Petersson EE, Andersson L, Sorensen S. Traumatic oral vs non-oral injuries. Swed Dent J. 1997; 21:55-68
Glendor U. Epidemiology of traumatic dental injuries – a 12 year review of the literature. Dent Traumatol. 2008; 24:603-611
DiAngelis AJ, Andreasen JO, Ebeleseder KA, Kenny DJ, Trope M, Sigurdsson A, Andersson L, Bourguignon C, Flores MT, Hicks ML, Lenzi AR International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012; 28:2-12
Andreasen JO, Andreasen FM, Skeie A, Hjørting-Hansen E, Schwartz O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries – a review article. Dent Traumatol. 2002; 18:116-128
Al-Nazhan S, Andreasen JO, Al-Bawardi S, Al-Rouq SA. Evaluation of the effect of delayed management of traumatized permanent teeth. J Endod. 1995; 21:391-393
Flores MT, Andersson L, Andreasen JO, Bakland LK, Malmgren B, Barnett F, Bourguignon C, DiAngelis A, Hicks L, Sigurdsson A, Trope M. Guidelines for the management of traumatic dental injuries. II. Avulsion of permanent teeth. Dent Traumatol. 2007; 23:130-136
Andreasen JO, Borum MK, Jacobsen HL, Andreasen FM. Replantation of 400 avulsed permanent incisors. 4. Factors related to periodontal ligament healing. Dent Traumatol. 1995; 11:76-89
Andersson L, Andreasen JO, Day P, Heithersay G, Trope M, DiAngelis AJ, Kenny DJ, Sigurdsson A, Bourguignon C, Flores MT, Hicks ML International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 2. Avulsion of permanent teeth. Dent Traumatol. 2012; 28:88-96
Finucane D, Kinirons MJ. External inflammatory and replacement resorption of luxated, and avulsed replanted permanent incisors: a review and case presentation. Dent Traumatol. 2003; 19:170-174
Effective management of traumatic dental injuries remains a challenge for clinicians worldwide. Ideally, treatment should be carried out as soon as possible to optimize patient comfort and wound healing. However, delays often happen for a variety of reasons and sometimes the appropriate skills are not readily available. A fit and well 22-year-old female patient was seen by her local hospital's A&E department after sustaining serious injuries. The avulsed upper left canine had been partially replanted, but was in the wrong position. Other displaced teeth had not been repositioned completely and were incorrectly splinted. She had been in constant pain and unable to eat properly when she was eventually seen at King's College Hospital, 12 days later. Clinical and radiographic examination revealed multiple extrusive and lateral luxation injuries, as well as a dento-alveolar fracture of both the upper and lower labial segments. The existing splint was removed and the displaced teeth and the avulsed canine tooth were repositioned and this was verified radiographically and compared to a patient photograph (a ‘selfie’) which she had taken, rather fortuitously, prior to her serious injury.
A new flexible splint was placed. Root canal treatment was initiated for the avulsed upper left canine tooth and endodontic treatment was eventually needed in all the injured teeth. In spite of the long delay, resolution of the symptoms and satisfactory healing was achieved and she was placed on annual recall. This case demonstrates that, even with very delayed presentation, the correct diagnosis and pragmatic management of severe traumatic dental injuries can still produce patient comfort and a reasonable prognosis.
CPD/Clinical Relevance: The main aim of this case report is to describe the management of a patient with very delayed presentation of multiple luxation injuries along with a dento-alveolar fracture and an avulsed tooth in a young adult helped by a photograph on her mobile phone.
Article
Traumatic dental injuries comprise 5% of all injuries for which patients seek treatment in A&E.1 According to a 12-year review of the literature, 33% of adults have experienced dental trauma, with the majority occurring before the age of nineteen.2 Effective management of traumatic dental injuries remains a serious challenge for dental clinicians worldwide.3 Ideally, the treatment of traumatic dental injuries should be carried out on an emergency basis to optimize patient comfort and wound healing.4 Various authors have suggested that having the correct diagnosis and treatment quickly, coupled with appropriate follow-up of injuries, is critical for improving patient outcomes.3
Delayed treatment or having inappropriate treatment for traumatic dental injuries have been associated with an increased risk of pulp necrosis and root resorption in young patients.5 Previous authors have correlated the effect of treatment delays on pulpal and periodontal ligament healing.4 Luxation injuries were recommended to be treated within the first 24 hours, even though some of that evidence is questionable.4
Avulsion of permanent teeth is considered to be the most serious dental injury.6 It is one of the few real emergency situations in dentistry.6 The time factor is critical for healing and immediate replantation is indicated, if at all feasible.4,7 Following an extra-oral dry time of 60 minutes or more, virtually all the periodontal ligament cells die.8
The aim of this case report is to describe the management of an adult patient with delayed presentation of multiple luxation injuries, a dentoalveolar fracture and an avulsed tooth. The patient was seen soon after the injury but, unfortunately, the correct diagnoses were not made and repositioning of the displaced dentition was incomplete. As a result, the patient was in constant distress until seen 12 days later. Fortunately, even at that late stage, correct diagnoses were made and adequate, despite delayed pragmatic management, producing resolution of the signs and symptoms, and a surprisingly favourable outcome was reached. In summary, this case demonstrates that, while the importance of early correct diagnosis and effective management of traumatic dental injuries remains important to optimize the prognosis, delayed effective treatment can still produce decent results.
History
A medically fit and well 22-year-old fell and bit into a solid oak coffee table whilst giving her friend a piggy-back in February 2014. The upper left canine was avulsed and several upper and lower teeth were displaced. She attended her local A&E where the on-call maxillofacial junior member of staff sutured her lacerations, partially replanted the UL3 (extra-oral time in milk = 3 hours) and attempted to reposition the remaining upper and lower anterior teeth. Three days later, she attended another hospital's A&E department as the original splints had debonded. A second attempt was made to reposition the teeth and new splints were placed: the patient was advised to see her dentist for follow-up. The patient saw her dentist who took some radiographs and noted that the teeth were not back correctly in their sockets. They then referred the patient to King's College Hospital where she was seen 12 days after the incident. At this time, the patient was very distressed and initially requested that all her teeth be removed as she was unable to eat and had been in constant pain for all that time.
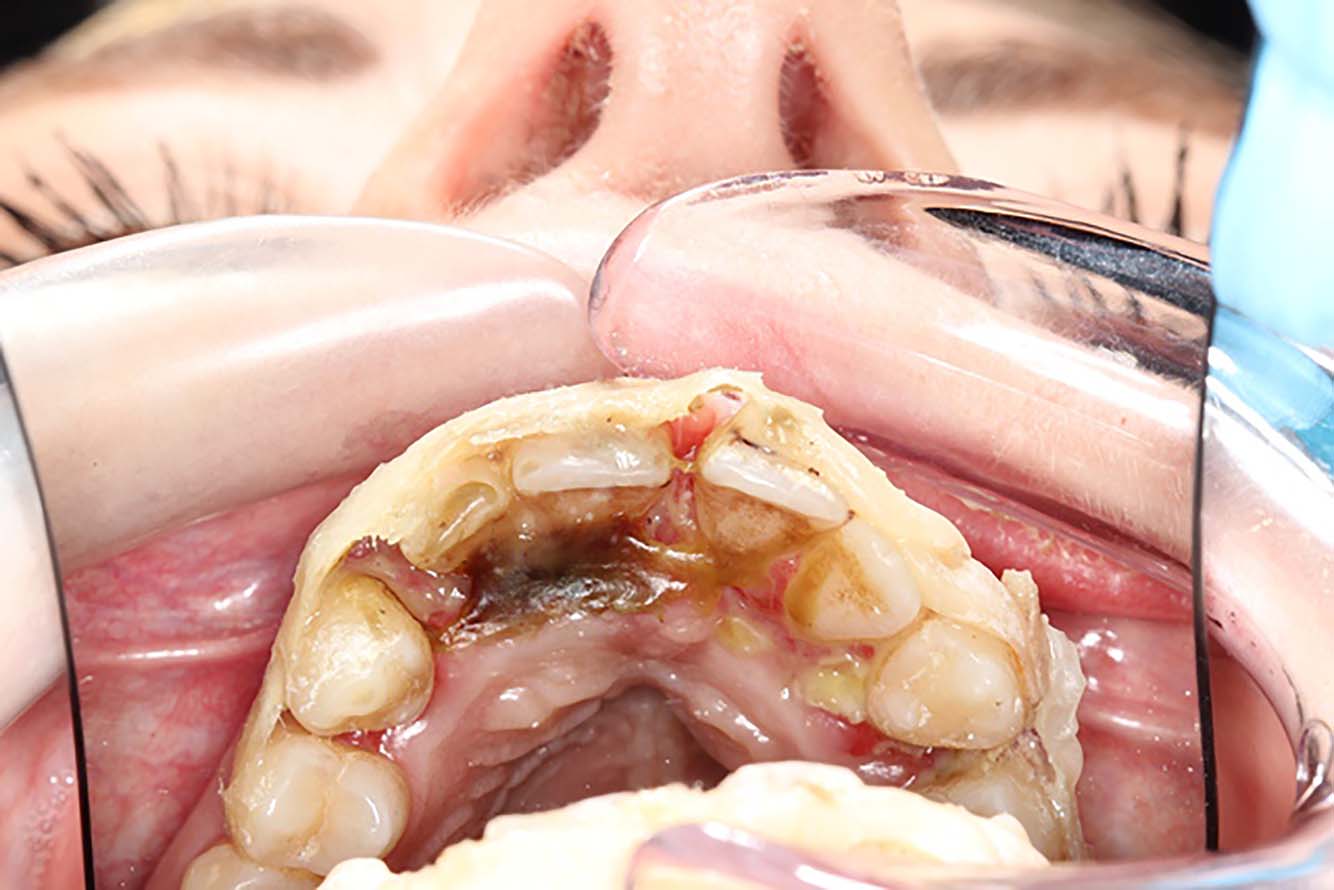
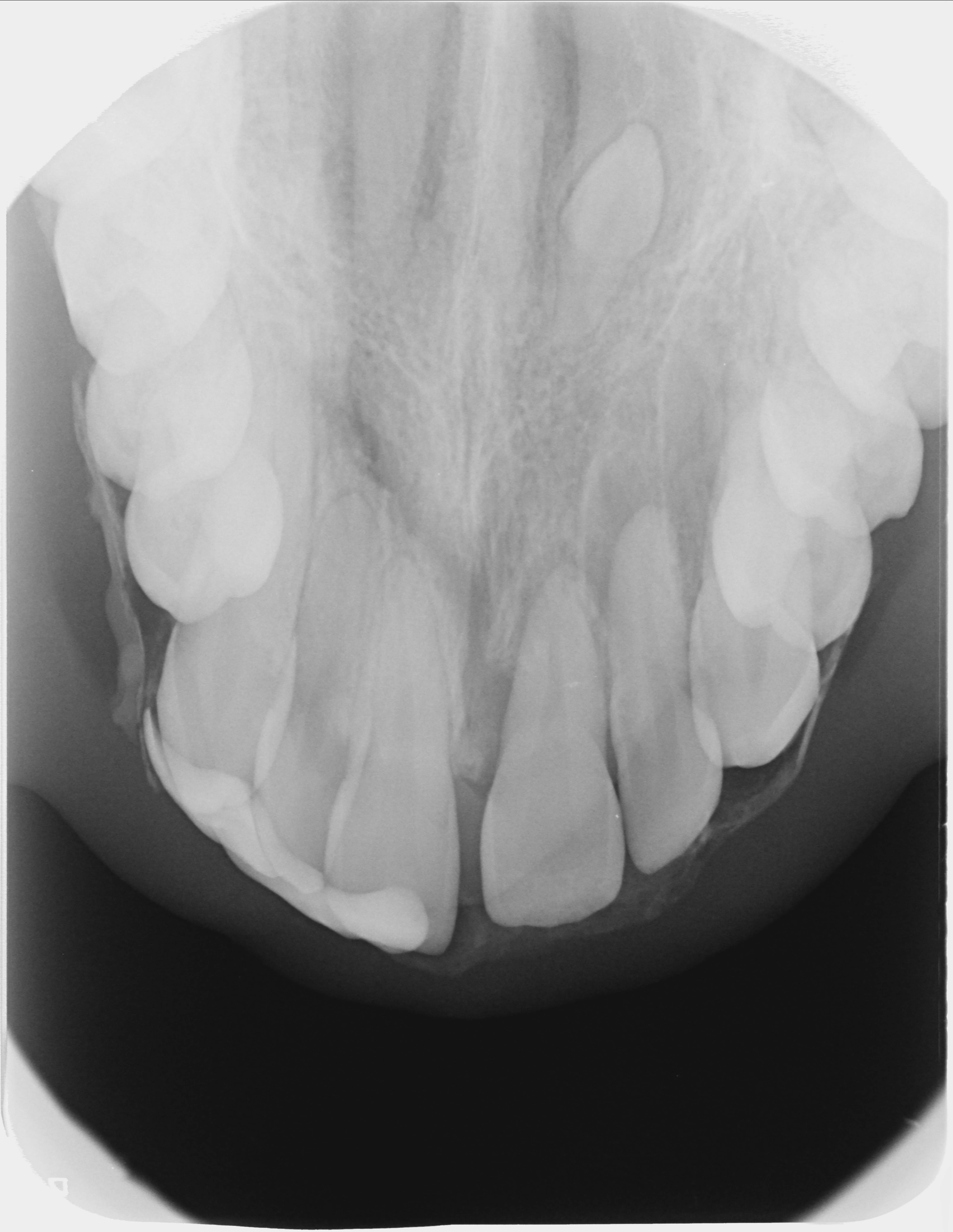
Figure 3.
(a–d) Upper and lower occlusal radiographs and periapical radiographs of UR4,5,4,3 and UL2,3,4,5 at presentation 12 days after the trauma.
Radiographic report
Wide horizontal radiolucent line 2–3 mm beyond apices UR1,2,3 extending to the marginal/alveolar bone;
Socket outline visible UR3, UL1,2,3;
Change in periodontal ligament space UR1,2;
Wide radiolucent line through apices LR2,1, LL1,2 and along the marginal/alveolar bone;
Supernumerary UL3 at level of floor of nose.
Diagnoses
Dento-alveolar fractures of the upper and lower labial segments;
Extrusion UR3,2,1, UL1,2;
Avulsion UL3 (extra-oral time in milk = 3 hours);
Lateral luxation LR2,1, LL1,2.
Prognosis
Due to the length of the extraoral time for the UL3, the patient was advised that the prognosis for this tooth was very poor and was guarded for the UR3,2,1, UL1,2 and fair for the LR2,1 LL1, LL2.
After lengthy discussions about the treatment options and long-term consequences of the trauma, as well as the potential negative impact of the delay in presentation, valid consent was obtained to attempt to reposition the upper and lower anterior teeth and to extirpate the pulp in the UL3.
Treatment strategy
The plan was to reposition the lower incisor teeth first of all. Their incisal edge positions were then to be used to inform the positioning of the upper anterior teeth. The patient said that her teeth were well aligned with no gaps between them. Fortunately, a couple of weeks before her accident, the patient had seen her hygienist and had taken a photo of her teeth on her mobile phone immediately afterwards to see how clean they were. This ‘selfie’ on her phone was used to aid correct repositioning of her upper teeth.
Profound local anaesthesia was achieved using articaine infiltrations placed buccally and lingually/palatally. The lower incisor segment was repositioned with firm pressure from the lingual towards the labial. The teeth were temporarily stabilized in position and a radiograph taken to check that the teeth were adequately repositioned. There was significant resistance to full repositioning of the segment.
The upper teeth were approached methodically and systematically, starting with the UL3 which, when repositioned, was stabilized to the UL4. The UL2 was, in turn, repositioned and temporarily splinted to the UL3, and so on sequentially. Once all the upper anterior teeth had been repositioned, verification radiographs were taken and further tooth repositioning carried out until the best possible result was obtained.
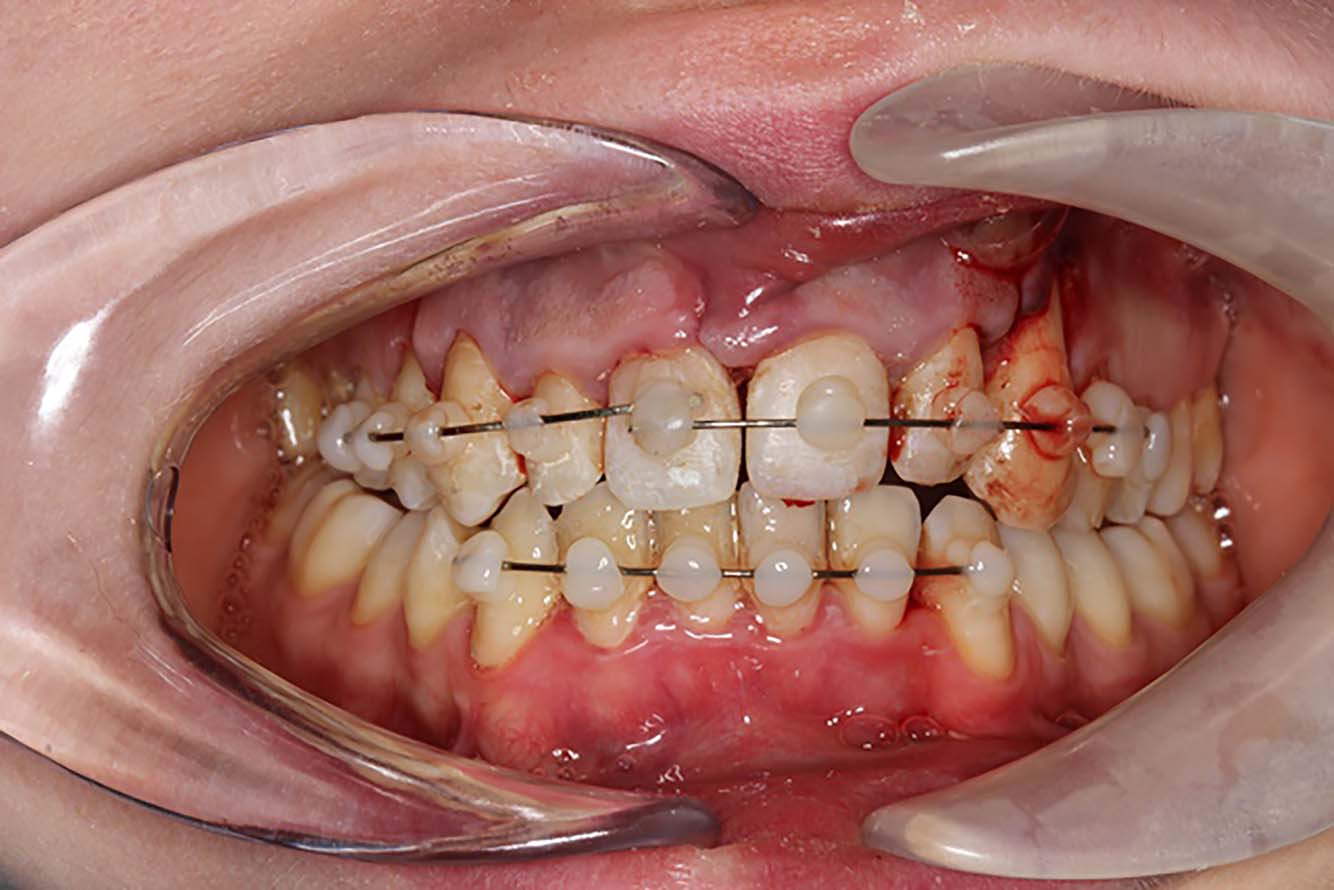
Once the tooth positions were acceptable, flexible splints were placed using 0.18” orthodontic stainless steel wire and composite balls (Figure 4). The final occlusion was checked and was deemed to be reasonable.
Figure 4. Labial view of repositioned and splinted teeth in upper and lower labial sextants.
Post-operative radiographs (Figure 5) revealed good reduction of the dento-alveolar fracture in the lower incisor region and fair repositioning of the upper incisor teeth. There was incomplete repositioning of the upper canine teeth and the patient was made aware of this.
Figure 5.
(a–d) Post-operative radiographs of the repositioned teeth.
The patient was reviewed 2 weeks later to check that healing was progressing reasonably well. The splints were removed 4 weeks after placement when all of the teeth were found to be grade I mobile. As expected, none of the teeth responded to sensibility testing with endo frost or electric pulp testing. At this point root canal treatment of the UL3 was completed.
Three months after the repositioning, the lower incisors did not respond to sensibility testing and the teeth were slightly tender to percussion and palpation. As a result, root canal treatment was also carried out in the LR2,1 LL1, LL2. Apical resorption was noted in the UL1, UL2 and since the UR3,2,1 and the UL1,2 did not respond to sensibility testing, these teeth were root canal treated as well.
Follow-up
By the 6-month review, all of the upper and lower anterior teeth had been root-filled and non-vital bleaching was carried out using 10% carbamide peroxide in trays. The patient was then put on yearly recall.
In November 2016, all appeared well and the patient was delighted with the appearance of her teeth (Figures 6 and 7).
Figure 6. Labial view of the teeth 30 months after the trauma.Figure 7. Occlusal view of the upper teeth 30 months after the trauma.
Radiographs taken 30 months after the initial injury (Figure 8) revealed good infill around the UR3 and UL3 sockets with no signs of apical radiolucencies associated with any of the teeth. The dentoalveolar fractures had healed completely.
Figure 8.
(a–d) Radiographs taken 30 months after the trauma.
Discussion
Comprehensive management of dental trauma is essential for patients' well-being and treatment prognosis. This case demonstrates the management of a young adult patient with delayed presentation of multiple severe traumatic dental injuries.
Whilst she received emergency treatment at two separate hospitals soon after the injury, this was not satisfactory. Appropriate emergency management and treatment planning are essential for improving prognosis.6 The incomplete repositioning of the displaced dentition resulted in both functional and aesthetic problems for the patient. There was a clear disturbance of her occlusion, making speech and eating painful and difficult. As a result, she was distressed to the point where she wanted to have all her teeth out.
Despite the delay in presentation and the two previous failed attempts at repositioning her teeth, the patient was informed of the poor prognosis for her teeth and that, due to the delay in presentation, it might not be possible to achieve complete repositioning. She was also warned that, although the UL3 was placed immediately in milk, owing to the extra-oral time of 3 hours before replantation and the loss of buccal bone, the prognosis for the UL3 was already very poor. She was also informed of the likely sequelae for all the other teeth, including pulp necrosis, discoloration, resorption and possible loss of other teeth.
An avulsion injury is a serious assault to the periodontium, cementum, pulp and dentine.9 The prognosis of an avulsed tooth is dependent on the actions taken at the time of injury and immediate replantation is the treatment of choice when feasible to maintain viability of the cells of the periodontal ligament.6 Alternatively, the tooth may be placed in a physiologic medium such as Hank's balanced salt solution, milk, saline, or saliva and the total extra-oral dry time should not exceed 60 minutes.8 According to previous authors, the length of the extraoral dry time was found to be the most critical factor related to post-replantation root resorption.9 In this case, that meant that the prognosis of the avulsed UL3 was poor due to the extended extra-oral dry time and the traumatic position in which it had been placed for 12 days. Interestingly, in this case, the UL3 remained functional and, although somewhat discoloured and lacking attached gingiva, it remained problem free throughout the entire follow-up period. The tooth was asymptomatic and firm, although there was 7 mm recession.
Radiographic presentation revealed no evidence of resorption and the lamina dura appeared normal. All these findings indicate a favorable outcome, as outlined in the International Association of Dental Traumatology guidelines.8
The prognosis for the upper anterior dentition was considered guarded. The marked displacement of the dentition, along with the concomitant dento-alveolar fracture, damaged the periodontal ligament and the supporting structures, thus increasing the risk of resorption.9 The effect of treatment delay on the prognosis of luxation injuries remains uncertain. Some authors found a decline in periodontal ligament healing following 5 hours, while others reported reduced healing after 33 hours. Therefore, it is recommended that management of the trauma should be carried out as soon as feasible within the first 24 hours, particularly for relief of the clinical symptoms.4
The patient presented with a debonded flexible splint. Adequate splinting is important for preserving the correct position of the repositioned dentition, maintaining patient comfort, improving function and preventing further injury to the pulp and periodontal ligament.3 In this case, following repositioning, a short-term flexible splint, which allowed physiologic movement of the teeth, was placed as advised in current existing evidence and guidelines.3,8 The slight motion along with short splinting time may promote periodontal and pulpal healing and allow functional stimulation of the periodontium.8
Fortunately, the patient had a ‘selfie’ of her dentition prior to the injury on her phone. The photograph was invaluable in guiding the repositioning of multiple teeth. Every effort was made to reposition the teeth as seen in the photograph and an acceptable result was achieved.
Sensibility testing was not considered at the initial presentation as transient loss of pulpal response may occur immediately after the dental injury.3,6 Therefore, regular follow-up was needed to get the pulpal diagnosis of the teeth and at least two signs and symptoms were necessary to diagnose pulp necrosis as recommended by previous authors.3
Finucane and Kinirons described the management of extrusive luxation and avulsion in a 10-year old boy.9 In that case, the luxated tooth was repositioned within 45 minutes, which was different from our case as repositioning was carried out 12 days after the injury. In contrast to this case, they reported a poor outcome due to poor patient attendance which was not the case reported here.
Overall, given the inadequate early treatment at two previous A&E departments, a surprisingly favourable outcome was achieved for this patient. High patient satisfaction was attained along with clinical and radiographic healing of the injuries, despite the initial assessment being that the very badly damaged teeth had a questionable prognosis.
No signs of resorption were evident radiographically at the 30 months' review. Previous authors have reported that the risk of resorption is greatly reduced if it was not detected within 2 years following the injury.9
Conclusion
Patient ‘selfies’ of close-ups of their teeth are very useful in cases of trauma. Patients should be routinely asked if they have any selfies showing their teeth on their mobile phones if they sustain dental injuries as a guide to help repositioning of their teeth.
Further repositioning of incompletely repositioned teeth, particularly when there is a delay in presentation, should be considered a serious complication in acute management of trauma.
Treatment of traumatic dental injuries remains a challenge owing to often complex diagnosis, particularly in emotionally distressed patients. Every effort should be made to manage traumatic dental injuries early and effectively in local A&E departments. Further training in this important area is to be encouraged in such departments and appropriate treatment guides can be downloaded from www.dentaltrauma.co.uk
In the case of delayed presentations, patients should be informed that further repositioning can be attempted but might not be successful. However, even then some attempts should be made to try to help these unfortunate patients.