine impaction is obscure, but is commonly attributed to polygenic multifactorial inheritance as there are gender, familial and population variances in its prevalence.4, 5
Assessment of a suspected impacted maxillary canine
Clinical assessment
Palpation of the buccal sulcus should take place from age 9, to confirm the presence of unerupted permanent maxillary canines. A non-palpable canine bulge by age 10 is a clinical indication of impaction of the maxillary canine. The other clinical signs associated with maxillary canine impaction are listed in Table 1.
Non-palpable buccal canine bulge
The canine bulge is non-palpable high in the buccal sulcus by age 10
Presence of a palpable palatal bulge indicating the underlying permanent canine is palatally positioned; this is more common in an uncrowded arch
Presence of a non-mobile retained deciduous canine
The retained deciduous canine is non-mobile by age 10. Particularly suspicious if the adjacent deciduous maxillary canine is mobile or has already exfoilated
The mobility, colour, extent of tooth wear of retained deciduous canines should be assessed to determine their long-term prognosis
Abnormal appearance of adjacent teeth
Missing, malformed or diminutive permanent lateral incisors are strongly associated with palatally impacted canines
Abnormal position of adjacent teeth
Rotated or tilted adjacent teeth suggest the unerupted permanent maxillary canine is overlying the roots of the adjacent teeth
Radiographic assessment
The British Orthodontic Society Radiography guidelines stipulate that by age 10, if there are clinical signs that the maxillary canine may be impacted, a radiographic investigation is required.6 The radiographic signs associated with maxillary canine impaction are listed in Table 2. Two radiographs using the parallax technique should be taken to determine the position of the impacted canine as either buccal or palatal. The majority (approximately 85%) of impacted maxillary canines are located palatally, with the remaining proportion located buccally.7, 8
Abnormal position of the permanent maxillary canine
Two radiographs in parallax view will confirm the position of an unerupted impacted canine as buccal or palatal
Abnormal appearance of the permanent maxllary canine
Cystic changes around the crown of the impacted canine can be seen
Lack of resorption of retained deciduous canine root
The presence of the impacted permanent canine can be associated with failure of the deciduous canine root to resorb
Root length and extent of root resorption of a retained deciduous canine can be assessed to determine its long-term prognosis
Abnormality in the position or appearance of adjacent teeth
The unerupted permanent maxillary canine overlying the roots of lateral incisors is a cardinal sign of maxillary canine impaction
Root resorption of adjacent teeth is common
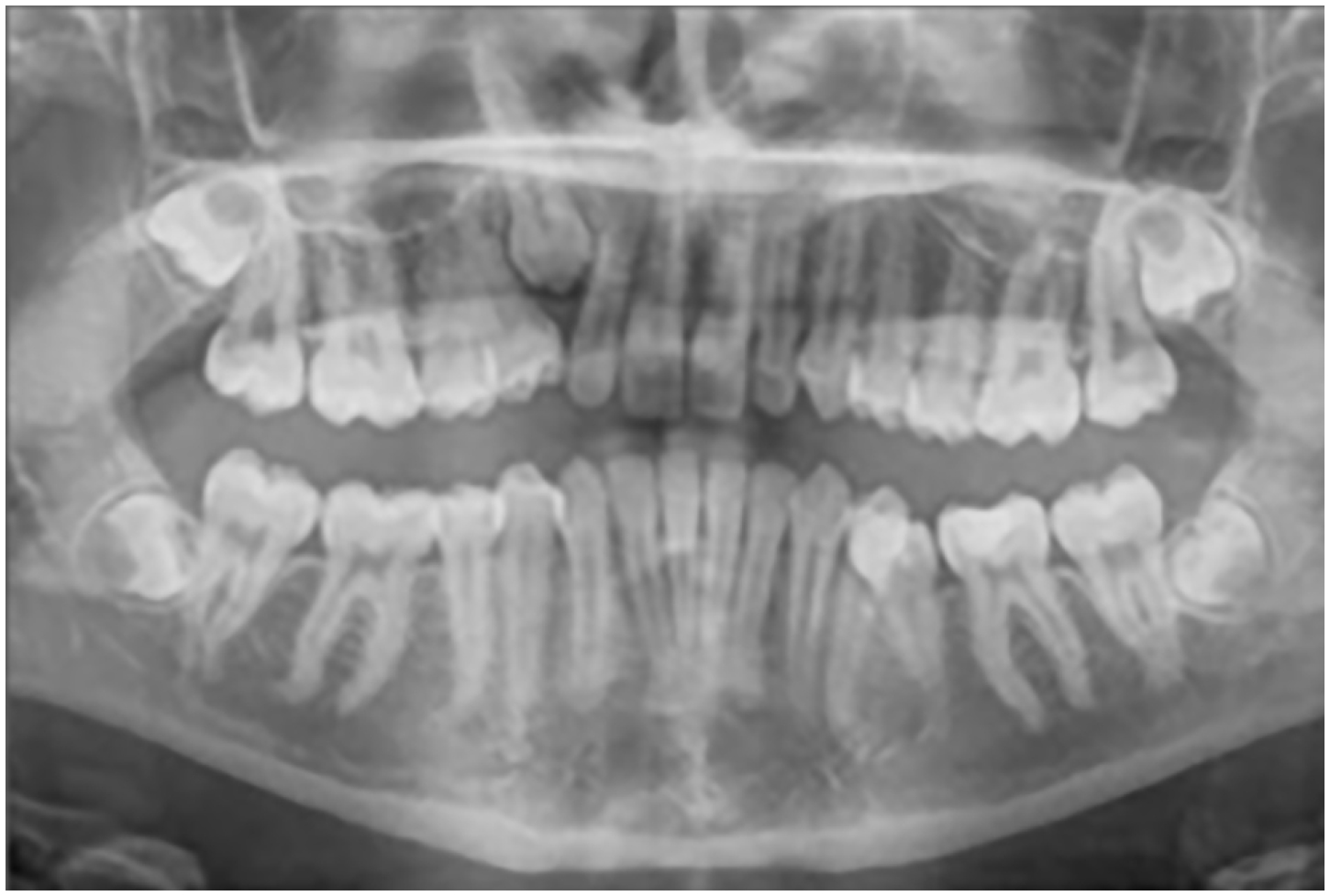
Research has shown that horizontal parallax is a more reliable technique than vertical parallax in locating unerupted maxillary canines.9 Appropriate radiographs for horizontal parallax include a combination of two periapicals or an upper standard occlusal with a periapical radiograph. For vertical parallax, panoramic radiographs can be used in conjunction with an upper occlusal or a periapical radiograph. Figure 1 provides an example of a panoramic radiograph with an impacted maxillary canine present.
Figure 1. A panoramic radiograph showing a single impacted maxillary canine. With full contact between UR2 and UR4, there is limited space for the eruption of the impacted UR3.
Management of impacted maxillary canines
Impacted permanent maxillary canines fall into the highest category of Index of Treatment Need (IOTN) with a score of 5i.1 This is because the impeded path of eruption for the canine is considered to be a great treatment need and is unlikely to improve without active intervention. The Royal College of Surgeons (England) strongly recommends that practitioners seek the opinion of an orthodontist prior to initiating any treatment for impacted maxillary canines.10 By referring patients for specialist advice, they can be assessed and a treatment plan can be devised by a qualified orthodontist. The role of a general dental practitioner is therefore to signpost patients with suspected impacted maxillary canines, at the appropriate age.
Clinical guidelines, published by the Royal College of Surgeons of England on ‘Management of the Palatally Ectopic Maxillary Canines’ (updated in 2016), state that patients with suspected impacted maxillary canines should be referred by age 12 or under.10 By age 12, it is expected that the permanent maxillary canine would have erupted. Thus early referral can mean simple, less invasive treatment options may be available to manage the canine impaction.
Interceptive extraction of deciduous canines
If timely referral occurs, interceptive extraction of a deciduous maxillary canine can be carried out to facilitate eruption of the impacted permanent canine into its correct position.5 Interceptive extraction is simple, cost-effective and can be readily carried out in general practice, under the request of a qualified orthodontist. Studies have shown that, for patients between the ages of 10 to 13, there is a reasonably high probability that the interceptive extractions will be successful.11 Where the permanent maxillary canine is located palatally in an uncrowded arch, interceptive extraction of the deciduous canine is particularly likely to align the maxillary canine into its normal path of eruption; there is a reported success rate of up to 78% in such cases.7, 12
Close monitoring of the patient following interceptive extraction is required. If there is no improvement in the canine position within 12 months, other treatment options will have to be explored. Consideration should also be given to balance the extraction of one retained maxillary primary canine with the removal of the opposite maxillary retained canine, to prevent a centreline shift.4
Other treatment options for impacted maxillary canines
A delay in the detection and/or referral of impacted maxillary canines can have serious implications for a patient. If a patient is age 13 or over, interceptive extraction of the deciduous canine is unlikely to be successful in correcting the position of an impacted permanent maxillary canine.
The alternative treatment options that will have to be considered are:
Leave the impacted canine in situ;
Surgical exposure and orthodontic alignment;
Surgical extraction and orthodontic alignment;
Transplantation of the permanent canine into the correct position.
No active treatment, ie leaving the impacted canine in situ, would require periodic radiographic monitoring to detect any spontaneous migration of the impacted canine or pathology caused to adjacent teeth. Treatment options such as surgical exposure and alignment would be invasive and costly in terms of clinical time for both the patient and orthodontist. Surgical extraction of the permanent canine may result in aesthetic and functional problems, as this tooth has a long root, good bony support and is advantageous in lateral excursive movements.2 Transplantation of the maxillary canine may possibly damage adjacent teeth and there is also the risk of ankylosis of the transplanted canine.13
Consequences of failure to treat impacted maxillary canines
Possible sequelae of untreated impacted canines include cyst formation, internal or external resorption of the impacted canine.13 Root resorption of adjacent permanent incisors is also a known risk in 12% to 48% of cases.14, 15 The incidence of incisor root resorption associated with an impacted maxillary canine differs with the radiographic imaging technique used, due to superimposition of incisor roots and the crown of the impacted canine.2 Compared with conventional plain radiographs, the incidence of root resorption has been reported to be up to five times higher in Cone Beam Computer Tomography (CBCT).4
Finally, there is also the added possibility of litigation for the referring practitioner, if he/she is found to be negligent in the detection or referral of impacted maxillary canines. The correct timing of referral is therefore imperative to ensure patients receive the most appropriate care.
Audit aims and objectives
A clinical audit on the referral pattern of impacted maxillary canines to the Orthodontic Department at Queen Elizabeth Hospital, Kings Lynn was conducted. The primary aim of the audit was to determine if patients with impacted maxillary canines were referred at the appropriate age of 12 or under, as required by the Royal College of Surgeons of England guidelines and secondly, to determine if appropriate radiographs were taken in patients aged 10 and over, as recommended by British Orthodontic Society Radiography guidelines. The objective of the audit was to highlight the importance of early referral of impacted maxillary canines and the potential consequences of delayed referral.
Standards
Royal College of Surgeons (England) Guidelines – All patients with suspected impacted maxillary canines are to be referred by age 12.10
British Orthodontic Society Radiology Guidelines – Radiographic investigation should be carried out in all patients with suspected impacted maxillary canines who are aged 10 or above.6
Method
This was a retrospective audit project. The Clinical Governance Department provided the medical records of 300 randomly selected patients, from all patients who had new patient appointments at the Orthodontic Department of QEHKL during March 2016 to March 2017. Data was collated on the age, gender and referral source. Of the 300 medical records analysed, 55 patient referrals were regarding suspected impacted maxillary canines.
Results
Analysis of 300 new orthodontic referrals
The average age of new patients referred to the Orthodontic Department was 14.2. The proportion of males to females was 36% to 64%, respectively. The sources of referral consisted of general practitioners (90%), specialist orthodontist (7%) and community dentists (3%).
Analysis of 55 impacted maxillary canine referrals
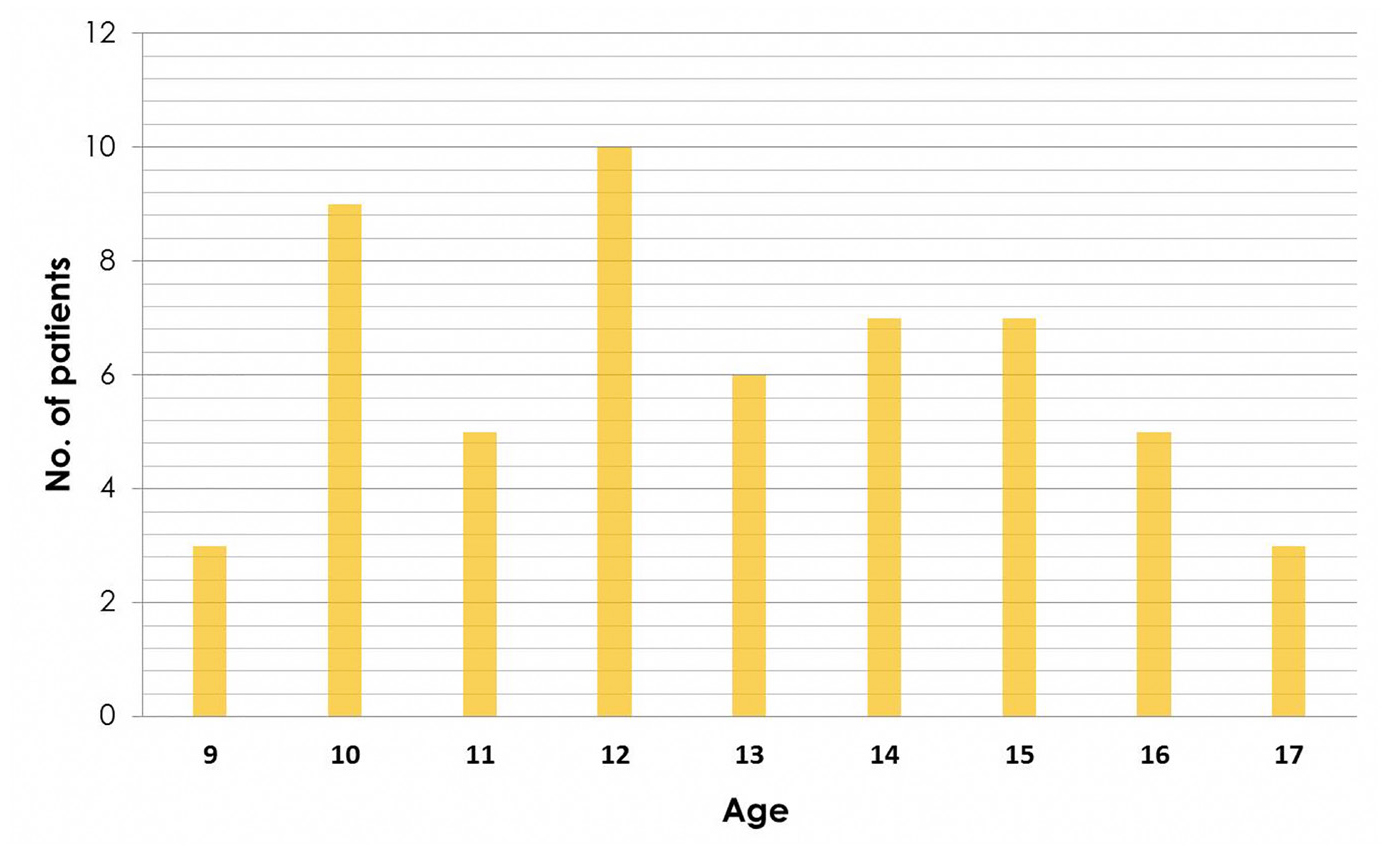
Impacted maxillary canines account for almost a fifth (18.3%) of patient referrals to the Orthodontic Department at QEHKL. Canine impaction was almost twice as common in females as it was in males; with a proportion of males to females of 37% to 63%, respectively. The referral sources consisted of general dental practitioners (GDPs) (86%), specialist orthodontist (14%) and community dentists (0%). Figure 2 shows the age distribution of the patients referred regarding impacted maxillary canines, the average age of referral was 12.8 In total, 27 out of 55 (49%) patients were referred at the appropriate age, 12 or under. The remaining 28 patients (51%) were referred late, at age 13 or over. A total of 24 out of 55 patients (44%) were referred with bilateral impacted maxillary canines and the remaining 31 patients (56%) had a single impacted maxillary canine. A total of 21 out of 55 (38%) referral letters included information confirming or excluding the presence of a palpable canine bulge. Some referral letters provided information regarding the risk factors associated with impacted maxillary canines and 31 out of 55 patients were confirmed to have retained deciduous canines; this feature was noted by 45% of referring practitioners in such cases. Abnormality to the permanent lateral incisor was confirmed in 23 out of 55 patients; this feature was noted by 34% of referring practitioners in such cases.
Figure 2. Age analysis of patients with impacted canine referrals. Mean age is 12.8
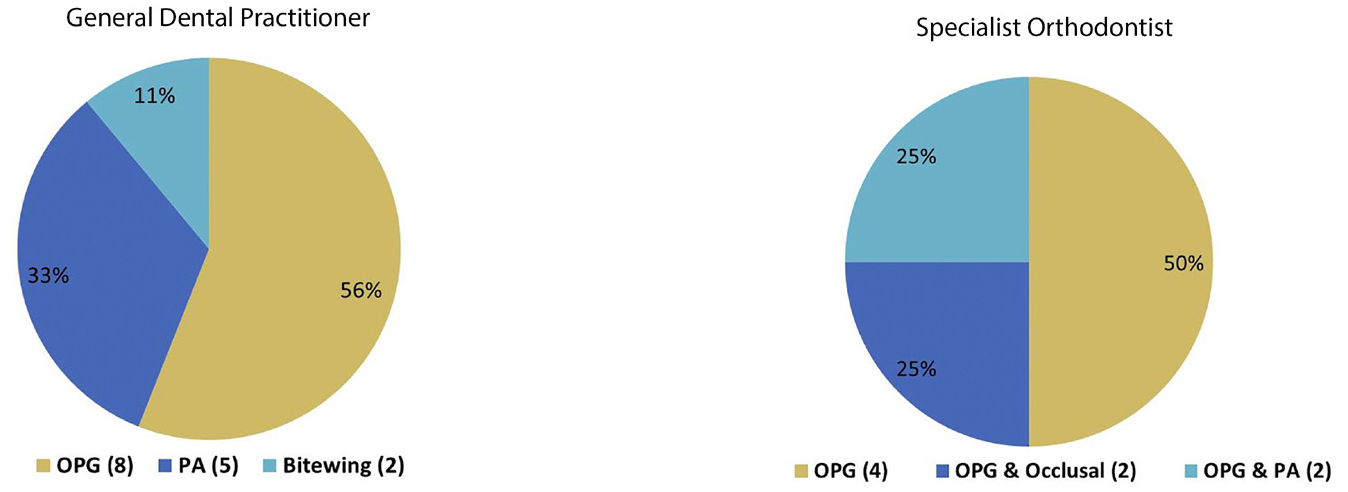
Appropriate radiographs were included in 22 out of 55 (40%) of referrals. These patients were all age 10 and above and 14 out of 47 GDPs provided radiographs; consisting of OPGs (56%), periapicals (33%) and bitewing radiographs (11%) (Figure 3). All 8 specialist orthodontists included radiographs in their referral letter; consisting of an OPG (50%), a combination of OPG and upper occlusal (25%) or a combination of OPG and a periapical (25%).
Figure 3. The type of radiographs included in referral letters for impacted maxillary canines.
Discussion
A significant proportion of patient referrals failed to meet the standard set based on the Royal College of Surgeons (England) guidelines (Table 3). There is therefore lost opportunity for interceptive measures in a significant number of patients. This affects the treatment options available, number of appointments and overall cost of treatment.
Criteria
Standard
Fulfilled criteria
Variance from standard
Royal College of Surgeons (England)
Patients referred by age 12
100%
49%
-51%
British Orthodontic Society Radiology guidelines
Appropriate radiograph taken for patients aged 10 and over
100%
40%
-60%
By age 10, the presence of the canine should be confirmed by palpation of the canine bulge in the buccal sulcus. Only 38% of referring practitioners noted presence or absence of a canine bulge. Practitioners should state whether the canine bulge is buccal, palatal or non-palpable in the referral letter. A total of 31 out of 55 (56%) of patients in this audit presented with retained deciduous canines. If a deciduous canine is present and non-mobile by the age of 10, one should suspect that the unerupted permanent canine may be impacted. If there is a reasonable degree of mobility, this is an indication that the unerupted permanent canine may still erupt.11
The findings of this audit show that 41% of impacted maxillary canines were associated with abnormality to the lateral permanent incisor; which was missing, peg-shaped or exhibited root resorption. This is similar to the reported prevalence of approximately 48% in studies and therefore practitioners should be suspicious in such clinical presentations.11 A total of 40% of referrals included radiographs; it is important that referral letters include radiographs that have been taken for patients, to avoid repeat radiation exposure to patients.
In summary, the main problem found with impacted maxillary canines referrals, to the Orthodontic Department of QEHKL is that 51% of patients are being referred later than recommended, at age 13 and above. The key message is that practitioners should be aware of normal canine development and anomalies associated with impacted canines, such as peg-shaped lateral incisors and retained deciduous canines.2 If impaction of a maxillary canine is suspected, an appropriate radiograph should be taken (in patients age 10 and over) and there should be timely referral for orthodontic opinion, by no later than age 12.
Changes to implement
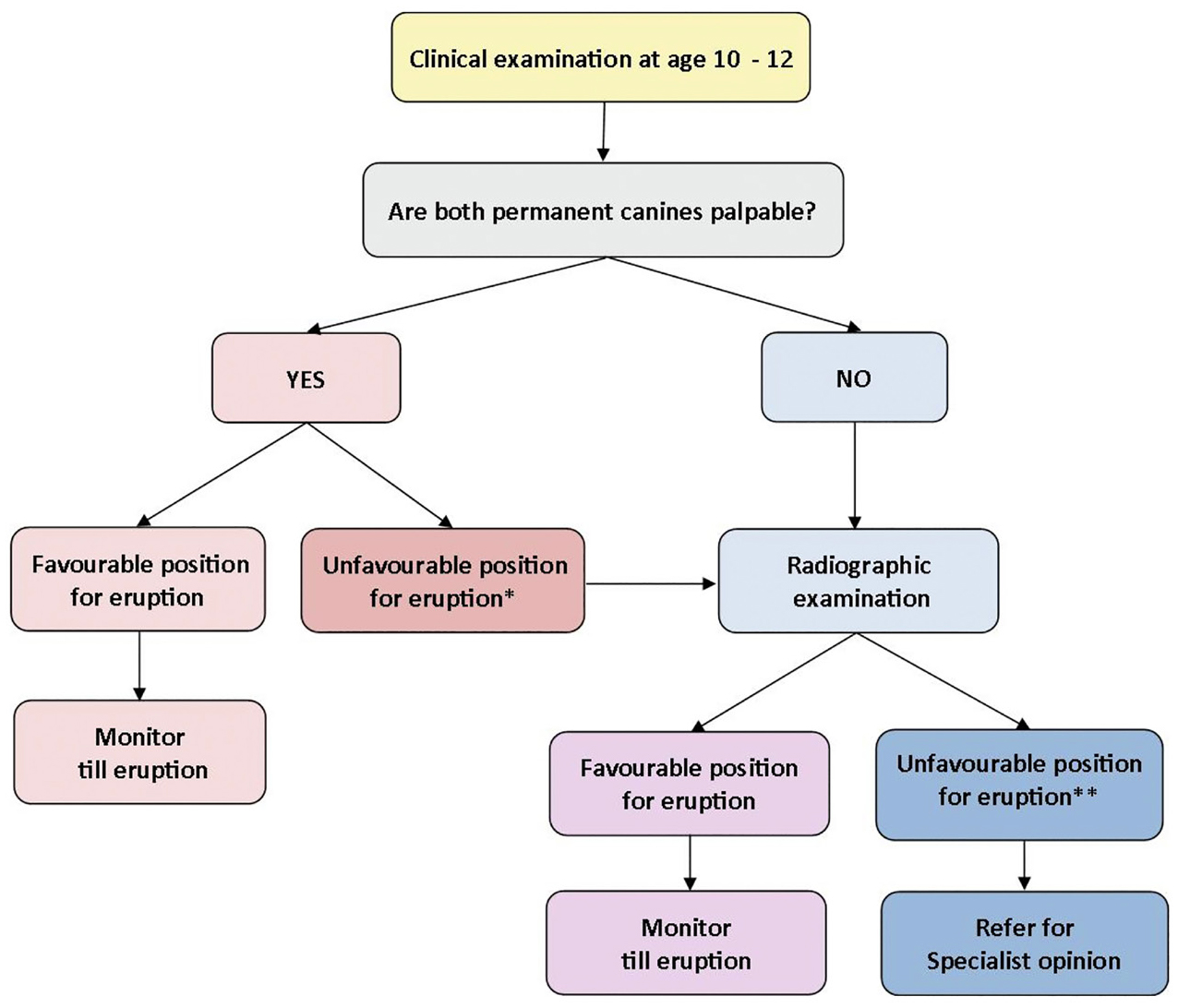
Write to all referring practitioners with the key findings from the audit. This letter would include an algorithm for when to refer suspected impacted maxillary canines (Figure 4) and a summary of the key information that would be required for a high quality referral letter.
Collaborate with referring practitioners and share suggestions to improve the referral patterns of impacted maxillary canines into secondary care. This would be carried out by hosting a teaching session at Queen Elizabeth Hospital, Kings Lynn for all local dental practitioners and dental care professionals.
Engage with the local orthodontic groups or MCN/LDC/BDA groups to disseminate the audit findings.
Conduct a second cycle of the audit to determine if there is an improvement in the timing of referrals for impacted maxillary canines.
Figure 4. Algorithm to determine which patients require referral regarding impacted maxillary canines.
Conclusion
Clinical audit can be an effective tool for improving the quality of care provided to patients. This audit highlights the issue of delayed orthodontic referrals for impacted maxillary canines. The findings show that there is scope to improve the timing and quality of orthodontic referrals regarding impacted maxillary canines. A significant proportion of patients are being referred late which leads to the increased likelihood of more extensive treatment being required to treat impacted maxillary canines. The findings of this audit show that, in order to meet the set standard of 100% for both clinical guidelines, there is a need for further education and training for referring practitioners on the detection and management of impacted maxillary canines. Figure 4 provides an algorithm to follow in order to determine when to refer patients for specialist opinion regarding impacted maxillary canines.