An audit investigating the management of diabetic patients in general practice, in relation to periodontal health Rana Wali Sophina Mahmoud Amrit Chaggar Yasamin Hamrang-Yousefi Dominic Hurst Dental Update 2024 46:1, 707-709.
Research has found a close relationship between the disease progression of diabetes and periodontitis. The aim of this audit is to determine the compliance of general dental practitioners (GDPs) with recommendations from the Delivering Better Oral Health toolkit (2014) for the management of diabetic patients. The final section of this article discusses the factors that affect the prognosis of immediate natural tooth bridges. Providing information on prognosis is an important part of the consent process; this includes patient factors and clinician factors.
CPD/Clinical Relevance: There is evidence of a bi-directional relationship between diabetes and periodontitis.
Article
Diabetes is an ever-increasing concern amongst patients and medical practitioners. It has received substantial media coverage aiming to raise awareness of its debilitating and potentially life-threatening complications.1 Research has also revealed the bi-directional relationship between periodontal disease and diabetes.2 Our role in the management of these patients has thus become ever-important to our holistic patient care.
Evidence in the UK suggests diabetic control is often poor, with only about 35.9% (2012–2013 National Diabetes Audit figures) of all patients achieving the targets for blood glucose, cholesterol and blood pressure that are recommended to reduce their risk of developing complications.
A retrospective audit was conducted at four different northeast London training dental practices, within the Redbridge, Barking and Dagenham borough, where a proportion of patients suffer from Type 2 Diabetes and its complications. The prevalence of diabetes in this area is high at 10%, compared to the national average of 8.6% (Public Health England, 2016).3
As dental practitioners, there is a unique opportunity to promote not only oral health, but general health on a regular basis to patients who may not be seeing their general medical practitioner (GMP) as often. Furthermore, the current evidence heightens the role of the GDP in the multidisciplinary management of diabetic patients.
This audit was based on an understanding that the dentist has a crucial role in the multidisciplinary management of a diabetic patient. In this regard, it is the duty of care of clinicians to liaise with GMPs where diabetes control is a concern, and to educate patients that their ongoing periodontal disease can hinder their diabetic control.
Criteria and standards
The ‘Delivering Better Oral Health’ (DBOH) toolkit4 was introduced to support dentists in improving patients' oral and general health, with a focus on preventive measures. Performance was measured against the recommendations made by the 3rd edition of the DBOH toolkit which states that:
Dentists should:
Inform diabetic patients of the relationship between periodontal disease and diabetes, and the related risks;
Enquire about and record their level of glycaemic control (HbA1c);
Encourage patients to maintain good diabetes control and to follow-up with the diabetes physician regularly;
Write to the diabetes physician for guidance on patients' diabetes status;
Inform the physician about the patient's periodontitis status to help to tailor diabetes care and advice appropriately.
Since this audit was introduced for the first time and aimed to explore new ideas, it was important initially to set a realistic degree of compliance that practitioners felt that they could achieve.
A target of 90% compliance was agreed for the following:
Recording diabetes control;
Informing patients of the risks and relationship between periodontal disease and diabetes;
Encouraging patients to maintain good diabetes control.
A lower expected degree of compliance, 70%, was set for:
Recording HbA1c;
Writing to the diabetes physician for guidance on diabetic status and informing the physician about the patient's diabetes status.
Objectives
Our key objectives were:
To determine the compliance of GDPs with the recommendations for management of diabetic patients in the ‘DBOH Toolkit for Prevention’ (2014);
To apply ‘Evidence-based practice’ to our management of diabetic patients;
To place the management of diabetic patients on the agenda for continuous quality improvement.
Methods
An audit tool was generated to record the relevant data under the headings given in Table 1.
Patient Details
Diabetic History
Recorded Management
No.
DOB
Initials
Type I/II Diabetes
HbA1C
Level of Control (Good/Poor)
Diet/Medication
Risks explained
Liaison with GMP
This was piloted by collecting a few patient records and checking that the tool captured all the information that was relevant to our aims. It was demonstrated to other dentists in the practices to ensure that everyone shared a common understanding of the data being gathered.
The pilot stage was followed by creation of an electronic toolkit, which allowed for accurate and easy auditing, including relevant evidence-based information and a summary of results.
A total of 175 patient records dating from June 2014 were randomly selected. There was no gender, age or dental practitioner bias. These files were carefully analysed for the relevant information, which was then inserted into the electronic toolkit for processing.
Results of first cycle
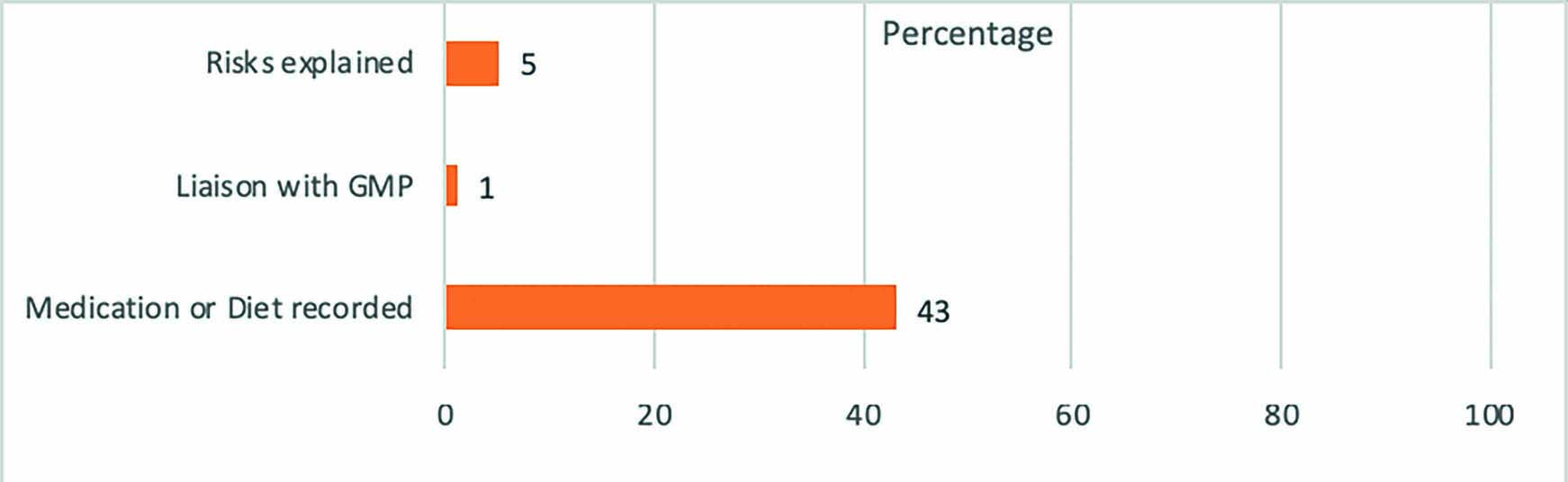
A total of 175 patients were included in the primary audit cycle. The results are shown in Figure 1. They reveal poor compliance with the DBOH standards in most areas. Dentists were recording the presence and type of diabetes and the medication taken, however, they were not enquiring further about the diabetic control or discussing appropriate management with patients. Risks of diabetes in relation to periodontal disease were rarely discussed.
Figure 1. Audit cycle 1.
Implementing change
The following actions were piloted and implemented at the four north-east London training practices:
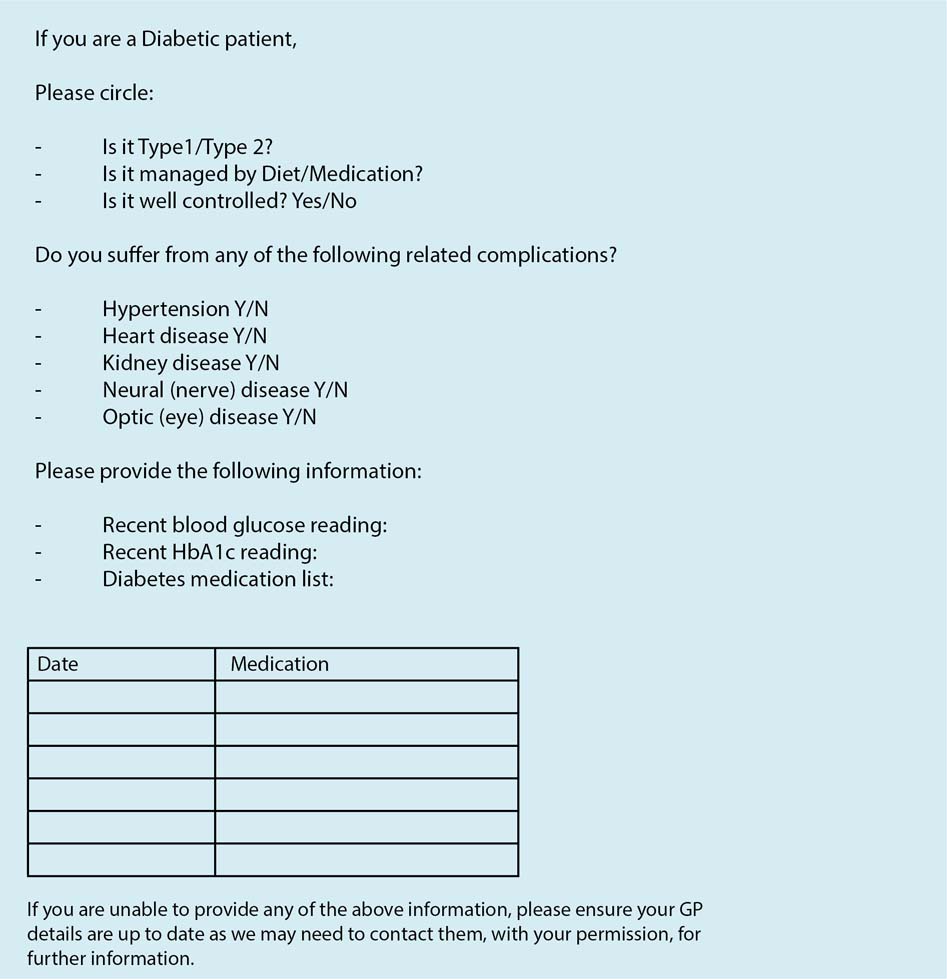
A diabetic patient medical history proforma was attached to the existing medical questionnaires (Figure 2);
A template letter to GMPs was made accessible to all surgeries in either hard-copy format, or incorporated into the practice software;
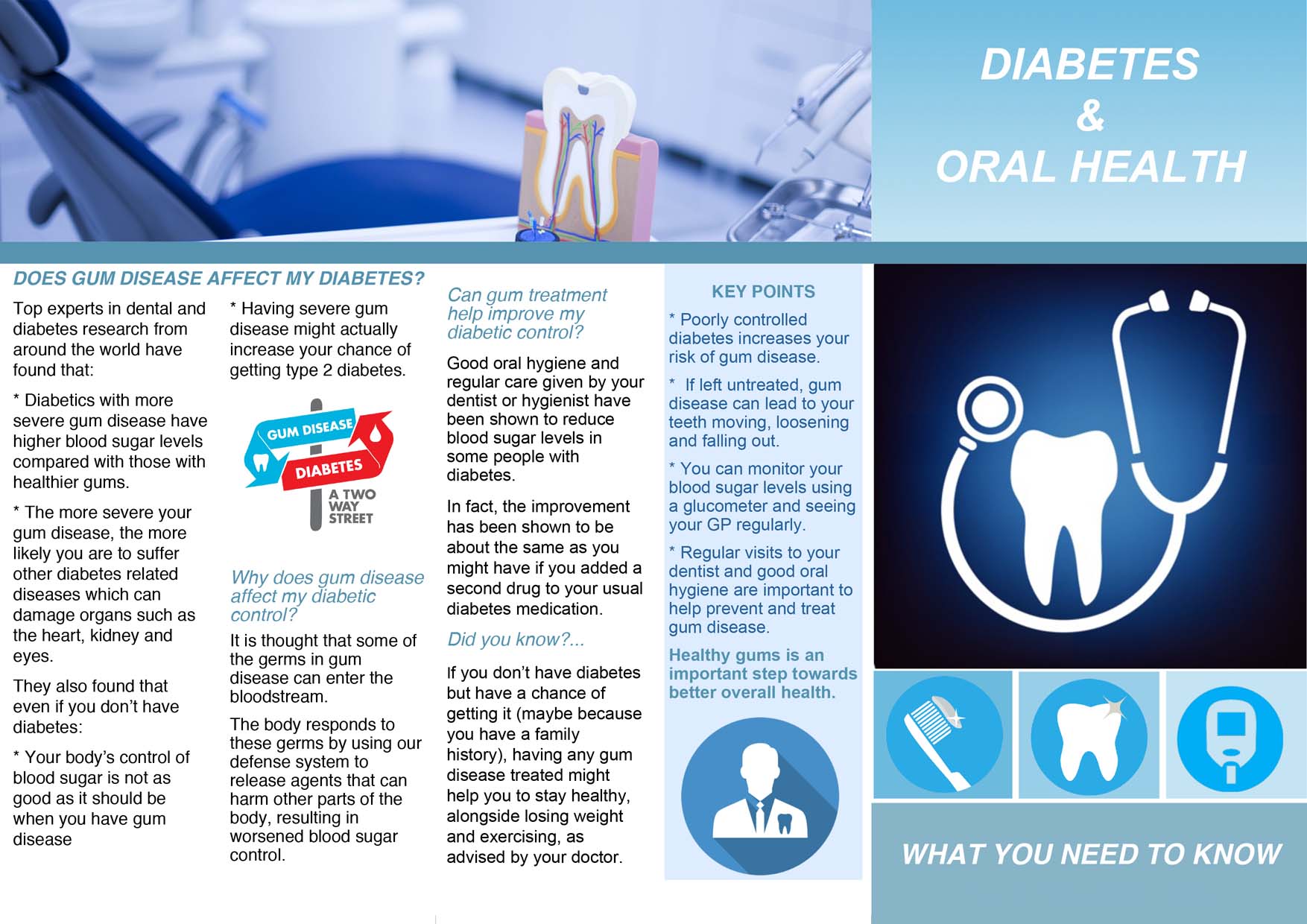
A patient information leaflet was created, presenting the information from ‘Diabetes and gum disease’ authored by Professor Preshaw in a patient-friendly format (Figure 3).
A GDP information pack explaining the audit process and including a guide to understanding HbA1c values was produced and made available in the practices.
Figure 2. Diabetic patient medical history proforma.Figure 3. Patient information leaflet.
These interventions were chosen as they demonstrated quick and easy methods of improving record-keeping and patient management. Dentists, nurses, receptionists and patients were involved in the pilot; feedback was gathered with regards to:
Ease and speed of use/delivery;
Willingness to participate in the use and delivery of these resources;
Perceived usefulness to patients and practitioners.
Dental practitioners showed a willingness to integrate these implementations into their patient care and agreed that they were quick, easy and effective aids to meeting the standards. Receptionists played an active role in integrating the diabetic medical history form with the existing practice proforma or onto the electronic software. They also ensured that multiple copies of the patient information leaflet were printed and available in all surgeries and at the reception desk. Patients gave positive feedback about the leaflets and considered the idea of communication between dentists and GMPs regarding their diabetic control to be good.
Results of second cycle
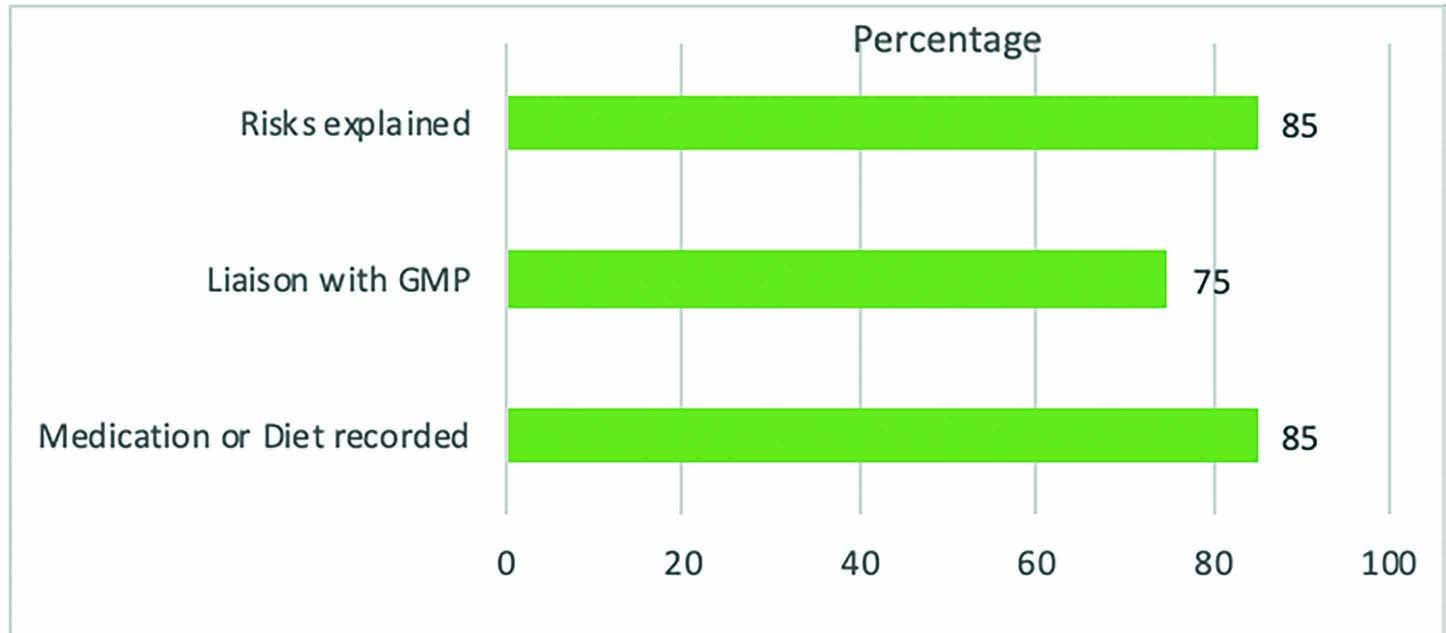
A second audit cycle was carried out three months following the implementations. Significant improvement was seen in all areas of patient management and history-taking (Figure 4). The target for compliance was met in most aspects of diabetic patient management, however, there was still room for improvement in explaining risks to patients where the 90% target was not met.
Figure 4. Audit cycle 2.
Discussion
The completion of this audit demonstrated how simple measures can help improve diabetic patient care, and promote awareness of the related risks.
The audit is limited, in so far that combined efforts of healthcare professionals are required to ensure the best patient outcomes. In addition, where prevalence of diabetes is relatively low, greater motivation to comply with the national standards may be necessary. As dentists, there is a need to promote a culture of ‘putting the mouth back into the body,’ and treating the patient as a whole to the best of our ability.
Conclusion
This audit intends to promote better management in general dental practice of diabetic patients. The current evidence on the bi-directional relationship between diabetes and periodontitis should not be dismissed in our everyday practice. The first audit cycle demonstrated significant room for improvement in complying with the guidance, and this was proved possible with the implementation of basic tools.
The authors would encourage auditing management of diabetic patients to identify the current performance with an aim to improve it. Since completion of this audit, the electronic toolkit has been modified to help other practitioners to assess efficiently the management of diabetic patients in their practices.
With recommendations already in place, the implementations suggested in this audit can be put into place to help practitioners follow these recommendations.
By having a more informed and active role in the management of diabetic patients, the dentist, along with the GMP, can work hand-in-hand to identify and manage poorly controlled diabetes and periodontitis.