Caufield PW, Li Y, Bromage TG. Hypoplasia-associated severe early childhood caries – a proposed definition. J Dent Res. 2012; 91:544-550
Welbury R, Duggal M, Hosey MT. Paediatric Dentistry, 4th edn. Oxford: Oxford University Press; 2012
Atia GS, May J. Dental fluorosis in the paediatric patient. Dent Update. 2013; 40:836-839
Visram S, McKaig S. Amelogenesis imperfecta – clinical presentation and management: a case report. Dent Update. 2006; 33:612-616
Salanitri S, Seow WK. Developmental enamel defects in the primary dentition: aetiology and clinical management. Aust Dent J. 2013; 58:133-140
Slayton RL, Warren JJ, Kanellis MJ, Levy SM, Islam M. Prevalence of enamel hypoplasia and isolated opacities in the primary dentition. Pediatr Dent. 2001; 23:32-36
Montero MJ, Douglass JM, Mathieu GM. Prevalence of dental caries and enamel defects in Connecticut head start children. Pediatr Dent. 2003; 25:235-239
Purvis RJ, MacKay GS, Barrie WJ Enamel hypoplasia of the teeth associated with neonatal tetany: a manifestation of maternal vitamin D deficiency. The Lancet. 1973; 2:811-814
Lai PY, Seow WK, Tudehope DI, Rogers Y. Enamel hypoplasia and dental caries in very-low birthweight children: a case-controlled, longitudinal study. Pediatr Dent. 1997; 19:42-49
Correa-Faria P, Martins-Junior PA, Vieira-Andrade RG, Oliveira-Ferreira F, Marques LS, Ramos-Jorge ML. Developmental defects of enamel in primary teeth: prevalence and associated factors. Int J Paediatr Dent. 2013; 23:173-179
Correa-Faria P, Ferreira RC Association between molar incisor hypomineralisation in schoolchildren and both prenatal and postnatal factors: a population based study. PLoS. 2016; 11
Ford D, Seow WK, Kazoullis S, Holcombe T, Newman B. A controlled study of risk factors for enamel hypoplasia in the permanent dentition. Pediatr Dent. 2009; 31:382-388
Whatling R, Fearne JM. Molar incisor hypomineralization: a study of aetiological factors in a group of UK children. Int J Paediatr Dent. 2008; 18:155-162
Ghanim A, Manton D, Marino R, Morgan M, Bailey D. Prevalence of demarcated hypomineralisation defects in second primary molars in Iraqi children. Int J Paediatr Dent. 2013; 23:48-55
Casanova-Rosado AJ, Medina-Solis CE, Casanova-Rosado JF Association between developmental enamel defects in the primary and permanent dentition. Eur J Paediatr Dent. 2011; 12:155-158
Mittal N, Sharma BB. Hypomineralised second primary molars: prevalence, defect characteristics and possible association with Molar Incisal Hypomineralisation in Indian children. Eur Archiv Paediatr Dent. 2015; 16:441-447
Ghanim A, Elfrink M, Weerheijm K, Marino R, Manton D. A practical method for use in epidemiological studies on enamel hypomineralisation. Eur Archiv Paediatr Dent. 2015; 16:235-246
Davit-Beal T, Gabay J, Antoniolli P, Wolikow M. Dental complications of rickets in early childhood: case report on 2 young girls. Pediatrics. 2014; 133::e1077-e1081
Vargas-Ferreira F, Salas MMS, Nascimento GG Association between developmental defects of enamel and dental caries: a systematic review and meta-analysis. J Dent. 2015; 43:619-628
Feigal RJ. The use of pit and fissure sealants. Pediatr Dent. 2002; 24:415-422
Kotsanos N, Kaklamanos EG, Arapostathis K. Treatment management of first permanent molars in children with Molar-Incisor Hypomineralisation. Eur J Paediatr Dent. 2005; 6:179-184
Kandiah T, Johnson J, Fayle S. British Society of Paediatric Dentistry: a policy document on management of caries in the primary dentition. Int J Paediatr Dent. 2010; 20
Lygidakis NA, Chaliasou A, Siounas G. Evaluation of composite restorations in hypomineralised permanent molars: a four year clinical study. Eur J Paediatr Dent. 2003; 4:143-148
Venezie RD, Vadiakas G, Christensen JR, Wright JT. Enamel pretreatment with sodium hypochlorite to enhance bonding in hypocalcified amelogenesis imperfecta: case report and SEM analysis. Pediatr Dent. 1994; 16:433-436
Kindelan SA, Day P, Nichol R, Willmott N, Fayle SA UK National Clinical Guidelines in Paediatric Dentistry: stainless steel preformed crowns for primary molars. Int J Paediatr Dent. 2008; 18:20-28
Rogers HJ, Batley HA, Deery C. An overview of preformed metal crowns Part 1: conventional techniques. Dent Update. 2015; 42:933-938
Ludwig KH, Fontana M, Vinson LA, Platt JA, Dean JA. The success of stainless steel crowns placed with the Hall Technique. A retrospective study. J Am Dent Assoc. 2014; 145:1248-1253
Innes N, Evans DJ, Stirrups DR. The Hall Technique; a randomized controlled clinical trial of a novel method of managing carious primary molars in general dental practice: acceptability of the technique and outcomes at 23 months. BMC Oral Health. 2007; 7
Rodd HD, Waterhouse PJ, Fuks AB, Fayle SA, Moffat MA. UK National Guidelines in Paediatric Dentistry. Pulp therapy for primary molars. Int J Paediatr Dent. 2006; 16:15-23
The Clinical Effectiveness Committee of The Faculty of Dental Surgery of The Royal College of Surgeons of England. Extraction of primary teeth – balance and compensation. 2001;
National Institute for Clinical Excellence. Dental checks: intervals between oral health reviews. 2004. https://www.nice.org.uk/guidance/cg19 (Accessed May 2016)
Developmental defects of enamel (DDE) are not uncommon in both the primary and permanent dentition. This article presents a review of the current literature and describes the definition, prevalence, aetiology, diagnosis and management of primary molars affected by DDE.
CPD/Clinical Relevance: This article describes the diagnosis and management of DDE in practice to aid treatment planning in children with primary molars affected by DDE.
Article
Definition, prevalence and aetiology
Historically, a collection of terms and definitions have been used to describe various developmental defects of the enamel (DDEs). DDEs are classified as demarcated opacities, diffuse opacities and hypoplasia.1 Clinicians have intermixed these terms in attempting to describe the clinical findings.
Hypoplasia is a quantitative defect of enamel caused by disturbances in the secretory phase of amelogenesis. During the secretory phase, enamel crystals grow in length creating the enamel thickness.2 Hypoplasia presents clinically as pitting, grooving or absence of enamel.
Hypomineralization, by contrast, is a qualitative defect of enamel and occurs due to disturbances in the maturation phase of amelogenesis. Enamel maturation is a slow developmental process, with two-thirds of the time needed for crown formation being used for this phase.3 During this phase, proteases remove the organic material as mineralization continues.4 Hypomineralization presents as enamel with a soft, chalky or cheesy appearance and can vary in colour from white to yellow or brown. A clear demarcation can usually be seen between the affected and non-affected enamel.5
It is important to differentiate between hypoplasia and hypomineralization in order to provide tailored care for patients affected by either condition. Molar incisor hypomineralization (MIH) describes enamel hypomineralization affecting one or more permanent molars, which is frequently associated with affected incisors.6 Hypomineralized second primary molars (HSPM) refers only to second primary molars which are affected by hypomineralization. In 2012, Caufield classified the concomitant presence of enamel hypoplasia and severe early childhood as hypoplasia-associated severe early childhood caries (HAS-ECC).7
DDE also includes fluorosis and amelogenesis imperfecta. Fluorosis can present in mild forms as diffuse opacities or mottling of the enamel and, in more severe cases, as marked opacities, discoloration, pitting and enamel hypoplasia.8 It presents in a chronological manner in accordance with increased fluoride ingestion. Amelogenesis imperfecta (AI) is a genetic condition resulting in hypomature, hypocalcified or hypoplastic enamel. AI should be suspected if the entire primary and permanent dentition is affected and often the permanent dentition is more severely affected. Parents of children with AI may also report a positive family history. This article does not discuss the management of fluorosis and amelogenesis imperfecta. Information on the management of these specific conditions can be obtained in previous Dental Update articles.9,10
The prevalence of DDE affecting the primary molar teeth has been reported from between 6–49% in studied populations with the second primary molars most often affected.11,12,13 There are several aetiological factors associated with DDE which can be acquired, systemic, local or hereditary. Hypoplasia and hypomineralization in the primary dentition has been linked with maternal vitamin D deficiency,14 low birth weight15,16 and asthma or bronchitis in the first four years of life.17 Hypoplasia and hypomineralization in the permanent dentition has been linked with; difficulties during pregnancy or labour, exposure to cigarette smoking, ear infections, urinary tract infections, chicken pox and respiratory infections in infancy.18,19 Recent studies have shown a relationship between MIH and DDE of the primary molars suggestive of a common aetiology. Ghanim et al found that 40% of patients with HSPMs had at least one first permanent molar which was affected by hypomineralization.20 Casanova-Rosado et al also found that, for each primary tooth with DDE, the odds of a permanent tooth also having a DDE increased 1.38 times.21 More recently, Mittal and Sharma observed concomitant presence of MIH in 32.7% of children affected by HSPM. Furthermore, the authors found that children affected by HSPM always had a higher odds ratio of MIH regardless of the severity of the HSPM (ie whether post-eruptive breakdown was present or absent).22 This link between DDE in primary teeth and DDE in the permanent dentition is thought to be due to the temporal proximity of development of the primary molars and the first permanent molars and permanent incisors.23Figure 1 shows an example of a child in the mixed dentition with DDE of the ULE and MIH affecting the maxillary permanent incisors and first permanent molars.
Figure 1. MIH affecting the UR1, UR6, UL1, UL6 in a child who also has hypomineralization of the ULE.
Diagnosis
A comprehensive medical, dental and family history should be taken to identify the specific type of DDE and exclude other dental diagnoses, including white spot lesions. White spot lesions can be differentiated from DDE as they generally appear at contact points or gingival margins, and are commonly associated with plaque deposits.4 Children with vitamin D deficiency rickets present with enamel hypoplasia (ie grooving/pitting or loss of enamel as defined earlier), which appears to affect teeth in a chronological manner.24 DDE in primary molars may be under-reported due to breakdown of these teeth, resulting in only a diagnosis of caries being given.
Screening of a child's teeth should start by the age of 12 months to allow for early detection of DDE on eruption of the teeth and to assess dental disease risk.25 In order to assess the teeth, they should be cleaned to remove debris and plaque and examination should be under standard clinical operatory lights.4 Ghanim et al suggested a method for the recording of DDE in the permanent and primary dentition for application in epidemiological and clinical studies.23 Their recommendations included: not scoring any tooth where less than a third of the crown had erupted and any DDE less than 1 mm in diameter was not considered. Regarding primary molars, the authors recommended that the clinical status of the tooth is recorded. The details of which should include:
The presence of any DDE;
The type of DDE (ie diffuse opacities, demarcated opacities or hypoplasia);
The colour of the DDE;
The presence of any post-eruptive breakdown (PEB) or atypical restorations;
An atypical pattern of caries;
If a primary molar has been lost due to DDE (this may be difficult to confirm from the dental history);
If breakdown of the tooth is so extensive it is impossible to identify the cause of breakdown.
Primary molars identified as being affected by DDE should then be further graded according to the amount of the tooth affected (Figure 2):
Less than 1/3 of the tooth affected;
At least 1/3 but less than 2/3 of the tooth affected;
Greater than 2/3 of the tooth affected.
Figure 2. (a) A grade I, white, demarcated opacity on the mesiopalatal cusp of the URE. (b) A grade II, yellow, demarcated opacity on the occlusal and buccal surface of the LLE with minimal PEB buccally. (c) A grade III, yellow-white demarcated opacity on the occlusal-buccal-lingual surface of the LRE with an atypical restoration present. (d) A grade III, yellow-white, demarcated opacity of the ULE with atypical caries and extensive PEB resulting in gingival overgrowth. All four images were taken from the same patient demonstrating the variation of presentation of DDE in one patient.
DDE in the primary dentition may be less apparent owing to the relative white appearance of the primary teeth compared to permanent teeth. Tooth surface loss may also cause difficulty in diagnosing enamel defects.4 However, the clinician should endeavour to record as much of the information listed previously as possible as this can lead to appropriate management for these teeth. Bitewing radiographs should be attempted to assess for dental caries and are valuable in treatment planning of the affected teeth.
Management
Early diagnosis and caries prevention is essential in children with DDE in their primary molars as they have an increased risk of developing dental caries.7,11 Correct diagnosis will aid assessment of caries risk and guide treatment planning of restorations and counselling of parents regarding the risk of DDE affecting the permanent dentition. A recent meta-analysis has also shown a positive association between enamel defects and dental caries in the permanent dentition.26 When extrapolating this relationship to the primary dentition, parents should be informed of the increased risk of caries in primary molars affected by DDE and given caries prevention advice suitable for children of high caries risk. This should include oral hygiene instruction with the use of toothpaste with an appropriate amount of fluoride for the patient's age and caries risk, diet advice, professional fluoride application and fluoride toothpaste prescription, where necessary. This is in accordance with the Public Health England document Delivering better oral health: an evidence-based toolkit for prevention.27 Risk of dental disease for all children should be documented and reviewed at subsequent appointments to guide management.
Given the link between DDE in primary teeth and increased risk of DDE in the permanent dentition, it would be prudent to warn parents that DDE in the primary dentition may be an indicator that the permanent dentition may also be affected.
The clinician should consider the patient experience throughout treatment, taking care to avoid negative experiences which may lead to anxieties regarding treatment when the child is older. In order to increase patient comfort, adequate local anaesthesia should be provided, where possible, when carrying out procedures which may elicit sensitivity or discomfort if local anaesthetic were not used. Avoidance of air drying teeth which are not anaesthetized is advised to reduce the risk of causing sensitivity during examination. As an alternative, teeth can be dried with cotton wool or gauze.
When administering local anaesthetic in children, clinicians should take care to deliver pain-free anaesthetic. This can be achieved by application of topical anaesthetic onto clean, dry mucosa. This must be left in situ for at least one minute before delivery of the anaesthetic solution. The anaesthetic solution should be delivered slowly using a short needle, first with buccal infiltration, followed by interpapillary infiltration to anaesthetize the lingual/palatal mucosa, if this is required. A description of this technique with accompanying images is available from the Scottish Dental Clinical Effectiveness Programme document Prevention and management of dental caries in children.28 New computer-controlled delivery devices can be used to deliver local anaesthetic slowly and reduce pain associated with this procedure. Clinicians must be aware of dose limits for local anaesthetic agents in children.
Sensitivity
Children may present to their general dental practitioner (GDP) initially complaining of sensitivity from a primary molar affected by DDE. Initial management should aim to relieve any discomfort. The following methods have been suggested for relief of sensitivity in hypomineralized permanent teeth and should be considered in the management of the same concerns in primary teeth. These include:
Use of sensitive toothpaste or toothpastes containing 0.4% stannous fluoride;31 and
The daily use of casein phosphopeptide-amorphous calcium phosphate (ie GC Tooth Mousse®).29,30
During toothbrushing, the use of warm water can minimize sensitivity.11 Where topical treatment of sensitivity is unsuccessful, or where there is post-eruptive breakdown of teeth, with or without caries present, sealants or restorations are required.
Sealants
As hypomineralized primary molars are at increased risk of developing dental caries, fissure sealants should be considered for the management of affected primary molars with intact enamel.32
When an affected primary molar is erupting, it can be provided with a glass ionomer cement (GIC) sealant until eruption. The GIC sealant will promote remineralization, prevent caries formation, and provide relief of any symptoms that the patient may be experiencing.
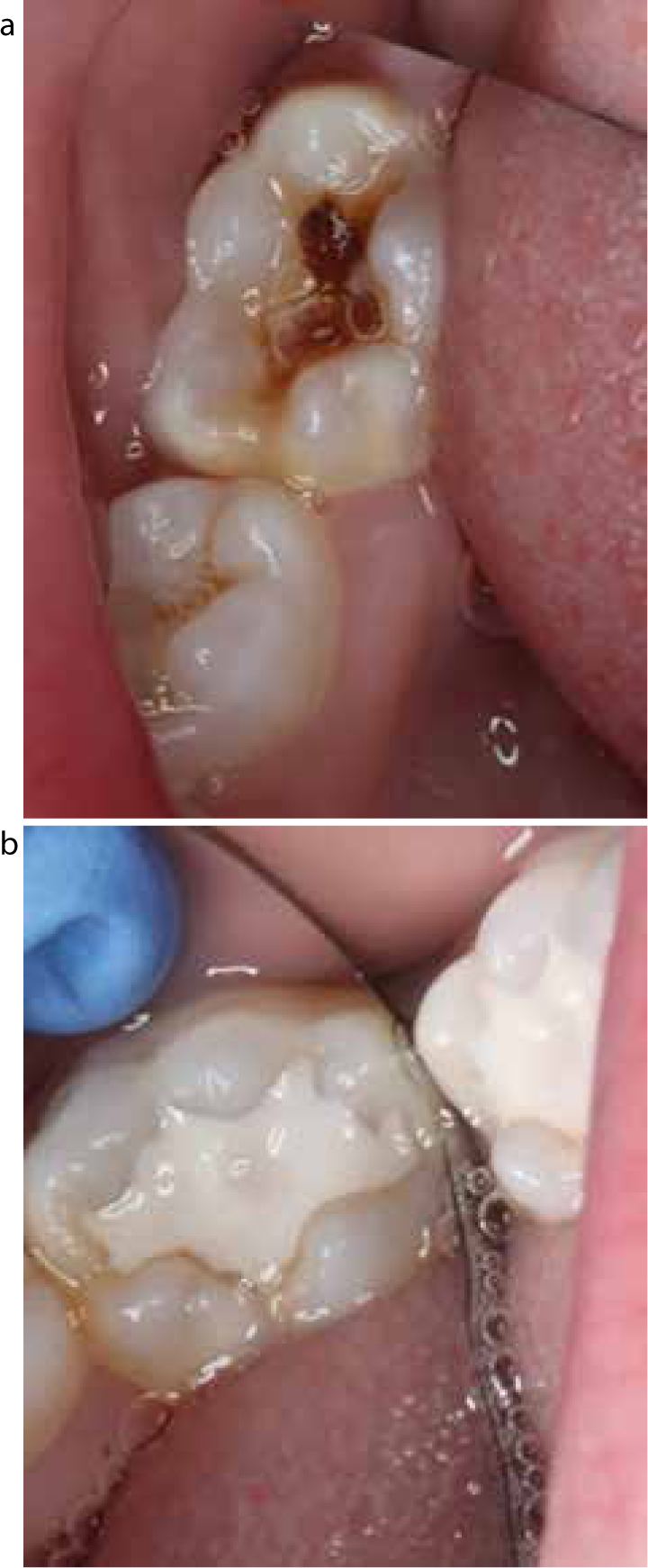
Primary molars affected by DDE which are fully erupted, with no post-eruptive breakdown, can be managed conservatively with resin-based sealant restorations. Optimal conditions for fissure sealant placement will increase longevity. Fissure sealants require adequate moisture control and ideally would be placed under rubber dam conditions. This would require the use of local anaesthetic for patient comfort and to minimize tooth sensitivity during the procedure. If resin-based sealants regularly fail, or if moisture control is suboptimal, GIC sealants are preferable.29 If the patient continues to experience sensitivity, preformed metal crowns should be considered. Figure 3 shows a primary molar affected by DDE and sealed occlusally with GIC.
Figure 3. (a, b) The LLE affected by DDE and sealed with GIC.
When comparing MIH-affected permanent molars to unaffected permanent molars, a greater failure rate of fissure sealants is seen in teeth affected by MIH.33 This is due to the reduced bond strength resulting from the poorer quality enamel in cases of hypomineralization. For this reason, fissure sealants should be reviewed regularly and maintained. Strategies to improve the bond strength of resin-based restorations are discussed in the next section.
Restorations
Where there is breakdown of primary molars affected by DDE or cavitated carious lesions associated with these teeth, restoration is required. Clinicians will need to make a decision regarding the most appropriate restorative material to use. This will depend on several factors, including: patient cooperation level; patient and guardian preferences for the type of restorative material; and the skill and experience of the clinician providing the treatment. There is limited published evidence regarding outcomes of restorations placed in primary molars with DDE. Much of the evidence used in this section refers to the management of permanent molars with MIH and has been extrapolated to apply to the management of primary molars with DDE in view of the lack of available evidence in this area.
Amalgam restorations should be avoided in the management of DDE in primary molars. This material is a poor insulator, non-adhesive, requires less conservative preservation of tooth tissue, and has a higher failure rate compared to composite restorations or preformed metal crowns.33 Furthermore, recent EU legislation has prohibited the general use of amalgam in primary teeth and in children under the age of 15 after July 2018.34
Glass ionomer cement (GIC) bonds to dentine and is a good insulator. It does, however, have poor wear resistance31 and is susceptible to acid dissolution. GIC does have the added benefit of releasing fluoride, and being less technique sensitive than composite. It can be considered for temporization of primary molars with DDE given its ease of use, particularly where moisture control is compromised.29 Temporization with GIC can allow time for acclimatization of the patient until cooperation improves to allow for composite or preformed metal crown restoration.
Composite restorations in the primary dentition can be considered for small one and two surface cavities and placement should ideally be carried out using local anaesthetic and rubber dam.31,35 Lygidakis et al showed full retention of all composite restorations in hypomineralized permanent molars (with no more than two surfaces affected) after 4-year follow-up when composite was placed under ideal clinical conditions.36 Enamel pre-treatment with sodium hypochlorite has been suggested to improve the bond of composite to permanent teeth affected by DDE.29,37 In a single case study, a 5% sodium hypochlorite pre-treatment of enamel affected by amelogenesis imperfecta (AI) showed improved bonding to enamel. This is thought to be due to deproteinating and exposing the enamel mineral, which is encased in acid-insoluble proteins. The method used was as follows: teeth were cleaned with pumice and rinsed with water, 5% sodium hypochlorite was applied to the tooth with a brush for one minute. The tooth was then rinsed and air dried prior to placement of the composite restoration using separate etch and bond stages.37 This method has not been reported for use in primary molars affected by DDE. If this was to be considered, use of rubber dam isolation would be essential to protect the soft tissues.
Preformed metal crowns (PMCs) are the restoration of choice for primary molars affected by DDE with multi surface cavitation or post-eruptive breakdown. They provide a complete seal over the primary molar, protecting it from further breakdown.12 PMCs are indicated in primary molars affected by localized or generalized developmental problems, as stated in Royal College of Surgeons of England guidance.38 This guidance describes in detail the procedural steps for placement of conventional PMCs on primary molars. The authors of this guidance stress the importance of good adaptation of the distal margin of second primary molars to avoid impaction of the first permanent molars if they are not erupted at the time of PMC placement. Readers are also directed to a Dental Update article which describes, with images, conventional PMC placement.39
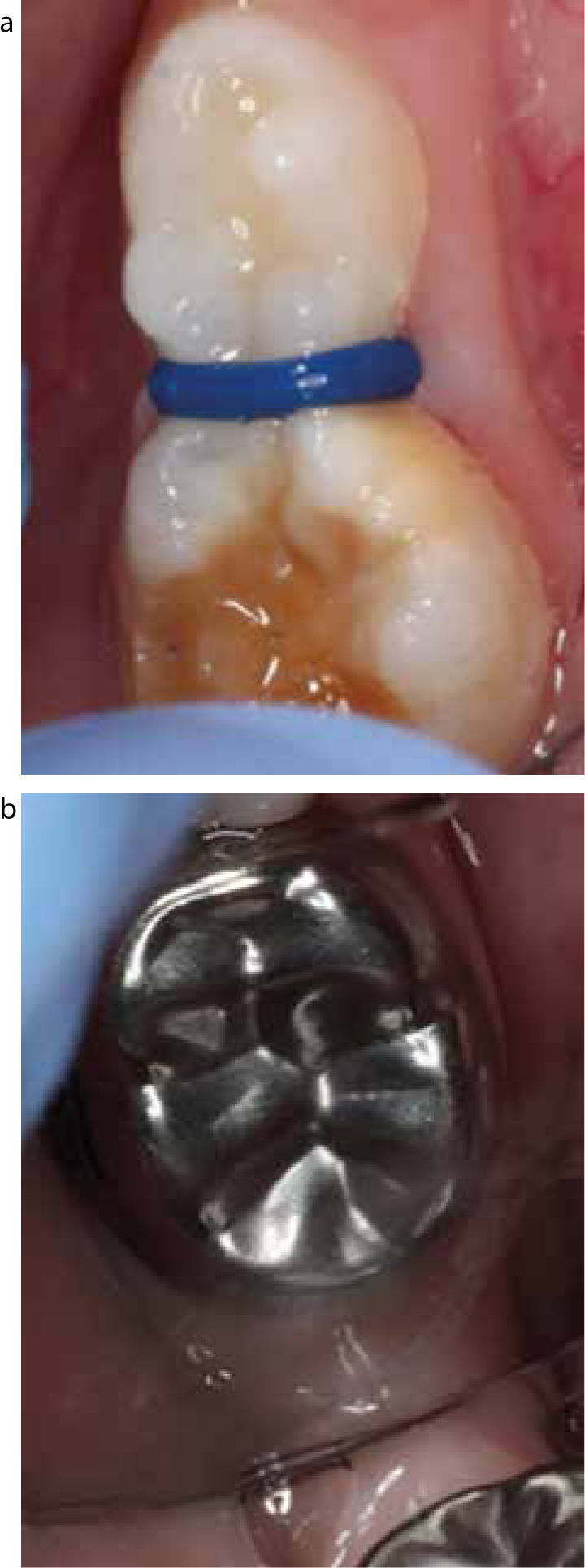
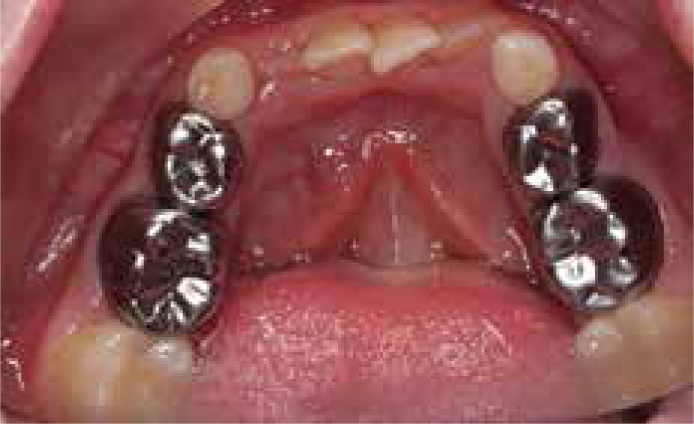
PMCs can also be provided using the Hall Technique. This is a minimally invasive technique for PMC placement which requires no tooth preparation or anaesthetic. Hall technique PMCs are indicated for occlusal lesions if the patient is unable to accept a sealant or composite restoration, or to restore proximal or multisurface cavities where conventional PMC placement may be difficult due to limited patient cooperation.40 Readers are directed to previous Dental Update articles related to the use of the Hall Technique for procedural tips, with images, when using this technique.41,42 A 2015 Cochrane review found that PMCs placed on primary molar teeth are likely to reduce the risk of major failure in the long term, compared to plastic restorations.43 Both conventional and Hall Technique PMCs have excellent long-term success rates of 94%44 and 95%,45 respectively. Figures 4 and 5 demonstrate the use of PMCs in the management of DDE in primary molars.
Figure 4. (a) Placement of an orthodontic separator mesial to the LRE in a 4-year-old with DDE or the LRE one week prior to the placement of a PMC using the Hall Technique. (b) The same tooth following placement of the PMC.Figure 5. Post-operative view following placement of preformed metal crowns on the LLE, LLD, LRE and LRD to manage DDE using the Hall Technique.
Extraction
In cases where a primary molar is affected by DDE with associated periapical pathology, draining sinus or facial swelling, or where the tooth would be unrestorable after pulp therapy, extraction is indicated.46 Those children in whom a primary molar is removed in an otherwise healthy arch, with good oral hygiene, could benefit from space maintenance in the following scenarios:
Loss of a primary first molar where crowding is severe, ie more than 3.5 mm (half a unit) per quadrant.
Loss of a primary second molar, except in spaced arches.
The details of space maintenance design which can be used are described in the Royal College of Surgeons of England guideline, from which this advice is taken.47
Review
Children should be reviewed every 3 months if they have high dental disease risk with a maximum recall interval of no greater than 6 months. Individual factors related to disease risk should tailor recall interval.48 Radiographic review of primary molars with DDE should be carried out according to caries risk in line with the Faculty of General Dental Practitioners (FGDP) guidelines.49
Summary
In order to manage DDE in primary molars, a practitioner must first correctly diagnose the type of condition based on a comprehensive medical, family and dental history. An assessment of disease risk should be made, the same as for any patient, in order to tailor disease prevention advice.
When treatment planning, the clinician will need to consider the dental diagnosis, disease risk, cooperation level of the patient, and acceptability of dental materials, as discussed with patients and their guardians. A period of temporization and acclimatization may be required in order to provide young children with the best possible treatment.
Consideration should be given to the long-term prognosis and restorability of the tooth, along with the child's ability to cope with treatment. Where there is a hopeless prognosis or lengthy treatment would be required to restore the affected teeth in a pre-cooperative child, clinicians should consider if extraction would be more appropriate than restoration.
Review is essential for all paediatric patients and especially those with previous dental concerns or increased disease risk.
Conclusion
Children with DDE in primary molars should be provided with a tailored treatment plan, to include disease prevention and management of the affected primary molars, as detailed in this article. For cooperative children, this treatment can be provided in general dental practice. Those children who are pre- or potentially cooperative may require treatment within a specialist setting, where inhalation sedation can be considered to aid treatment delivery. In some cases, general anaesthetic may have to be considered and should be treatment planned by a specialist in paediatric dentistry.
Given the limited evidence available on the topic of DDE in primary molars, particularly regarding outcomes of treatment, this would be an interesting area for the development of research studies.