Valachi B, Valachi K. Preventing musculoskeletal disorders in clinical dentistry. J Am Dent Assoc. 2003; 134:1604-1612
Paul JE. Are you sitting comfortably?. Dent Update. 1981; Nov/Dec:559-566
Paul JE. A Manual of Four Handed Dentistry.Berlin: Quintessence Publishing Co; 1980
Burke FJT, Main JR, Freeman R. The practice of dentistry: an assessment of reasons for premature retirement. Br Dent J. 1997; 182:250-254
Rundcrantz BL, Johnsson B, Moritz U. Cervical pain and discomfort among dentists. Epidemiological, clinical and therapeutic aspects. Part 1. A survey of pain and discomfort. Swed Dent J. 1990; 14:71-80
Shugars D, Miller D, Williams D, Fishburne C, Strickland D. Musculoskeletal pain among general dentists. Gen Dent. 1987; July:272-276
Maillet JP, Millar AM, Burke JM, Maillet MA, Maillet WA, Neish NR. Effect of magnification loupes on dental hygiene student posture. J Dent Educ. 2008; 72:33-44
Liss GM, Jesin E, Kusiak RA, White P. Musculoskeletal problems among Ontario dental hygienists. Am J Ind Med. 1995; 28:521-540
Hagberg M, Wegman DH. Prevalence rates and odds ratio of shoulder-neck diseases in different occupational groups. Br J Ind Med. 1987; 44:602-610
Brown J, Burke FJT, Macdonald EB Dental practitioners and ill health retirement: causes, outcomes and re-employment. Br Dent J. 2010; 209
Hill KB, Burke FJ, Brown J, Macdonald EB, Morris AJ, White DA, Murray K. Dental practitioners and ill health retirement: a qualitative investigation into the causes and effects. Br Dent J. 2010; 209
Pilkington RJJ. Clinical simulation in dental ergonomics: Part 1. Team in Practice. 2011; 8:7-9
Pilkington RJJ. Clinical simulation in dental ergonomics: Part 2. Team in Practice. 2011; 8:11-12
Park JP, Kim KH, Kuh SU, Chin DK, Kim KS, Cho YE. Spine surgeon’s kinematics during discectomy according to operating table height and the methods to visualize the surgical field. Eur Spine J. 2012; 21:2704-2712
Ergonomics and the Dental Worker. In: Murphy DC (ed). : American Public Health Association; 1998
Paul JE. Perfect posture for the dental team CD. Smile-on Productions. 2006;
Gagnon M. The efficacy of training for three manual handling strategies based on the observation of expert and novice workers. Clin Biomech. 2003; 18:601-611
Koes BW, Van Tulder MW, Ostelo R Clinical guidelines for the management of low back pain in primary care: an international comparison. Spine. 2001; 26:2504-2512
McGill S. Ultimate Back Fitness and Performance 3rd edn.: Backfitpro Inc; 2006
Sahrmann S. Diagnosis and Treatment of Movement Impairment Syndromes.Oxford: Elsevier (Mosby); 2002
Nachemson AL. The load on lumbar disks in different positions of the body. Clin Orthop. 1966; 45:107-122
Adams M, Bogduk N, Burton K, Dolan P. The Biomechanics of Back Pain 2nd edn.Oxford: Churchill Livingstone, Elsevier; 2006
McGill SM, Brown S. Creep response of the lumbar spine to prolonged full flexion. Clin Biomech. 1992; 7:43-46
Schultz AB, Warwick DN, Berkson MH Mechanical properties of human lumbar spine segments. Part 1. Response in flexion, extension, lateral bending and torsion. J Biomech Eng. 1979; 101:46-52
Gandavadi A, Ramsay JRE, Burke FJT. Assessment of dental student posture in two seating conditions using RULA methodology – a pilot study. Br Dent J. 2007; 203:601-605
Occupational health problems in the dental setting have been highlighted in the past mainly focusing on cross infection and acquired illnesses, such as hepatitis B and HIV. Musculoskeletal problems have been documented over the years but little has been done to address them. This article highlights the potential problems that may arise if certain precautions are not taken into consideration. The main objectives are to make the dental professional aware that not looking after one's musculoskeletal health could result in premature retirement.
CPD/Clinical Relevance: Simple measures such as ergonomic working with the correct use of dental equipment and conditioning of the body will hopefully aid the professional throughout his/her career.
Article
Dentistry has long been associated with the development of musculoskeletal problems.1 In the past, dentistry was commonly taught in a standing position, usually with the practitioner standing in a stooped, distorted position, placing considerable stress on the lower lumbar spine. Ellis Paul devised the Four Handed Dentistry2 (Close Support) technique once chairside assistance dentistry became the norm. The aim was to try and keep practitioners working in an ergonomic fashion to avoid prolonged, distorted positions which would place increased loads on their spines. This ergonomic form of working improved efficiency, productivity, reduced stress and was the start of ‘Team Dentistry’.3
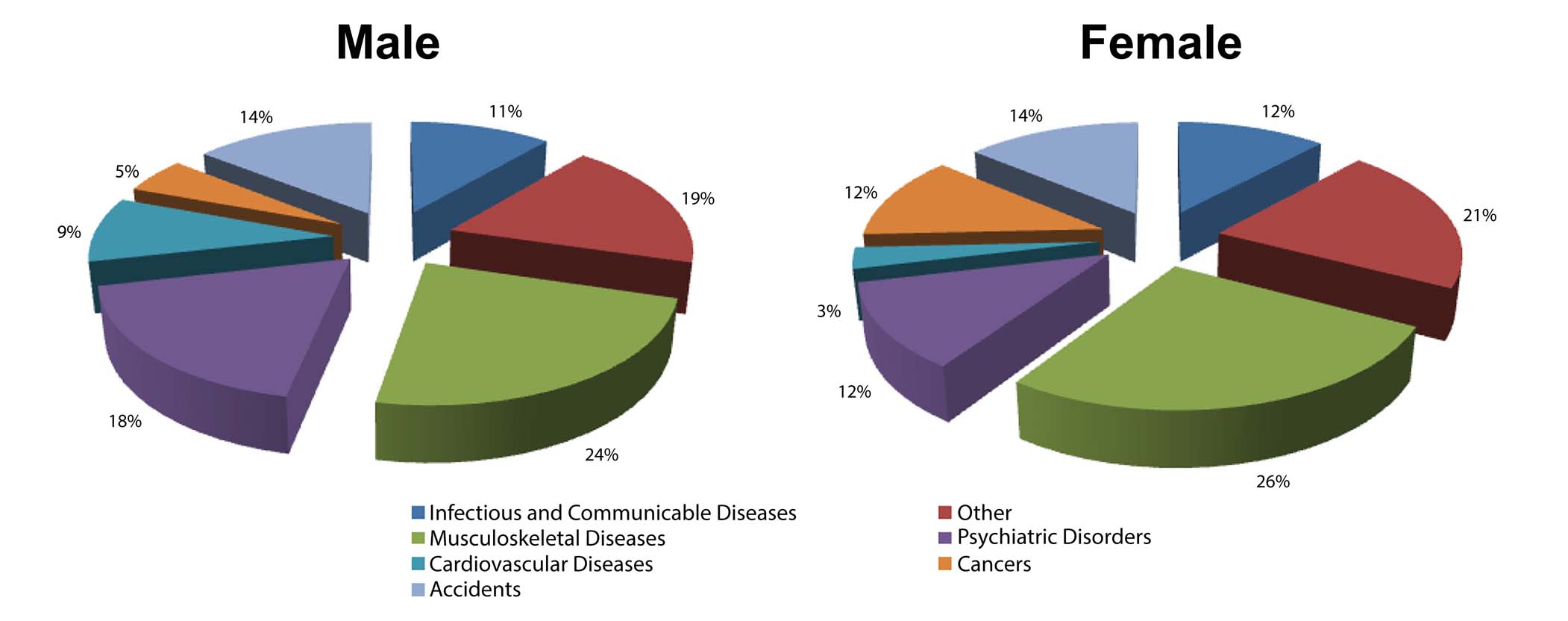
There have been many articles4,5,6,7,8,9,10-11 written on the topic of the incidence of musculoskeletal problems in the dental profession, some of which have been summarized in Table 1. Burke et al4 highlighted that it was the most common reason for premature retirement based on data (1981–1992) from The Dentists' Provident Society. The figures from their 2007 claims showed that musculoskeletal problems accounted for 24%–26% (total of 1507 claims) as the main cause of early retirement (Figure 1). These figures have remained static and other critical illness insurance companies have shown that it is one of their leading causes of early retirement.10-11
Causes of retirement due to depression, musculoskeletal disease and skin conditions
Figure 1. Dentists' Provident Society claims for premature retirement (2007).
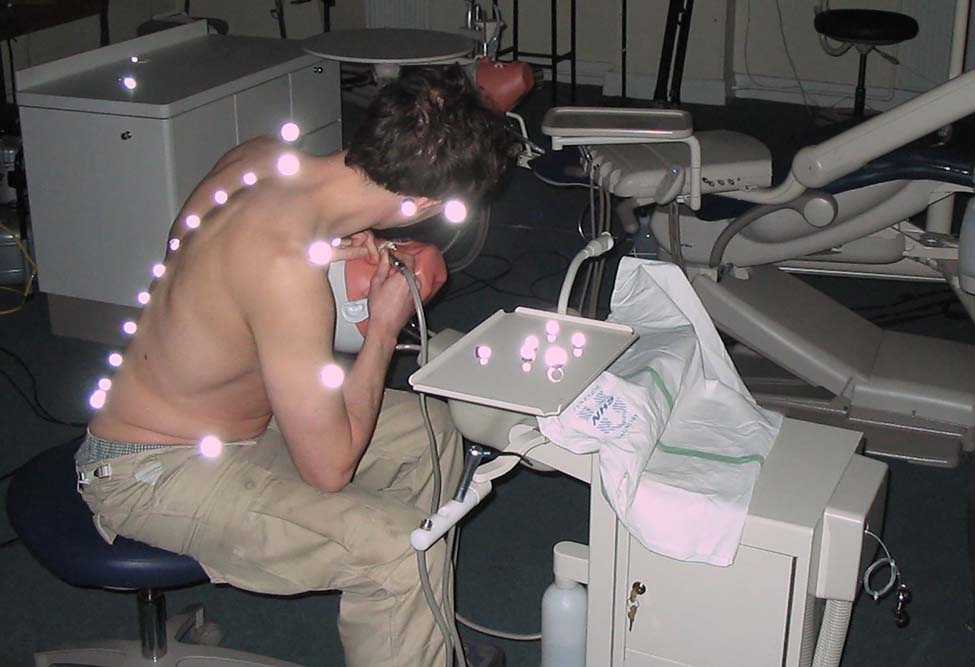
Several years ago, the present author demonstrated how final year dental students' neck posture could be improved with the implementation of an ergonomically designed surgery, the use of four handed skills, good seating and the use of loupes whilst performing simple restorative techniques. In this study, the biomechanical recording system of skin markers and infra-red motion capture cameras recorded the operator's body movements. The study demonstrated how these simple measures resulted in the dental students adopting a less distorted neck and shoulder posture when compared to working alone on the phantom head models.12,13
In Figures 2 and 3, the author is adopting the usual distorted posture in an attempt to use direct vision to visualize the teeth that need to be restored. The posterior and lateral views show the spine being held in a flexed and rotated position, predominantly at the cervical and lumbar spine.
Figure 2. Poor posture due to direct vision working.Figure 3. Lateral view of spine.
Such recording of spinal motion has extended into other surgical specialties where, once again, the chief complaint was the operator complaining of musculoskeletal pain whilst working in an awkward and distorted body posture. Using a motion analysis system, similar to our study with dentists, a study of spinal surgeons performing a simulated procedure was noted to be improved when using loupes and adjusting an operating table between the umbilicus and sternum.14
Prevention
Dentists, hygienists and dental assistants are required to adopt non-neutral postures throughout most of the working day. The postures adopted usually require prolonged static contraction of the trunk and the scapular musculature, combined with repetitive contractions of the muscles in the wrist, hand and fingers during fine motor movements. The dental team tend to adopt these awkward postures in order:
To obtain optimal view of teeth within the patient's mouth, often whilst maintaining a seated posture;
To provide a comfortable position for the patient;
To co-ordinate their positions relative to assistants, with whom they share limited space;
To manoeuvre complex equipment and reach for instruments.15
Ergonomics
For anyone working in the dental profession, to acquire knowledge of ergonomics will be most beneficial at the start of one's career. In its simplest definition, ergonomics could be defined as ‘fitting the task to the person’. In this simplest form the excellent approach devised by Ellis Paul puts these measures into performing close support dentistry.16
However, in sports medicine the approach is more about how we can condition the body to withstand the stresses being placed on it whilst performing. In this analogy, the approach of ergonomics is ‘changing the person to fit the task’. Gagnon17 observed expert weightlifters and concluded that their lifting strategies and personal body movements led to their health success. If dentists take this approach we can educate our professional colleagues in how to minimize occupational health-related musculoskeletal problems from poor lifting and prolonged poor posture. Then it is possible to try and minimize the times when an ideal position may not be able to be adopted whilst performing the various work-related tasks.
The postgraduate course run by the author had the elements shown in Table 2 to educate the dental personnel.
How to build a solid spine foundationAnatomical, biochemical and motor control of the spineReduce the risk of injuryImplementation of ergonomic aids whilst performing dentistry (4 handed principles/Loupes/Seating/Surgery design)Science of spine stabilityStabilization exercise programme (Core abdominal muscles/Neck and scapular stability)
If the same analogy in dentistry is used, then the strategies to adopt would be to use a varied posture as much as possible whilst working to maintain a neutral posture, so that distorted positions are not maintained for long periods. This would prevent vulnerable areas of the musculoskeletal system being subjected to a lifetime of continual tissue strain.
Reducing pain and improving function for patients with back pain involves two components:
Removing the stressors that create or exacerbate damage;
Enhancing activities that build healthy supportive tissues.
It must be stressed that anybody developing back pain must first seek medical advice as back pain can be a manifestation of an underlying sinister pathology. A review with a registered medical practitioner to exclude any ‘red flags’ would be a primary care guideline recommendation.18
Exercises
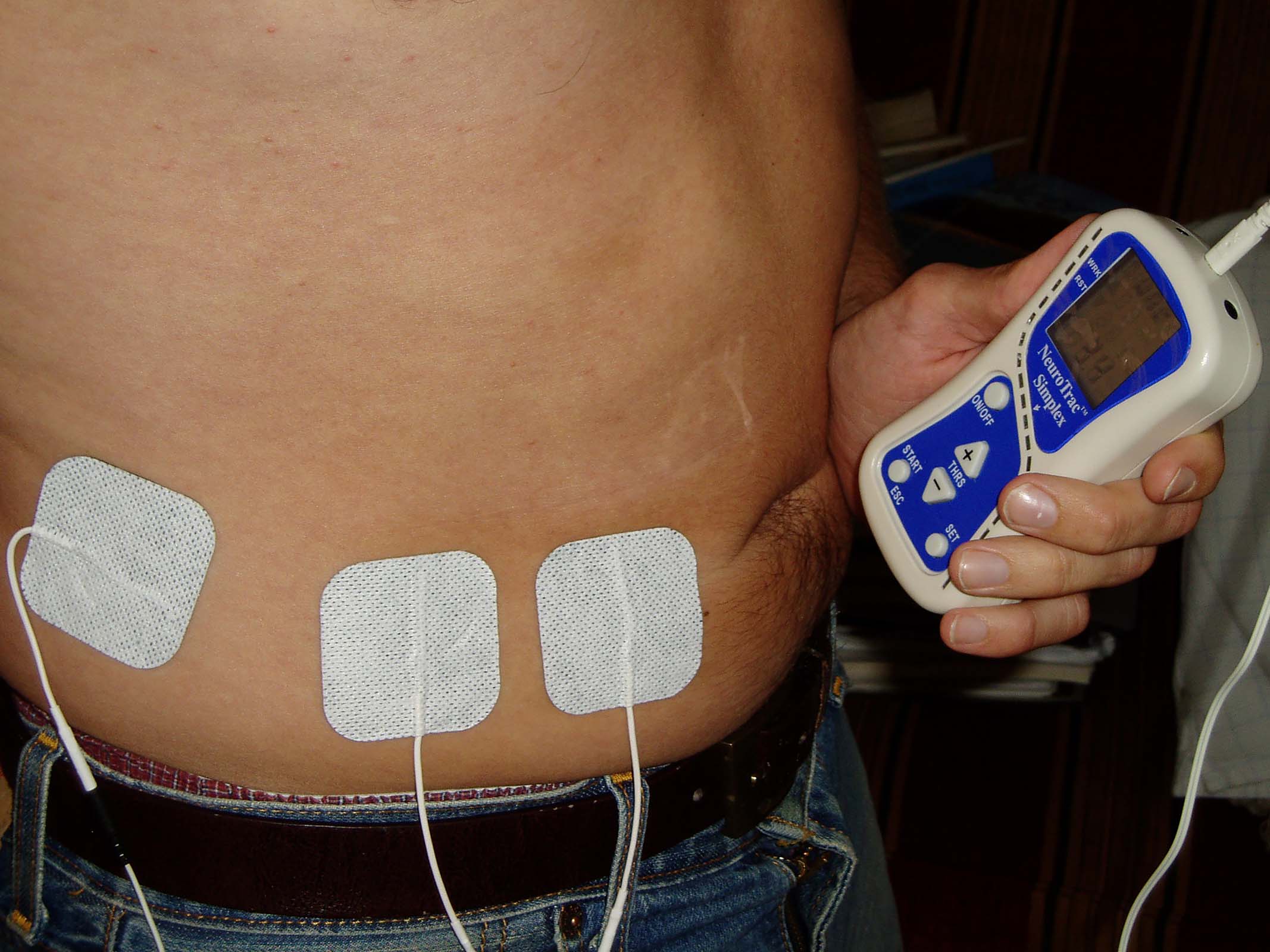
First, in order to develop a good posture one needs to develop a good core (made up of a three-layered abdominal wall muscular, namely external oblique, transversus abdominus and internal oblique) from which the main stability is formed. In patients who have developed a poor core muscle strength, activation of these muscles may be difficult. Physiotherapists can use techniques such as biofeedback where skin electrodes pick up faint muscle contractions and help patients visualize activation of the muscles. This helps muscle fibres contract again and regain muscular tone and strength (Figure 4).
Figure 4. Biofeedback.
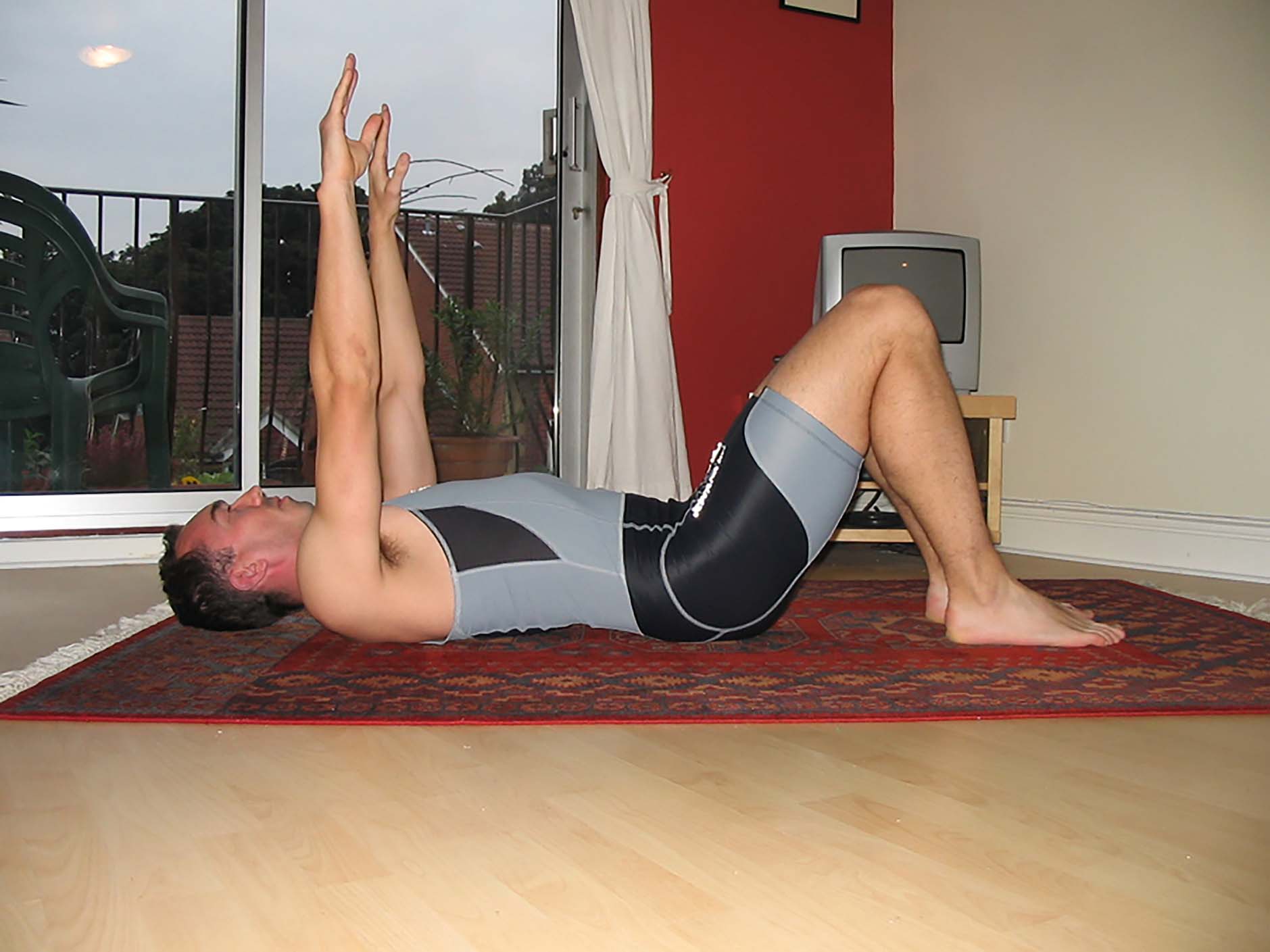
The abdominal brace activates the three layers of the abdominal wall with no hollowing or drawing in. The main core muscles can be further built-up with the classic Professor McGill stability lumbar spine exercises. Affectionately known as ‘the big 3’,19 the approach to rehabilitation is summarized in Table 3. They comprise a modified spine curl which does not load the lumbar spine as the typical curl up does. The bird dog starts on all fours with extension of the leg whilst ensuring that spinal motion is minimal. The patient has to maintain the lumbar lordosis and ensure no dropping or elevation of the pelvis on the side of the extended leg. In performing this exercise, locking the ribcage to the pelvis whilst raising the leg indicates lumbar torsional control. If the performance is poor there will be hiking of the pelvis which indicates poor lumbar torsional control (Figures 5 and 6).
Assessment of the underlying problem
Rehabilitation
Tailor-made for each individualAssess the patient as a whole, look for:
Instability issues
Stiffness issues
Where are the problems?Faulty movement patternsNo single approach may work for that individual depending on the problem
Groove motion/motor patterns and corrective exerciseBuilding the whole body and spine stabilityIncreasing enduranceBuild strengthDevelop speed, power, agilityGluteal amnesia/dominance correctionCurl upSide bridgeBird dogSquat patterns
Figure 5. Starting on all fours.Figure 6. Bird dog with lifting of leg ensuring that spinal motion is minimal.
For more exercise information, follow the link: www.backfitpro.com
Neck exercises
Most dental personnel complain of the upper spine and shoulder being a common source of musculoskeletal discomfort.1,5,9 To build up this vulnerable area will involve working from a strong core and building scapular stability and neck extensor stability. Figures 7, 8 and 9 show common exercises to do this. It is recommended that the reader follows the Sahrmann exercises20 for more guidance.
Figure 7. Shoulder drops starting position, keeping ribcage engaged.Figure 8. Shoulder drops extending the arms ensuring that the ribcage keeps engaged to the pelvis.Figure 9. Dart position which helps build up the extensors in the neck.
Loupes
Many dental schools have started to introduce the use of magnification to their dental students. This has started to expand into the dental hygienist programme, as their use has been shown to improve the operator's working posture. The University of British Columbia has integrated an ergonomic approach to teaching its dental students and hygienists dental ergonomic concepts early in their clinical practice. For further advice on how they achieve this follow the links:
www.ergonomicsdental.com
www.dentistry.ubc.ca/ergo
then click onto the study module resource link.
A concise summary of the benefits of various magnification aids can be accessed via the following online resource:
Known mechanical changes associated with seated posture include a number of issues.
There is an increase in intradiscal pressure when compared to standing postures.21
Looking at the spinal MRI scan in Figure 13 (the author's) does not show the whole story. The lower lumbar discs show loss of height and signs of early disc degeneration. However, the process of associated back pain is a complex mechanism of altered spinal movements under spinal loading and biopsychosocial factors.22
Figure 13. Lumbar spine wear.
Sitting in a slumped position causes the lumbar spine to ‘creep’ in the posterior passive tissues of the spine,23 which decreases posterior stiffness and increases shearing movement.24 This puts the discs at this part of the spine under more considerable damage.25
Strategies to reduce back troubles during prolonged sitting:
Use an ergonomic chair – properly, the ideal sitting posture is a variable one that migrates the internal loads among the various tissues.
Get out of the chair. Regular change of posture is recommended.
In between patients, a stretch of the spine and holding the stretch to release the stresses that may have accumulated in the spinal tissues, especially the lumbar region, is beneficial.
Seating saddle seats (Figure 14) are ergonomic seats which are designed to tilt the pelvis forward, keeping the hips at roughly 130 degrees with the feet firmly resting on the floor. It allows the natural lumbar lordosis of the lumbar spine to be easily maintained and keeps disc pressure minimal in this position. This stable pelvic position then helps promote upper limb stability, which is important for the operator performing fine motor control movements. Gandavadi et al26 showed how dental students using a saddle seat were able to maintain a more acceptable working posture than those using a conventional seat.
Figure 14. Saddle seat.
All well designed seats have parts that can be varied so that they can be adjusted and made more bespoke for the individuals using them. The stem height can be altered for height. The saddle size comes in various widths, depending on user's pelvis size.
Other ergonomically designed seating has the same features of height adjustment and castors to allow easy movement. The one shown in Figure 15 allows the operator to adopt a natural lumbar lordosis as the pelvis is held in a neutral position with the height adjusted so that the front of the thighs are sloping downwards.
Figure 15. Ergonomic seat with pedestal ring.
When the height of the operator and dental assistant is compared, the assistant needs a couple of inches height advantage as this makes his/her job easier in providing soft tissue retraction at this height. To achieve this, and depending on the height difference between the operator and assistant, usually the assistant's chair is fitted with a pedestal ring so that his/her feet can be firmly supported.
Summary
The purpose of this article is to educate the dental team in how to be aware of potential musculoskeletal problems that may arise in the dental team. Its main focus is the musculoskeletal disorders that arise as a result of a poor working posture and poor conditioning of the back. There are more musculoskeletal complaints that have been well documented in the dental literature covering topics such as carpal tunnel syndrome and epicondylitis. Hopefully, the resources that are mentioned in this article will direct the reader to more informative texts covering such topics.