
References
The oral implications of mental health disorders part 2: depression
From Volume 46, Issue 2, February 2019 | Pages 119-124
Article

Depression
Depression is a common mental health disorder affecting 4−10% of people in England and approximately 300 million people globally.1, 2 It is a psychiatric disorder characterized by low mood and can include feelings of sadness, despair or discouragement. It can often involve loss of interest in usual activities, social withdrawal and somatic symptoms, including sleep and appetite disturbance.3, 4 In order to arrive at a diagnosis of depression, the altered behaviour must persist for a minimum of two weeks.4 Chronic stress is strongly associated with depression, with a possible causal relationship between stressful life events and major depressive episodes. The neurobiology underlying stress and depression is thought to result from molecular and cellular abnormalities that interact with genetic and environmental factors.5 It is essential for dental professionals to understand and recognize the possible oral manifestations of depression. This knowledge can help undiagnosed patients receive an appropriate early referral to a medical practitioner, and will also be of benefit in managing the oral manifestations of this disease.
Mucosal lesions
The oral tissues are highly responsive to psychological influences; thus it has been suggested that psychological disturbance can compromise oral health. Psychological factors can alter the markers of the nervous system (catecholamines: adrenaline, noradrenaline and dopamine), endocrine system (cortical and aldosterone) and immune system (T-cells, B-cells and NK-cells), which in turn can lead to oral disease pathogenesis.6, 7 This interaction between psychological and biological systems increases the prevalence of conditions such as burning mouth syndrome (BMS), oral lichen planus (OLP) and recurrent aphthous stomatitis (RAS) in patients with depression.6
The aetiology of BMS is thought to be largely neuropathic. BMS has a strong psychological relationship with anxiety and stress, and a high number of patients with BMS are reported to suffer from moderate to severe depression. Patients with depression may encounter burning mouth symptoms as either a consequence of xerostomia or as a side-effect of antidepressant medication.8 Furthermore, prolonged psychosocial and emotive stress may contribute to the initiation and clinical expression of OLP. These factors may also precipitate in the transformation of reticular OLP to the erosive form.9 Individuals with moderate and severe depression are likely to exhibit a higher incidence of RAS compared to patients with mild depression.6
Dental lesions
Individuals with depression often have little interest or motivation to maintain adequate self-care activities, which can adversely affect oral hygiene and compliance with treatment. Poor oral hygiene may result in an increased incidence of dental caries. The risk of dental caries formation may be exacerbated further by a cariogenic diet. Patients with depression have a suppressed serotonin metabolism, which can lead to an increased preference for carbohydrates. This creates conditions favourable for the growth of aciduric bacteria.3, 4 Ineffective biofilm disruption associated with poor oral hygiene can allow the aciduric bacteria to colonize and multiply.4 Drug-induced xerostomia is a common side-effect of antidepressant medication, which can also facilitate the formation of dental caries due to reduced salivary flow and compromised buffering action.3, 4
Patients with depression are more likely to exhibit signs of bruxism because parafunctional activity is a physical manifestation of emotional stress and anxiety.10 In addition, bruxism can be experienced by patients taking anti-depressants because these drugs raise extrapyramidal serotonin levels, thus inhibiting the dopaminergic pathways that control these movements.3, 11 Chronic bruxism can lead to severe tooth wear and dentine hypersensitivity (Figure 1). Myofascial pain and temporomandibular joint disorders may also arise due to parafunctional activity.10

Periodontal lesions
There is evidence that a bi-directional relationship exists between depression and periodontal disease, with multiple pathways linking the two (Figure 2).12 The different mechanisms proposed for the effect of depression on periodontal health include dysregulation of the hypothalamic-pituitary-adrenal (HPA) system, behavioural changes and anti-depressive medication.5, 12 Each mechanism can independently induce periodontal destruction, however their combination may interact to magnify the effect.12

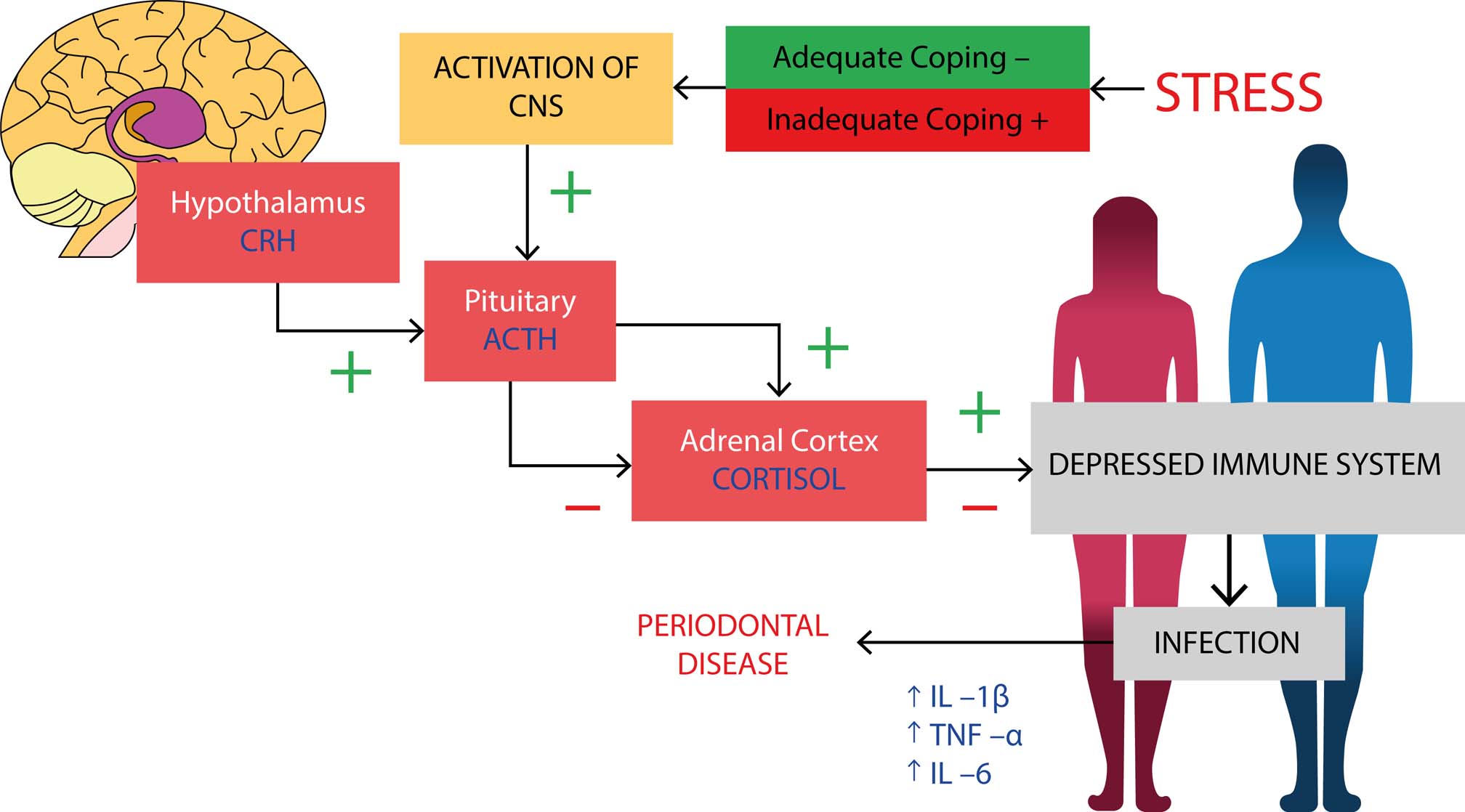
Depression can lead to biological changes within the body, including dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis. Stress mediators, including monoamines, neuropeptides and steroid hormones, convey stress signals to the central nervous system and in turn this affects the HPA axis. This will cause a shift in cortisol balance, which results in compromised immune defences and excessive secretion of pro-inflammatory cytokines. These pro-inflammatory cytokines include interleukin-1beta (IL-1β), interleukin-6 (IL-6) and tumour necrosis factor alpha (TNF-α).5 Through these processes, depression might affect progression of periodontal infection in susceptible patients and may compromise treatment outcome through delayed wound healing.12 The biological effect of stress on the body and its potential progression to periodontal disease is depicted in Figure 3.5 Behavioural changes that may occur in patients with depression include poorer oral hygiene, increased smoking and excessive alcohol consumption.12, 13 Negligence for oral hygiene can result in plaque and calculus accumulation, which can lead to gingivitis and an increased risk of developing periodontitis.3, 4, 14 A dose-effect relationship exists between cigarette smoking and severity of periodontal disease, highlighting its significant effect on periodontal destruction. Smoking causes both functional impairment in gingival microcirculation and structural changes within fibroblasts. Also, it can have a significant effect on the immune system, modifying the humoral and cellular immune systems and affecting the cytokine and adhesion molecule network.15 Moreover, increased alcohol consumption is often associated with depression and this has the potential to lead to alcohol dependence. Evidence shows the combined interaction of alcohol and smoking has a synergistic effect in the development of oral and pharyngeal cancers.16 Excessive alcohol consumption can also alter host immune responses, increasing susceptibility to micro-organisms. Alcohol can increase both the prevalence and severity of periodontitis, with a positive correlation existing between attachment loss and alcohol consumption. This occurs as alcohol can cause oral dehydration and reduced salivary flow, therefore high alcohol consumption can contribute to an increased rate of biofilm formation and accumulation.17 The effect of these behavioural changes on the periodontium can be exacerbated by drug-induced xerostomia. Saliva is more viscous in patients with xerostomia, resulting in enhanced food and bacteria adherence to teeth and consequent plaque accumulation, which may ultimately contribute to periodontal disease.18
The concept that periodontal disease may influence the onset of depression is based upon a cell-mediated response to the periodontal pathogens, leading to chronic, low-grade inflammation. Patients with depression often have increased oxidative and nitrosative stress, which contributes to the neuro-progression of this condition. It is also common for these patients to have increased serum levels of both pro-inflammatory cytokines and acute phase proteins. The pro-inflammatory cytokines include IL-1, IL-6 and TNFα and the acute phase proteins are C-reactive proteins (CRP), complement factors and chemokines. Periodontal disease is also associated with high levels of systemic inflammation, particularly IL-6, TNF-α and CRP. These may potentiate oxidative and nitrosative stress and inflammatory processes, which may consequently lead to an increased susceptibility of depression.12
Patients with periodontal disease may also be more likely to experience depression through psychological effects of tooth loss and complications such as halitosis, both of which may arise as a consequence of periodontits.12 Halitosis, which may be related to oral neglect and periodontal disease, may lead to embarrassment causing personal and social isolation.19, 20 Tooth loss may impair masticatory function which can affect nutritional status. It can also have a major impact on aesthetics, significantly affecting self-esteem and confidence.12, 21 Periodontal disease can have a detrimental effect on quality of life and well-being which, if severe, could potentially lead to depression.
Tooth loss has a significant influence on quality of life, especially when it affects well-being, appearance and nutritional status. Periodontal disease may also relate to depression through the shared common factor of systemic disease. There is significant literature suggesting an association between periodontitis and systemic diseases, such as cardiovascular disease and diabetes.17, 22, 23 In addition, epidemiologic studies provide strong evidence that chronic psychosocial stress and depression increase the risk of atherosclerotic cardiovascular disease, diabetes and other systemic conditions, as well as adversely affecting the course and outcome of the conditions.5, 24 This suggests that there may be a relationship between periodontal disease and depression, which is indirectly linked by systemic disease.
Gingivitis artefacta is a type of periodontal disease that is caused by habitual injury to the gingival tissues, resulting in localized recession defects. The condition is usually associated with an emotional disorder, such as depression, and has a higher occurrence in children and females. The self-inflicted injury often involves scratching or picking at the gingiva with a fingernail or any foreign object.25 Appropriate diagnosis of the lesion can often be difficult as the clinical presentation can mimic that of a number of more common causative factors associated with recession defects.26
Other oral symptoms
Xerostomia, as previously indicated, is a common oral side-effect in patients taking anti-depressant medication. Table 1 lists commonly prescribed anti-depressant medications and their associated side-effects.3, 4, 11 Anti-depressants have either anticholinergic or antimuscarinic action, which suppress the parasympathetic nervous system and will inhibit the effects of acetylcholine on the salivary gland receptors. Adrenergic sympathetic vasoconstriction reduces blood flow to the salivary gland, thus reducing salivary flow. The drugs may also interfere with acinar and salivary duct function, resulting in changes to both salivary flow rates and composition.11 These changes to saliva secretion can lead to other oral symptoms including dysgeusia and stomatitis.11
| Medication | Side-Effects |
|---|---|
| Selective Serotonin Reuptake Inhibitor (SSRIs), eg |
Xerostomia, dysgeusia, stomatitis, gingivitis, glossitis, bruxism, discoloured tongue |
| Serotonin – Norepinephrine Reuptake Inhibitor, eg |
Xerostomia, dysphagia, nausea, anxiety, dizziness, nervousness, headache, sweating, bruxism |
| Norepinephrine – Dopamine Reuptake |
Xerostomia, dysgeusia, stomatitis, gingivitis, glossitis, bruxism, dysphagia, angioedema |
| Tricyclic Anti-depressants, eg |
Xerostomia, sialadenitis, dysgeusia, stomatitis, tongue oedema, tongue discoloration |
| Monoamine Oxidase Inhibitors, eg |
Xerostomia |
Chronic facial pain and depressive disorders share common pathophysiological characteristics and a comorbidity between these conditions frequently exists.4, 27 A major life event, such as divorce or bereavement, often precedes onset of chronic facial pain by up to 6 months. This type of life stressor has also been implicated in increasing the risk of a major depressive episode. Chronic facial pain and depression have a similar epidemiological background, with a peak prevalence in younger women and a lower incidence in older age groups. Therefore, due to this relationship between these conditions, depression should be considered in patients experiencing chronic facial pain.27
Conclusion/Management in the dental setting
It is important for dental professionals to explain the benefit of good oral hygiene to patients, both in preventing dental caries and periodontitis. Similarly, appropriate dietary advice should be offered, reducing sugar and carbohydrate intake. This should be common practice to all patients, however it may need to be emphasized and monitored in patients with depression.
Additionally, dental professionals need to ensure that they regularly ask their patients about their perceived stress levels. This could be attained by the use of a simple 1−10 scale, with 0 representing no stress and 10 maximum stress. Stress levels are important to document as they may have an impact on the immune system, particularly if not adequately managed. They may also indicate likelihood of compliance with behavioural changes, such as improving oral hygiene or smoking cessation. Patients with high stress levels or those struggling to cope with stress may benefit from referral to their medical practitioner. A medical practitioner may provide support to manage stress and assess whether the patient is suffering with an underlying mental health disorder. The medical management of depression can involve either non-pharmacological or pharmacological treatments.
It is always essential for a thorough medical history to be taken, recording all medications and being aware of possible oral side-effects. Drug-induced xerostomia is a common side-effect of anti-depressants, which can be managed appropriately if identified. Sugar-free gum and lozenges can be recommended to patients to stimulate saliva production or artificial saliva substitutes can be offered. Improving salivary flow may also help patients experiencing burning mouth symptoms. Fluoride supplements can be offered in caries management.3 Finally, occlusal assessment and appropriate management is important for patients exhibiting bruxism and chronic facial pain. These patients may benefit from the use of a hard occlusal guard to relieve masticatory muscle tenderness and avoid further tooth wear.